Have a language expert improve your writing
Run a free plagiarism check in 10 minutes, generate accurate citations for free.
- Knowledge Base
Methodology
- Longitudinal Study | Definition, Approaches & Examples

Longitudinal Study | Definition, Approaches & Examples
Published on May 8, 2020 by Lauren Thomas . Revised on June 22, 2023.
In a longitudinal study, researchers repeatedly examine the same individuals to detect any changes that might occur over a period of time.
Longitudinal studies are a type of correlational research in which researchers observe and collect data on a number of variables without trying to influence those variables.
While they are most commonly used in medicine, economics, and epidemiology, longitudinal studies can also be found in the other social or medical sciences.
Table of contents
How long is a longitudinal study, longitudinal vs cross-sectional studies, how to perform a longitudinal study, advantages and disadvantages of longitudinal studies, other interesting articles, frequently asked questions about longitudinal studies.
No set amount of time is required for a longitudinal study, so long as the participants are repeatedly observed. They can range from as short as a few weeks to as long as several decades. However, they usually last at least a year, oftentimes several.
One of the longest longitudinal studies, the Harvard Study of Adult Development , has been collecting data on the physical and mental health of a group of Boston men for over 80 years!
Prevent plagiarism. Run a free check.
The opposite of a longitudinal study is a cross-sectional study. While longitudinal studies repeatedly observe the same participants over a period of time, cross-sectional studies examine different samples (or a “cross-section”) of the population at one point in time. They can be used to provide a snapshot of a group or society at a specific moment.

Both types of study can prove useful in research. Because cross-sectional studies are shorter and therefore cheaper to carry out, they can be used to discover correlations that can then be investigated in a longitudinal study.
If you want to implement a longitudinal study, you have two choices: collecting your own data or using data already gathered by somebody else.
Using data from other sources
Many governments or research centers carry out longitudinal studies and make the data freely available to the general public. For example, anyone can access data from the 1970 British Cohort Study, which has followed the lives of 17,000 Brits since their births in a single week in 1970, through the UK Data Service website .
These statistics are generally very trustworthy and allow you to investigate changes over a long period of time. However, they are more restrictive than data you collect yourself. To preserve the anonymity of the participants, the data collected is often aggregated so that it can only be analyzed on a regional level. You will also be restricted to whichever variables the original researchers decided to investigate.
If you choose to go this route, you should carefully examine the source of the dataset as well as what data is available to you.
Collecting your own data
If you choose to collect your own data, the way you go about it will be determined by the type of longitudinal study you choose to perform. You can choose to conduct a retrospective or a prospective study.
- In a retrospective study , you collect data on events that have already happened.
- In a prospective study , you choose a group of subjects and follow them over time, collecting data in real time.
Retrospective studies are generally less expensive and take less time than prospective studies, but are more prone to measurement error.
Like any other research design , longitudinal studies have their tradeoffs: they provide a unique set of benefits, but also come with some downsides.
Longitudinal studies allow researchers to follow their subjects in real time. This means you can better establish the real sequence of events, allowing you insight into cause-and-effect relationships.
Longitudinal studies also allow repeated observations of the same individual over time. This means any changes in the outcome variable cannot be attributed to differences between individuals.
Prospective longitudinal studies eliminate the risk of recall bias , or the inability to correctly recall past events.
Disadvantages
Longitudinal studies are time-consuming and often more expensive than other types of studies, so they require significant commitment and resources to be effective.
Since longitudinal studies repeatedly observe subjects over a period of time, any potential insights from the study can take a while to be discovered.
Attrition, which occurs when participants drop out of a study, is common in longitudinal studies and may result in invalid conclusions.
Receive feedback on language, structure, and formatting
Professional editors proofread and edit your paper by focusing on:
- Academic style
- Vague sentences
- Style consistency
See an example

If you want to know more about statistics , methodology , or research bias , make sure to check out some of our other articles with explanations and examples.
- Normal distribution
- Degrees of freedom
- Null hypothesis
- Discourse analysis
- Control groups
- Mixed methods research
- Non-probability sampling
- Quantitative research
- Ecological validity
Research bias
- Rosenthal effect
- Implicit bias
- Cognitive bias
- Selection bias
- Negativity bias
- Status quo bias
Longitudinal studies and cross-sectional studies are two different types of research design . In a cross-sectional study you collect data from a population at a specific point in time; in a longitudinal study you repeatedly collect data from the same sample over an extended period of time.
Longitudinal studies can last anywhere from weeks to decades, although they tend to be at least a year long.
Longitudinal studies are better to establish the correct sequence of events, identify changes over time, and provide insight into cause-and-effect relationships, but they also tend to be more expensive and time-consuming than other types of studies.
The 1970 British Cohort Study , which has collected data on the lives of 17,000 Brits since their births in 1970, is one well-known example of a longitudinal study .
Cite this Scribbr article
If you want to cite this source, you can copy and paste the citation or click the “Cite this Scribbr article” button to automatically add the citation to our free Citation Generator.
Thomas, L. (2023, June 22). Longitudinal Study | Definition, Approaches & Examples. Scribbr. Retrieved April 15, 2024, from https://www.scribbr.com/methodology/longitudinal-study/
Is this article helpful?

Lauren Thomas
Other students also liked, cross-sectional study | definition, uses & examples, correlational research | when & how to use, guide to experimental design | overview, steps, & examples, "i thought ai proofreading was useless but..".
I've been using Scribbr for years now and I know it's a service that won't disappoint. It does a good job spotting mistakes”
Longitudinal Study Design
Julia Simkus
Editor at Simply Psychology
BA (Hons) Psychology, Princeton University
Julia Simkus is a graduate of Princeton University with a Bachelor of Arts in Psychology. She is currently studying for a Master's Degree in Counseling for Mental Health and Wellness in September 2023. Julia's research has been published in peer reviewed journals.
Learn about our Editorial Process
Saul Mcleod, PhD
Editor-in-Chief for Simply Psychology
BSc (Hons) Psychology, MRes, PhD, University of Manchester
Saul Mcleod, PhD., is a qualified psychology teacher with over 18 years of experience in further and higher education. He has been published in peer-reviewed journals, including the Journal of Clinical Psychology.
Olivia Guy-Evans, MSc
Associate Editor for Simply Psychology
BSc (Hons) Psychology, MSc Psychology of Education
Olivia Guy-Evans is a writer and associate editor for Simply Psychology. She has previously worked in healthcare and educational sectors.
A longitudinal study is a type of observational and correlational study that involves monitoring a population over an extended period of time. It allows researchers to track changes and developments in the subjects over time.
What is a Longitudinal Study?
In longitudinal studies, researchers do not manipulate any variables or interfere with the environment. Instead, they simply conduct observations on the same group of subjects over a period of time.
These research studies can last as short as a week or as long as multiple years or even decades. Unlike cross-sectional studies that measure a moment in time, longitudinal studies last beyond a single moment, enabling researchers to discover cause-and-effect relationships between variables.
They are beneficial for recognizing any changes, developments, or patterns in the characteristics of a target population. Longitudinal studies are often used in clinical and developmental psychology to study shifts in behaviors, thoughts, emotions, and trends throughout a lifetime.
For example, a longitudinal study could be used to examine the progress and well-being of children at critical age periods from birth to adulthood.
The Harvard Study of Adult Development is one of the longest longitudinal studies to date. Researchers in this study have followed the same men group for over 80 years, observing psychosocial variables and biological processes for healthy aging and well-being in late life (see Harvard Second Generation Study).
When designing longitudinal studies, researchers must consider issues like sample selection and generalizability, attrition and selectivity bias, effects of repeated exposure to measures, selection of appropriate statistical models, and coverage of the necessary timespan to capture the phenomena of interest.
Panel Study
- A panel study is a type of longitudinal study design in which the same set of participants are measured repeatedly over time.
- Data is gathered on the same variables of interest at each time point using consistent methods. This allows studying continuity and changes within individuals over time on the key measured constructs.
- Prominent examples include national panel surveys on topics like health, aging, employment, and economics. Panel studies are a type of prospective study .
Cohort Study
- A cohort study is a type of longitudinal study that samples a group of people sharing a common experience or demographic trait within a defined period, such as year of birth.
- Researchers observe a population based on the shared experience of a specific event, such as birth, geographic location, or historical experience. These studies are typically used among medical researchers.
- Cohorts are identified and selected at a starting point (e.g. birth, starting school, entering a job field) and followed forward in time.
- As they age, data is collected on cohort subgroups to determine their differing trajectories. For example, investigating how health outcomes diverge for groups born in 1950s, 1960s, and 1970s.
- Cohort studies do not require the same individuals to be assessed over time; they just require representation from the cohort.
Retrospective Study
- In a retrospective study , researchers either collect data on events that have already occurred or use existing data that already exists in databases, medical records, or interviews to gain insights about a population.
- Appropriate when prospectively following participants from the past starting point is infeasible or unethical. For example, studying early origins of diseases emerging later in life.
- Retrospective studies efficiently provide a “snapshot summary” of the past in relation to present status. However, quality concerns with retrospective data make careful interpretation necessary when inferring causality. Memory biases and selective retention influence quality of retrospective data.
Allows researchers to look at changes over time
Because longitudinal studies observe variables over extended periods of time, researchers can use their data to study developmental shifts and understand how certain things change as we age.
High validation
Since objectives and rules for long-term studies are established before data collection, these studies are authentic and have high levels of validity.
Eliminates recall bias
Recall bias occurs when participants do not remember past events accurately or omit details from previous experiences.
Flexibility
The variables in longitudinal studies can change throughout the study. Even if the study was created to study a specific pattern or characteristic, the data collection could show new data points or relationships that are unique and worth investigating further.
Limitations
Costly and time-consuming.
Longitudinal studies can take months or years to complete, rendering them expensive and time-consuming. Because of this, researchers tend to have difficulty recruiting participants, leading to smaller sample sizes.
Large sample size needed
Longitudinal studies tend to be challenging to conduct because large samples are needed for any relationships or patterns to be meaningful. Researchers are unable to generate results if there is not enough data.
Participants tend to drop out
Not only is it a struggle to recruit participants, but subjects also tend to leave or drop out of the study due to various reasons such as illness, relocation, or a lack of motivation to complete the full study.
This tendency is known as selective attrition and can threaten the validity of an experiment. For this reason, researchers using this approach typically recruit many participants, expecting a substantial number to drop out before the end.
Report bias is possible
Longitudinal studies will sometimes rely on surveys and questionnaires, which could result in inaccurate reporting as there is no way to verify the information presented.
- Data were collected for each child at three-time points: at 11 months after adoption, at 4.5 years of age and at 10.5 years of age. The first two sets of results showed that the adoptees were behind the non-institutionalised group however by 10.5 years old there was no difference between the two groups. The Romanian orphans had caught up with the children raised in normal Canadian families.
- The role of positive psychology constructs in predicting mental health and academic achievement in children and adolescents (Marques Pais-Ribeiro, & Lopez, 2011)
- The correlation between dieting behavior and the development of bulimia nervosa (Stice et al., 1998)
- The stress of educational bottlenecks negatively impacting students’ wellbeing (Cruwys, Greenaway, & Haslam, 2015)
- The effects of job insecurity on psychological health and withdrawal (Sidney & Schaufeli, 1995)
- The relationship between loneliness, health, and mortality in adults aged 50 years and over (Luo et al., 2012)
- The influence of parental attachment and parental control on early onset of alcohol consumption in adolescence (Van der Vorst et al., 2006)
- The relationship between religion and health outcomes in medical rehabilitation patients (Fitchett et al., 1999)
Goals of Longitudinal Data and Longitudinal Research
The objectives of longitudinal data collection and research as outlined by Baltes and Nesselroade (1979):
- Identify intraindividual change : Examine changes at the individual level over time, including long-term trends or short-term fluctuations. Requires multiple measurements and individual-level analysis.
- Identify interindividual differences in intraindividual change : Evaluate whether changes vary across individuals and relate that to other variables. Requires repeated measures for multiple individuals plus relevant covariates.
- Analyze interrelationships in change : Study how two or more processes unfold and influence each other over time. Requires longitudinal data on multiple variables and appropriate statistical models.
- Analyze causes of intraindividual change: This objective refers to identifying factors or mechanisms that explain changes within individuals over time. For example, a researcher might want to understand what drives a person’s mood fluctuations over days or weeks. Or what leads to systematic gains or losses in one’s cognitive abilities across the lifespan.
- Analyze causes of interindividual differences in intraindividual change : Identify mechanisms that explain within-person changes and differences in changes across people. Requires repeated data on outcomes and covariates for multiple individuals plus dynamic statistical models.
How to Perform a Longitudinal Study
When beginning to develop your longitudinal study, you must first decide if you want to collect your own data or use data that has already been gathered.
Using already collected data will save you time, but it will be more restricted and limited than collecting it yourself. When collecting your own data, you can choose to conduct either a retrospective or prospective study .
In a retrospective study, you are collecting data on events that have already occurred. You can examine historical information, such as medical records, in order to understand the past. In a prospective study, on the other hand, you are collecting data in real-time. Prospective studies are more common for psychology research.
Once you determine the type of longitudinal study you will conduct, you then must determine how, when, where, and on whom the data will be collected.
A standardized study design is vital for efficiently measuring a population. Once a study design is created, researchers must maintain the same study procedures over time to uphold the validity of the observation.
A schedule should be maintained, complete results should be recorded with each observation, and observer variability should be minimized.
Researchers must observe each subject under the same conditions to compare them. In this type of study design, each subject is the control.
Methodological Considerations
Important methodological considerations include testing measurement invariance of constructs across time, appropriately handling missing data, and using accelerated longitudinal designs that sample different age cohorts over overlapping time periods.
Testing measurement invariance
Testing measurement invariance involves evaluating whether the same construct is being measured in a consistent, comparable way across multiple time points in longitudinal research.
This includes assessing configural, metric, and scalar invariance through confirmatory factor analytic approaches. Ensuring invariance gives more confidence when drawing inferences about change over time.
Missing data
Missing data can occur during initial sampling if certain groups are underrepresented or fail to respond.
Attrition over time is the main source – participants dropping out for various reasons. The consequences of missing data are reduced statistical power and potential bias if dropout is nonrandom.
Handling missing data appropriately in longitudinal studies is critical to reducing bias and maintaining power.
It is important to minimize attrition by tracking participants, keeping contact info up to date, engaging them, and providing incentives over time.
Techniques like maximum likelihood estimation and multiple imputation are better alternatives to older methods like listwise deletion. Assumptions about missing data mechanisms (e.g., missing at random) shape the analytic approaches taken.
Accelerated longitudinal designs
Accelerated longitudinal designs purposefully create missing data across age groups.
Accelerated longitudinal designs strategically sample different age cohorts at overlapping periods. For example, assessing 6th, 7th, and 8th graders at yearly intervals would cover 6-8th grade development over a 3-year study rather than following a single cohort over that timespan.
This increases the speed and cost-efficiency of longitudinal data collection and enables the examination of age/cohort effects. Appropriate multilevel statistical models are required to analyze the resulting complex data structure.
In addition to those considerations, optimizing the time lags between measurements, maximizing participant retention, and thoughtfully selecting analysis models that align with the research questions and hypotheses are also vital in ensuring robust longitudinal research.
So, careful methodology is key throughout the design and analysis process when working with repeated-measures data.
Cohort effects
A cohort refers to a group born in the same year or time period. Cohort effects occur when different cohorts show differing trajectories over time.
Cohort effects can bias results if not accounted for, especially in accelerated longitudinal designs which assume cohort equivalence.
Detecting cohort effects is important but can be challenging as they are confounded with age and time of measurement effects.
Cohort effects can also interfere with estimating other effects like retest effects. This happens because comparing groups to estimate retest effects relies on cohort equivalence.
Overall, researchers need to test for and control cohort effects which could otherwise lead to invalid conclusions. Careful study design and analysis is required.
Retest effects
Retest effects refer to gains in performance that occur when the same or similar test is administered on multiple occasions.
For example, familiarity with test items and procedures may allow participants to improve their scores over repeated testing above and beyond any true change.
Specific examples include:
- Memory tests – Learning which items tend to be tested can artificially boost performance over time
- Cognitive tests – Becoming familiar with the testing format and particular test demands can inflate scores
- Survey measures – Remembering previous responses can bias future responses over multiple administrations
- Interviews – Comfort with the interviewer and process can lead to increased openness or recall
To estimate retest effects, performance of retested groups is compared to groups taking the test for the first time. Any divergence suggests inflated scores due to retesting rather than true change.
If unchecked in analysis, retest gains can be confused with genuine intraindividual change or interindividual differences.
This undermines the validity of longitudinal findings. Thus, testing and controlling for retest effects are important considerations in longitudinal research.
Data Analysis
Longitudinal data involves repeated assessments of variables over time, allowing researchers to study stability and change. A variety of statistical models can be used to analyze longitudinal data, including latent growth curve models, multilevel models, latent state-trait models, and more.
Latent growth curve models allow researchers to model intraindividual change over time. For example, one could estimate parameters related to individuals’ baseline levels on some measure, linear or nonlinear trajectory of change over time, and variability around those growth parameters. These models require multiple waves of longitudinal data to estimate.
Multilevel models are useful for hierarchically structured longitudinal data, with lower-level observations (e.g., repeated measures) nested within higher-level units (e.g., individuals). They can model variability both within and between individuals over time.
Latent state-trait models decompose the covariance between longitudinal measurements into time-invariant trait factors, time-specific state residuals, and error variance. This allows separating stable between-person differences from within-person fluctuations.
There are many other techniques like latent transition analysis, event history analysis, and time series models that have specialized uses for particular research questions with longitudinal data. The choice of model depends on the hypotheses, timescale of measurements, age range covered, and other factors.
In general, these various statistical models allow investigation of important questions about developmental processes, change and stability over time, causal sequencing, and both between- and within-person sources of variability. However, researchers must carefully consider the assumptions behind the models they choose.
Longitudinal vs. Cross-Sectional Studies
Longitudinal studies and cross-sectional studies are two different observational study designs where researchers analyze a target population without manipulating or altering the natural environment in which the participants exist.
Yet, there are apparent differences between these two forms of study. One key difference is that longitudinal studies follow the same sample of people over an extended period of time, while cross-sectional studies look at the characteristics of different populations at a given moment in time.
Longitudinal studies tend to require more time and resources, but they can be used to detect cause-and-effect relationships and establish patterns among subjects.
On the other hand, cross-sectional studies tend to be cheaper and quicker but can only provide a snapshot of a point in time and thus cannot identify cause-and-effect relationships.
Both studies are valuable for psychologists to observe a given group of subjects. Still, cross-sectional studies are more beneficial for establishing associations between variables, while longitudinal studies are necessary for examining a sequence of events.
1. Are longitudinal studies qualitative or quantitative?
Longitudinal studies are typically quantitative. They collect numerical data from the same subjects to track changes and identify trends or patterns.
However, they can also include qualitative elements, such as interviews or observations, to provide a more in-depth understanding of the studied phenomena.
2. What’s the difference between a longitudinal and case-control study?
Case-control studies compare groups retrospectively and cannot be used to calculate relative risk. Longitudinal studies, though, can compare groups either retrospectively or prospectively.
In case-control studies, researchers study one group of people who have developed a particular condition and compare them to a sample without the disease.
Case-control studies look at a single subject or a single case, whereas longitudinal studies are conducted on a large group of subjects.
3. Does a longitudinal study have a control group?
Yes, a longitudinal study can have a control group . In such a design, one group (the experimental group) would receive treatment or intervention, while the other group (the control group) would not.
Both groups would then be observed over time to see if there are differences in outcomes, which could suggest an effect of the treatment or intervention.
However, not all longitudinal studies have a control group, especially observational ones and not testing a specific intervention.
Baltes, P. B., & Nesselroade, J. R. (1979). History and rationale of longitudinal research. In J. R. Nesselroade & P. B. Baltes (Eds.), (pp. 1–39). Academic Press.
Cook, N. R., & Ware, J. H. (1983). Design and analysis methods for longitudinal research. Annual review of public health , 4, 1–23.
Fitchett, G., Rybarczyk, B., Demarco, G., & Nicholas, J.J. (1999). The role of religion in medical rehabilitation outcomes: A longitudinal study. Rehabilitation Psychology, 44, 333-353.
Harvard Second Generation Study. (n.d.). Harvard Second Generation Grant and Glueck Study. Harvard Study of Adult Development. Retrieved from https://www.adultdevelopmentstudy.org.
Le Mare, L., & Audet, K. (2006). A longitudinal study of the physical growth and health of postinstitutionalized Romanian adoptees. Pediatrics & child health, 11 (2), 85-91.
Luo, Y., Hawkley, L. C., Waite, L. J., & Cacioppo, J. T. (2012). Loneliness, health, and mortality in old age: a national longitudinal study. Social science & medicine (1982), 74 (6), 907–914.
Marques, S. C., Pais-Ribeiro, J. L., & Lopez, S. J. (2011). The role of positive psychology constructs in predicting mental health and academic achievement in children and adolescents: A two-year longitudinal study. Journal of Happiness Studies: An Interdisciplinary Forum on Subjective Well-Being, 12( 6), 1049–1062.
Sidney W.A. Dekker & Wilmar B. Schaufeli (1995) The effects of job insecurity on psychological health and withdrawal: A longitudinal study, Australian Psychologist, 30: 1,57-63.
Stice, E., Mazotti, L., Krebs, M., & Martin, S. (1998). Predictors of adolescent dieting behaviors: A longitudinal study. Psychology of Addictive Behaviors, 12 (3), 195–205.
Tegan Cruwys, Katharine H Greenaway & S Alexander Haslam (2015) The Stress of Passing Through an Educational Bottleneck: A Longitudinal Study of Psychology Honours Students, Australian Psychologist, 50:5, 372-381.
Thomas, L. (2020). What is a longitudinal study? Scribbr. Retrieved from https://www.scribbr.com/methodology/longitudinal-study/
Van der Vorst, H., Engels, R. C. M. E., Meeus, W., & Deković, M. (2006). Parental attachment, parental control, and early development of alcohol use: A longitudinal study. Psychology of Addictive Behaviors, 20 (2), 107–116.
Further Information
- Schaie, K. W. (2005). What can we learn from longitudinal studies of adult development?. Research in human development, 2 (3), 133-158.
- Caruana, E. J., Roman, M., Hernández-Sánchez, J., & Solli, P. (2015). Longitudinal studies. Journal of thoracic disease, 7 (11), E537.
- Open access
- Published: 01 October 2022
Qualitative longitudinal research in health research: a method study
- Åsa Audulv 1 ,
- Elisabeth O. C. Hall 2 , 3 ,
- Åsa Kneck 4 ,
- Thomas Westergren 5 , 6 ,
- Liv Fegran 5 ,
- Mona Kyndi Pedersen 7 , 8 ,
- Hanne Aagaard 9 ,
- Kristianna Lund Dam 3 &
- Mette Spliid Ludvigsen 10 , 11
BMC Medical Research Methodology volume 22 , Article number: 255 ( 2022 ) Cite this article
10k Accesses
17 Citations
2 Altmetric
Metrics details
Qualitative longitudinal research (QLR) comprises qualitative studies, with repeated data collection, that focus on the temporality (e.g., time and change) of a phenomenon. The use of QLR is increasing in health research since many topics within health involve change (e.g., progressive illness, rehabilitation). A method study can provide an insightful understanding of the use, trends and variations within this approach. The aim of this study was to map how QLR articles within the existing health research literature are designed to capture aspects of time and/or change.
This method study used an adapted scoping review design. Articles were eligible if they were written in English, published between 2017 and 2019, and reported results from qualitative data collected at different time points/time waves with the same sample or in the same setting. Articles were identified using EBSCOhost. Two independent reviewers performed the screening, selection and charting.
A total of 299 articles were included. There was great variation among the articles in the use of methodological traditions, type of data, length of data collection, and components of longitudinal data collection. However, the majority of articles represented large studies and were based on individual interview data. Approximately half of the articles self-identified as QLR studies or as following a QLR design, although slightly less than 20% of them included QLR method literature in their method sections.
Conclusions
QLR is often used in large complex studies. Some articles were thoroughly designed to capture time/change throughout the methodology, aim and data collection, while other articles included few elements of QLR. Longitudinal data collection includes several components, such as what entities are followed across time, the tempo of data collection, and to what extent the data collection is preplanned or adapted across time. Therefore, there are several practices and possibilities researchers should consider before starting a QLR project.
Peer Review reports
Health research is focused on areas and topics where time and change are relevant. For example, processes such as recovery or changes in health status. However, relating time and change can be complicated in research, as the representation of reality in research publications is often collected at one point in time and fixed in its presentation, although time and change are always present in human life and experiences. Qualitative longitudinal research (QLR; also called longitudinal qualitative research, LQR) has been developed to focus on subjective experiences of time or change using qualitative data materials (e.g., interviews, observations and/or text documents) collected across a time span with the same participants and/or in the same setting [ 1 , 2 ]. QLR within health research may have many benefits. Firstly, human experiences are not fixed and consistent, but changing and diverse, therefore people’s experiences in relation to a health phenomenon may be more comprehensively described by repeated interviews or observations over time. Secondly, experiences, behaviors, and social norms unfold over time. By using QLR, researchers can collect empirical data that represents not only recalled human conceptions but also serial and instant situations reflecting transitions, trajectories and changes in people’s health experiences, personal development or health care organizations [ 3 , 4 , 5 ].
Key features of QLR
Whether QLR is a methodological approach in its own right or a design element of a particular study within a traditional methodological approach (e.g., ethnography or grounded theory) is debated [ 1 , 6 ]. For example, Bennett et al. [ 7 ] describe QLR as untied to methodology, giving researchers the flexibility to develop a suitable design for each study. McCoy [ 6 ] suggests that epistemological and ontological standpoints from interpretative phenomenological analysis (IPA) align with QLR traditions, thus making longitudinal IPA a suitable methodology. Plano-Clark et al. [ 8 ] described how longitudinal qualitative elements can be used in mixed methods studies, thus creating longitudinal mixed methods. In contrast, several researchers have argued that QLR is an emerging methodology [ 1 , 5 , 9 , 10 ]. For example, Thomson et al. [ 9 ] have stated “What distinguishes longitudinal qualitative research is the deliberate way in which temporality is designed into the research process, making change a central focus of analytic attention” (p. 185). Tuthill et al. [ 5 ] concluded that some of the confusion might have arisen from the diversity of data collection methods and data materials used within QLR research. However, there are no investigations showing to what extent QLR studies use QLR as a distinct methodology versus using a longitudinal data collection as a more flexible design element in combination with other qualitative methodologies.
QLR research should focus on aspects of temporality, time and/or change [ 11 , 12 , 13 ]. The concepts of time and change are seen as inseparable since change is happening with the passing of time [ 13 ]. However, time can be conceptualized in different ways. Time is often understood from a chronological perspective, and is viewed as fixed, objective, continuous and measurable (e.g., clock time, duration of time). However, time can also be understood from within, as the experience of the passing of time and/or the perspective from the current moment into the constructed conception of a history or future. From this perspective, time is seen as fluid, meaning that events, contexts and understandings create a subjective experience of time and change. Both the chronological and fluid understanding of time influence QLR research [ 11 ]. Furthermore, there is a distinction between over-time, which constitutes a comparison of the difference between points in time, often with a focus on the latter point or destination, and through-time, which means following an aspect across time while trying to understand the change that occurs [ 11 ]. In this article, we will mostly use the concept of across time to include both perspectives.
Some authors assert that QLR studies should include a qualitative data collection with the same sample across time [ 11 , 13 ], whereas Thomson et al. [ 9 ] also suggest the possibility of returning to the same data collection site with the same or different participants. When a QLR study involves data collection in shorter engagements, such as serial interviews, these engagements are often referred to as data collection time points. Data collection in time waves relates to longer engagements, such as field work/observation periods. There is no clear-cut definition for the minimum time span of a QLR study; instead, the length of the data collection period must be decided based upon what processes or changes are the focus of the study [ 13 ].
Most literature describing QLR methods originates from the social sciences, where the approach has a long tradition [ 1 , 10 , 14 ]. In health research, one-time-data collection studies have been the norm within qualitative methods [ 15 ], although health research using QLR methods has increased in recent years [ 2 , 5 , 16 , 17 ]. However, collecting and managing longitudinal data has its own sets of challenges, especially regarding how to integrate perspectives of time and/or change in the data collection and subsequent analysis [ 1 ]. Therefore, a study of QLR articles from the health research literature can provide an insightful understanding of the use, trends and variations of how methods are used and how elements of time/change are integrated in QLR studies. This could, in turn, provide inspiration for using different possibilities of collecting data across time when using QLR in health research. The aim of this study was to map how QLR articles within the existing health research literature are designed to capture aspects of time and/or change.
More specifically, the research questions were:
What methodological approaches are described to inform QLR research?
What methodological references are used to inform QLR research?
How are longitudinal perspectives articulated in article aims?
How is longitudinal data collection conducted?
In this method study, we used an adapted scoping review method [ 18 , 19 , 20 ]. Method studies are research conducted on research studies to investigate how research design elements are applied across a field [ 21 ]. However, since there are no clear guidelines for method studies, they often use adapted versions of systematic reviews or scoping review methods [ 21 ]. The adaptations of the scoping review method consisted of 1) using a large subsample of studies (publications from a three-year period) instead of including all QLR articles published, and 2) not including grey literature. The reporting of this study was guided by the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist [ 20 , 22 ] (see Additional file 1 ). A (unpublished) protocol was developed by the research team during the spring of 2019.
Eligibility criteria
In line with method study recommendations [ 21 ], we decided to draw on a manageable subsample of published QLR research. Articles that were eligible for inclusion were health research primary studies written in English, published between 2017 and 2019, and with a longitudinal qualitative data collection. Our operating definition for qualitative longitudinal data collection was data collected at different time points (e.g., repeated interviews) or time waves (e.g., periods of field work) involving the same sample or conducted in the same setting(s). We intentionally selected a broad inclusion criterion for QLR since we wanted a wide variety of articles. The selected time period was chosen because the first QLR method article directed towards health research was published in 2013 [ 1 ] and during the following years the methodological resources for QLR increased [ 3 , 8 , 17 , 23 , 24 , 25 ], thus we could expect that researchers publishing QLR in 2017–2019 should be well-grounded in QLR methods. Further, we found that from 2012 to 2019 the rate of published QLR articles were steady at around 100 publications per year, so including those from a three-year period would give a sufficient number of articles (~ 300 articles) for providing an overview of the field. Published conference abstracts, protocols, articles describing methodological issues, review articles, and non-research articles (e.g., editorials) were excluded.
Search strategy
Relevant articles were identified through systematic searches in EBSCOhost, including biomedical and life science research and nursing and allied health literature. A librarian who specialized in systematic review searches developed and performed the searches, in collaboration with the author team (LF, TW & ÅA). In the search, the term “longitudinal” was combined with terms for qualitative research (for the search strategy see Additional file 2 ). The searches were conducted in the autumn of 2019 (last search 2019-09-10).
Study selection
All identified citations were imported into EndNote X9 ( www.endnote.com ) and further imported into Rayyan QCRI online software [ 26 ], and duplicates were removed. All titles and abstracts were screened against the eligibility criteria by two independent reviewers (ÅA & EH), and conflicting decisions were discussed until resolved. After discussions by the team, we decided to include articles published between 2017 and 2019, that selection alone included 350 records with diverse methods and designs. The full texts of articles that were eligible for inclusion were retrieved. In the next stage, two independent reviewers reviewed each full text article to make final decisions regarding inclusion (ÅA, EH, Julia Andersson). In total, disagreements occurred in 8% of the decisions, and were resolved through discussion. Critical appraisal was not assessed since the study aimed to describe the range of how QLR is applied and not aggregate research findings [ 21 , 22 ].
Data charting and analysis
A standardized charting form was developed in Excel (Excel 2016). The charting form was reviewed by the research team and pretested in two stages. The tests were performed to increase internal consistency and reduce the risk of bias. First, four articles were reviewed by all the reviewers, and modifications were made to the form and charting instructions. In the next stage, all reviewers used the charting form on four other articles, and the convergence in ratings was 88%. Since the convergence was under 90%, charting was performed in duplicate to reduce errors in the data. At the end of the charting process, the convergence among the reviewers was 95%. The charting was examined by the first author, who revised the charting in cases of differences.
Data items that were charted included 1) the article characteristics (e.g., authors, publication year, journal, country), 2) the aim and scope (e.g., phenomenon of interest, population, contexts), 3) the stated methodology and analysis method, 4) text describing the data collection (e.g., type of data material, number of participants, time frame of data collection, total amount of data material), and 5) the qualitative methodological references used in the methods section. Extracted text describing data collection could consist of a few sentences or several sections from the articles (and sometimes figures) concerning data collection practices, rational for time periods and research engagement in the field. This was later used to analyze how the longitudinal data collection was conducted and elements of longitudinal design. To categorize the qualitative methodology approaches, a framework from Cresswell [ 27 ] was used (including the categories for grounded theory, phenomenology, ethnography, case study and narrative research). Overall, data items needed to be explicitly stated in the articles in order to be charted. For example, an article was categorized as grounded theory if it explicitly stated “in this grounded theory study” but not if it referred to the literature by Glaser and Strauss without situating itself as a grounded theory study (See Additional file 3 for the full instructions for charting).
All charting forms were compiled into a single Microsoft Excel spreadsheet (see Supplementary files for an overview of the articles). Descriptive statistics with frequencies and percentages were calculated to summarize the data. Furthermore, an iterative coding process was used to group the articles and investigate patterns of, for example, research topics, words in the aims, or data collection practices. Alternative ways of grouping and presenting the data were discussed by the research team.
Search and selection
A total of 2179 titles and abstracts were screened against the eligibility criteria (see Fig. 1 ). The full text of one article could not be found and the article was excluded [ 28 ]. Fifty full text articles were excluded. Finally, 299 articles, representing 271 individual studies, were included in this study (see additional files 4 and 5 respectively for tables of excluded and included articles).

PRISMA diagram of study selection]
General characteristics and research areas of the included articles
The articles were published in many journals ( n = 193), and 138 of these journals were represented with one article each. BMJ Open was the most prevalent journal ( n = 11), followed by the Journal of Clinical Nursing ( n = 8). Similarly, the articles represented many countries ( n = 41) and all the continents; however, a large part of the studies originated from the US or UK ( n = 71, 23.7% and n = 70, 23.4%, respectively). The articles focused on the following types of populations: patients, families−/caregivers, health care providers, students, community members, or policy makers. Approximately 20% ( n = 63, 21.1%) of the articles collected data from two or more of these types of population(s) (see Table 1 ).
Approximately half of the articles ( n = 158, 52.8%) articulated being part of a larger research project. Of them, 95 described a project with both quantitative and qualitative methods. They represented either 1) a qualitative study embedded in an intervention, evaluation or implementation study ( n = 66, 22.1%), 2) a longitudinal cohort study collecting both quantitative and qualitative material ( n = 23, 7.7%), or 3) qualitative longitudinal material collected together with a cross sectional survey (n = 6, 2.0%). Forty-eight articles (16.1%) described belonging to a larger qualitative project presented in several research articles.
Methodological traditions
Approximately one-third ( n = 109, 36.5%) of the included articles self-identified with one of the qualitative traditions recognized by Cresswell [ 27 ] (case study: n = 36, 12.0%; phenomenology: n = 35, 11.7%; grounded theory: n = 22, 7.4%; ethnography: n = 13, 4.3%; narrative method: n = 3, 1.0%). In nine articles, the authors described using a mix of two or more of these qualitative traditions. In addition, 19 articles (6.4%) self-identified as mixed methods research.
Every second article self-identified as having a qualitative longitudinal design ( n = 156, 52.2%); either they self-identified as “a longitudinal qualitative study” or “using a longitudinal qualitative research design”. However, in some articles, this was stated in the title and/or abstract and nowhere else in the article. Fifty-two articles (17.4%) self-identified both as having a QLR design and following one of the methodological approaches (case study: n = 8; phenomenology: n = 23; grounded theory: n = 9; ethnography: n = 6; narrative method: n = 2; mixed methods: n = 4).
The other 143 articles used various terms to situate themselves in relation to a longitudinal design. Twenty-seven articles described themselves as a longitudinal study (9.0%) or a longitudinal study within a specific qualitative tradition (e.g., a longitudinal grounded theory study or a longitudinal mixed method study) ( n = 64, 21.4%). Furthermore, 36 articles (12.0%) referred to using longitudinal data materials (e.g., longitudinal data or longitudinal interviews). Nine of the articles (3.0%) used the term longitudinal in relation to the data analysis or aim (e.g., the aim was to longitudinally describe), used terms such as serial or repeated in relation to the data collection design ( n = 2, 0.7%), or did not use any term to address the longitudinal nature of their design ( n = 5, 1.7%).
Use of methodological references
The mean number of qualitative method references in the methods sections was 3.7 (range 0 to 16), and 20 articles did not have any qualitative method reference in their methods sections. Footnote 1 Commonly used method references were generic books on qualitative methods, seminal works within qualitative traditions, and references specializing in qualitative analysis methods (see Table 2 ). It should be noted that some references were comprehensive books and thus could include sections about QLR without being focused on the QLR method. For example, Miles et al. [ 31 ] is all about analysis and coding and includes a chapter regarding analyzing change.
Only approximately 20% ( n = 58) of the articles referred to the QLR method literature in their methods sections. Footnote 2 The mean number of QLR method references (counted for articles using such sources) was 1.7 (range 1 to 6). Most articles using the QLR method literature also used other qualitative methods literature (except two articles using one QLR literature reference each [ 39 , 40 ]). In total, 37 QLR method references were used, and 24 of the QLR method references were only referred to by one article each.
Longitudinal perspectives in article aims
In total, 231 (77.3%) articles had one or several terms related to time or change in their aims, whereas 68 articles (22.7%) had none. Over one hundred different words related to time or change were identified. Longitudinally oriented terms could focus on changes across time (process, trajectory, transition, pathway or journey), patterns of how something changed (maintenance, continuity, stability, shifts), or phenomena that by nature included change (learning or implementation). Other types of terms emphasized the data collection time period (e.g., over 6 months) or a specific changing situation (e.g., during pregnancy, through the intervention period, or moving into a nursing home). The most common terms used for the longitudinal perspective were change ( n = 63), over time ( n = 52), process ( n = 36), transition ( n = 24), implementation ( n = 14), development ( n = 13), and longitudinal (n = 13). Footnote 3
Furthermore, the articles varied in what ways their aims focused on time/change, e.g., the longitudinal perspectives in the aims (see Table 3 ). In 71 articles, the change across time was the phenomenon of interest of the article : for example, articles investigating the process of learning or trajectories of diseases. In contrast, 46 articles investigated change or factors impacting change in relation to a defined outcome : for example, articles investigating factors influencing participants continuing in a physical activity trial. The longitudinal perspective could also be embedded in an article’s context . In such cases, the focus of the article was on experiences that happened during a certain time frame or in a time-related context (e.g., described experiences of the patient-provider relationship during 6 months of rehabilitation).
Types of data and length of data collection
The QLR articles were often large and complex in their data collection methods. The median number of participants was 20 (range from one to 1366, the latter being an article with open-ended questions in questionnaires [ 46 ]). Most articles used individual interviews as the data material ( n = 167, 55.9%) or a combination of data materials ( n = 98, 32.8%) (e.g., interviews and observations, individual interviews and focus group interviews, or interviews and questionnaires). Forty-five articles (15.1%) presented quantitative and qualitative results. The median number of interviews was 46 (range three to 507), which is large in comparison to many qualitative studies. The observation materials were also comprehensive and could include several hundred hours of observations. Documents were often used as complementary material and included official documents, newspaper articles, diaries, and/or patient records.
The articles’ time spans Footnote 4 for data collection varied between a few days and over 20 years, with 60% of the articles’ time spans being 1 year or shorter ( n = 180) (see Fig. 2 ). The variation in time spans might be explained by the different kinds of phenomena that were investigated. For example, Jensen et al. [ 47 ] investigated hospital care delivery and followed each participant, with observations lasting between four and 14 days. Smithbattle [ 48 ] described the housing trajectories of teen mothers, and collected data in seven waves over 28 years.

Number of articles in relation to the time span of data collection. The time span of data collection is given in months
Three components of longitudinal data collection
In the articles, the data collection was conducted in relation to three different longitudinal data collection components (see Table 4 ).
Entities followed across time
Four different types of entities were followed across time: 1) individuals, 2) individual cases or dyads, 3) groups, and 4) settings. Every second article ( n = 170, 56.9%) followed individuals across time, thus following the same participants through the whole data collection period. In contrast, when individual cases were followed across time, the data collection was centered on the primary participants (e.g., people with progressive neurological conditions) who were followed over time, and secondary participants (e.g., family caregivers) might provide complementary data at several time points or only at one-time point. When settings were followed over time, the participating individuals were sometimes the same, and sometimes changed across the data collection period. Typical settings were hospital wards, hospitals, smaller communities or intervention trials. The type of collected data corresponded with what kind of entities were followed longitudinally. Individuals were often followed with serial interviews, whereas groups were commonly followed with focus group interviews complemented with individual interviews, observations and/or questionnaires. Overall, the lengths of data collection periods seemed to be chosen based upon expected changes in the chosen entities. For example, the articles following an intervention setting were structured around the intervention timeline, collecting data before, after and sometimes during the intervention.
Tempo of data collection
The data collection tempo differed among the articles (e.g., the frequency and mode of the data collection). Approximately half ( n = 154, 51.5%) of the articles used serial time points, collecting data at several reoccurring but shorter sequences (e.g., through serial interviews or open-ended questions in questionnaires). When data were collected in time waves ( n = 50, 16.7%), the periods of data collection were longer, usually including both interviews and observations; often, time waves included observations of a setting and/or interviews at the same location over several days or weeks.
When comparing the tempo with the type of entities, some patterns were detected (see Fig. 3 ). When individuals were followed, data were often collected at time points, mirroring the use of individual interviews and/or short observations. For research in settings, data were commonly collected in time waves (e.g., observation periods over a few weeks or months). In studies exploring settings across time, time waves were commonly used and combined several types of data, particularly from interviews and observations. Groups were the least common studied entity ( n = 9, 3.0%), so the numbers should be interpreted with caution, but continuous data collection was used in five of the nine studies. The continuous data collection mode was, for example, collecting electronic diaries [ 62 ] or minutes from committee meetings during a time period [ 63 ].

Tempo of data collection in relation to entities followed over time
Preplanned or adapted data collection
A large majority ( n = 224, 74.9%) of the articles used preplanned data collection (e.g., in preplanned data collection, all participants were followed across time according to the same data collection plan). For example, all participants were interviewed one, six and twelve months’ post-diagnosis. In contrast to the preplanned data collection approach, 44 articles had a participant-adapted data collection (14.7%), and participants were followed at different frequencies and/or over various lengths of time depending on each participant’s situation. Participant-adapted data collection was more common among articles following individuals or individual cases (see Fig. 4 ). To adapt the data collection to the participants, the researchers created strategies to reach participants when crucial events were happening. Eleven articles used a participant entry approach to data collection ( n = 11, 6.7%), and the whole or parts of the data were independently sent in by participants in the form of diaries, questionnaires, or blogs. Another approach to data collection was using theoretical or analysis-driven ideas to guide the data collection ( n = 19, 6.4%). In these articles, the analysis and data collection were conducted simultaneously, and ideas arising in the analysis could be followed up, for example, returning to some participants, recruiting participants with specific experiences, or collecting complementary types of data materials. This approach was most common in the articles following settings across time, which often included observations and interviews with different types of populations. Articles using theoretical or analysis driven data collection were not associated with grounded theory to a greater extent than the other articles in the sample (e.g., did not self-identify as grounded theory or referred to methodological literature within grounded theory traditions to a greater proportion).

Preplanned or adapted data collection in relation to entities followed over time
According to our results, some researchers used QLR as a methodological approach and other researchers used a longitudinal qualitative data collection without aiming to investigate change. Adding to the debate on whether QLR is a methodological approach in its own right or a design element in a particular study we suggest that the use of QLR can be described as layered (see Fig. 5 ). Namely, articles must fulfill several criteria in order to use QLR as a methodological approach, and that is done in some articles. In those articles QLR method references were used, the aim was to investigate change of a phenomenon and the longitudinal elements of the data collection were thoroughly integrated into the method section. On the other hand, some articles using a longitudinal qualitative data collection were just collecting data over time, without addressing time and/or change in the aim. These articles can still be interesting research studies with valuable results, but they are not using the full potential of QLR as a methodological approach. In all, around 40% of the articles had an aim that focused on describing or understanding change (either as phenomenon or outcome); but only about 24% of the articles set out to investigate change across time as their phenomenon of interest.

The QLR onion. The use of QLR design can be described as layered, where researchers use more or less elements of a QLR design. The two inmost layers represents articles using QLR as a methodological approach
Regarding methodological influences, about one-third of the articles self-identify with any of the traditional qualitative methodologies. Using a longitudinal qualitative data collection as an element integrated with another methodological tradition can therefore be seen as one way of working with longitudinal qualitative materials. In our results, the articles referring to methodologies other than QLR preferably used case study, phenomenology and grounded theory methodologies. This was surprising since Neale [ 10 ] identified ethnography, case studies and narrative methods as the main methodological influences on QLR. Our findings might mirror the profound impacts that phenomenology and grounded theory have had on the qualitative field of health research. Regarding phenomenology, the findings can also be influenced by more recent discussions of combining interpretative phenomenological analysis with QLR [ 6 ].
Half of the articles self-identified as QLR studies, but QLR method references were used in less than 20% of the identified articles. This is both surprising and troublesome since use of appropriate method literature might have supported researchers who were struggling with for example a large quantity of materials and complex analysis. A possible explanation for the lack of use of QLR method literature is that QLR as a methodological approach is not well known, and authors might not be aware that method literature exists. It is quite understandable that researchers can describe a qualitative project with longitudinal data collection as a qualitative longitudinal study, without being aware that QLR is a specific form of study. Balmer [ 64 ] described how their group conducted serial interviews with medical students over several years before they became aware of QLR as a method of study. Within our networks, we have met researchers with similar experiences. Likewise, peer reviewers and editorial boards might not be accustomed to evaluating QLR manuscripts. In our results, 138 journals published one article between 2017 and 2019, and that might not be enough for editorial boards and peer reviewers to develop knowledge to enable them to closely evaluate manuscripts with a QLR method.
In 2007, Holland and colleagues [ 65 ] mapped QLR in the UK and described the following four categories of QLR: 1) mixed methods approaches with a QLR component; 2) planned prospective longitudinal studies; 3) follow-up studies complementing a previous data collection with follow-up; and 4) evaluation studies. Examples of all these categories can be found among the articles in this method study; however, our results do paint a more complex picture. According to our results, Holland’s categories are not multi-exclusive. For example, studies with intentions to evaluate or implement practices often used a mixed methods design and were therefore eligible for both categories one and four described above. Additionally, regarding the follow-up studies, it was seldom clearly described if they were planned as a two-time-point study or if researchers had gained an opportunity to follow up on previous data collection. When we tried to categorize QLR articles according to the data collection design, we could not identify multi-exclusive categories. Instead, we identified the following three components of longitudinal data collection: 1) entities followed across time; 2) tempo; and 3) preplanned or adapted data collection approaches. However, the most common combination was preplanned studies that followed individuals longitudinally with three or more time points.
The use of QLR differs between disciplines [ 14 ]. Our results show some patterns for QLR within health research. Firstly, the QLR projects were large and complex; they often included several types of populations and various data materials, and were presented in several articles. Secondly, most studies focused upon the individual perspective, following individuals across time, and using individual interviews. Thirdly, the data collection periods varied, but 53% of the articles had a data collection period of 1 year or shorter. Finally, patients were the most prevalent population, even though topics varied greatly. Previously, two other reviews that focused on QLR in different parts of health research (e.g., nursing [ 4 ] and gerontology [ 66 ]) pointed in the same direction. For example, individual interviews or a combination of data materials were commonly used, and most studies were shorter than 1 year but a wide range existed [ 4 , 66 ].
Considerations when planning a QLR project
Based on our results, we argue that when health researchers plan a QLR study, they should reflect upon their perspective of time/change and decide what part change should play in their QLR study. If researchers decide that change should play the main role in their project, then they should aim to focus on change as the phenomenon of interest. However, in some research, change might be an important part of the plot, without having the main role, and change in relation to the outcomes might be a better perspective. In such studies, participants with change, no change or different kinds of change are compared to explore possible explanations for the change. In our results, change in relation to the outcomes was often used in relation to intervention studies where participants who reached a desired outcome were compared to individuals who did not. Furthermore, for some research studies, change is part of the context in which the research takes place. This can be the case when certain experiences happen during a period of change; for example, when the aim is to explore the experience of everyday life during rehabilitation after stroke. In such cases a longitudinal data collection could be advisable (e.g., repeated interviews often give a deep relationship between interviewer and participants as well as the possibility of gaining greater depth in interview answers during follow-up interviews [ 15 ]), but the study might not be called a QLR study since it does not focus upon change [ 13 ]. We suggest that researchers make informed decisions of what kind of longitudinal perspective they set out to investigate and are transparent with their sources of methodological inspiration.
We would argue that length of data collection period, type of entities, and data materials should be in accordance with the type of change/changing processes that a study focuses on. Individual change is important in health research, but researchers should also remember the possibility of investigating changes in families, working groups, organizations and wider communities. Using these types of entities were less common in our material and could probably grant new perspectives to many research topics within health. Similarly, using several types of data materials can complement the insights that individual interviews can give. A large majority of the articles in our results had a preplanned data collection. Participant-adapted data collection can be a way to work in alignment with a “time-as-fluid” conceptualization of time because the events of subjective importance to participants can be more in focus and participants (or other entities) change processes can differ substantially across cases. In studies with lengthy and spaced-out data collection periods and/or uncertainty in trajectories, researchers should consider participant-adapted or participant entry data collection. For example, some participants can be followed for longer periods and/or with more frequency.
Finally, researchers should consider how to best publish and disseminate their results. Many QLR projects are large, and the results are divided across several articles when they are published. In our results, 21 papers self-identified as a mixed methods project or as part of a larger mixed methods project, but most of these did not include quantitative data in the article. This raises the question of how to best divide a large research project into suitable pieces for publication. It is an evident risk that the more interesting aspects of a mixed methods project are lost when the qualitative and quantitative parts are analyzed and published separately. Similar risks occur, for example, when data have been collected from several types of populations but are then presented per population type (e.g., one article with patient data and another with caregiver data). During the work with our study, we also came across studies where data were collected longitudinally, but the results were divided into publications per time point. We do not argue that these examples are always wrong, there are situations when these practices are appropriate. However, it often appears that data have been divided without much consideration. Instead, we suggest a thematic approach to dividing projects into publications, crafting the individual publications around certain ideas or themes and thus using the data that is most suitable for the particular research question. Combining several types of data and/or several populations in an analysis across time is in fact what makes QLR an interesting approach.
Strengths and limitations
This method study intended to paint a broad picture regarding how longitudinal qualitative methods are used within the health research field by investigating 299 published articles. Method research is an emerging field, currently with limited methodological guidelines [ 21 ], therefore we used scoping review method to support this study. In accordance with scoping review method we did not use quality assessment as a criterion for inclusion [ 18 , 19 , 20 ]. This can be seen as a limitation because we made conclusions based upon a set of articles with varying quality. However, we believe that learning can be achieved by looking at both good and bad examples, and innovation may appear when looking beyond established knowledge, or assessing methods from different angles. It should also be noted that the results given in percentages hold no value for what procedures that are better or more in accordance with QLR, the percentages simply state how common a particular procedure was among the articles.
As described, the included articles showed much variation in the method descriptions. As the basis for our results, we have only charted explicitly written text from the articles, which might have led to an underestimation of some results. The researchers might have had a clearer rationale than described in the reports. Issues, such as word restrictions or the journal’s scope, could also have influenced the amount of detail that was provided. Similarly, when charting how articles drew on a traditional methodology, only data from the articles that clearly stated the methodologies they used (e.g., phenomenology) were charted. In some articles, literature choices or particular research strategies could implicitly indicate that the researchers had been inspired by certain methodologies (e.g., referring to grounded theory literature and describing the use of simultaneous data collection and analysis could indicate that the researchers were influenced by grounded theory), but these were not charted as using a particular methodological tradition. We used the articles’ aims and objectives/research questions to investigate their longitudinal perspectives. However, as researchers have different writing styles, information regarding the longitudinal perspectives could have been described in surrounding text rather than in the aim, which might have led to an underestimation of the longitudinal perspectives.
The experience and diversity of the research team in our study was a strength. The nine authors on the team represent ten universities and three countries, and have extensive experience in different types of qualitative research, QLR and review methods. The different level of experiences with QLR within the team (some authors have worked with QLR in several projects and others have qualitative experience but no experience in QLR) resulted in interesting discussions that helped drive the project forward. These experiences have been useful for understanding the field.
Based on a method study of 299 articles, we can conclude that QLR in health research articles published between 2017 and 2019 often contain comprehensive complex studies with a large variation in topics. Some research was thoroughly designed to capture time/change throughout the methodology, focus and data collection, while other articles included a few elements of QLR. Longitudinal data collection included several components, such as what entities were followed across time, the tempo of data collection, and to what extent the data collection was preplanned or adapted across time. In sum, health researchers need to be considerate and make informed choices when designing QLR projects. Further research should delve deeper into what kind of research questions go well with QLR and investigate the best practice examples of presenting QLR findings.
Availability of data and materials
The datasets used and analyzed in this current study are available in supplementary file 6 .
Qualitative method references were defined as a journal article or book with a title that indicated an aim to guide researchers in qualitative research methods and/or research theories. Primary studies, theoretical works related to the articles’ research topics, protocols, and quantitative method literature were excluded. References written in a language other than English was also excluded since the authors could not evaluate their content.
QLR method references were defined as a journal article or book that 1) focused on qualitative methodological questions, 2) used terms such as ‘longitudinal’ or ‘time’ in the title so it was evident that the focus was on longitudinal qualitative research. Referring to another original QLR study was not counted as using QLR method literature.
Words were charted depending on their word stem, e.g., change, changes and changing were all charted as change.
It should be noted that here time span refers to the data collection related to each participant or case. Researchers could collect data for 2 years but follow each participant for 6 months.
Calman L, Brunton L, Molassiotis A. Developing longitudinal qualitative designs: lessons learned and recommendations for health services research. BMC Med Res Methodol. 2013;13:14.
Article PubMed PubMed Central Google Scholar
Solomon P, Nixon S, Bond V, Cameron C, Gervais N. Two approaches to longitudinal qualitative analyses in rehabilitation and disability research. Disabil Rehabil. 2020;42:3566–72.
Article PubMed Google Scholar
Grossoehme D, Lipstein E. Analyzing longitudinal qualitative data: the application of trajectory and recurrent cross-sectional approaches. BMC Res Notes. 2016;9:136.
SmithBattle L, Lorenz R, Reangsing C, Palmer JL, Pitroff G. A methodological review of qualitative longitudinal research in nursing. Nurs Inq. 2018;25:e12248.
Tuthill EL, Maltby AE, DiClemente K, Pellowski JA. Longitudinal qualitative methods in health behavior and nursing research: assumptions, design, analysis and lessons learned. Int J Qual Methods. 2020;19:10.
Article PubMed Central Google Scholar
McCoy LK. Longitudinal qualitative research and interpretative phenomenological analysis: philosophical connections and practical considerations. Qual Res Psychol. 2017;14:442–58.
Article Google Scholar
Bennett D, Kajamaa A, Johnston J. How to... Do longitudinal qualitative research. Clin Teach. 2020;17:489–92.
Plano Clark V, Anderson N, Wertz JA, Zhou Y, Schumacher K, Miaskowski C. Conceptualizing longitudinal mixed methods designs: a methodological review of health sciences research. J Mix Methods Res. 2014;23:1–23.
Google Scholar
Thomson R, Plumridge L, Holland J. Longitudinal qualitative research: a developing methodology. Int J Soc Res Methodol. 2003;6:185–7.
Neale B. The craft of qualitative longitudinal research: thousand oaks. Sage. 2021.
Balmer DF, Varpio L, Bennett D, Teunissen PW. Longitudinal qualitative research in medical education: time to conceptualise time. Med Educ. 2021;55:1253–60.
Smith N. Cross-sectional profiling and longitudinal analysis: research notes on analysis in the longitudinal qualitative study, 'Negotiating transitions to Citizenship'. Int J Soc Res Methodol. 2003;6:273–7.
Saldaña J. Longitudinal qualitative research - analyzing change through time. Walnut Creek: AltaMira Press; 2003.
Corden A, Millar J. Time and change: a review of the qualitative longitudinal research literature for social policy. Soc Policy Soc. 2007;6:583–92.
Thorne S. Interpretive description: qualitative research for applied practice (2nd ed): Routledge; 2016.
Book Google Scholar
Kneck Å, Audulv Å. Analyzing variations in changes over time: development of the pattern-oriented longitudinal analysis approach. Nurs Inq. 2019;26:e12288.
Whiffin CJ, Bailey C, Ellis-Hill C, Jarrett N. Challenges and solutions during analysis in a longitudinal narrative case study. Nurse Res. 2014;21:20–62.
Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8:19–32.
Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5:69.
Peters MDJ, Marnie C, Tricco AC, Pollock D, Munn Z, Alexander L, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Implementation. 2021;19:3–10.
Mbuagbaw L, Lawson DO, Puljak L, Allison DB, Thabane L. A tutorial on methodological studies: the what, when, how and why. BMC Med Res Methodol. 2020;20:226.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern. 2018;169:467–73.
Neale B. Adding time into the mix: stakeholder ethics in qualitative longitudinal research. Methodological Innovations Online. 2013;8:6–20.
Henderson S, Holland J, McGrellis S, Sharpe S, Thomson R. Storying qualitative longitudinal research: sequence, voice and motif. Qual Res. 2016;12:16–34.
Balmer DF, Richards BF. Longitudinal qualitative research in medical education. Perspect Med Educ. 2017;6:306–10.
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5:210.
Creswell JW. Qualitative inquiry and research design: choosing among five approaches. 3rd ed: SAGE Publications; 2012.
McIntyre H, Fraser D. 'Hands-off' breastfeeding skill development in a UK, UNICEF baby friendly initiative pre-registration midwifery programme. MIDIRS Midwifery Digest. 2018;28:98–102.
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77–101.
Patton MQ. Qualitative research and evaluation methods: integrating theory and practice. Sage. 2015.
Miles M, Huberman A, Saldaña J. Qualitative data analysis: a methods sourcebook. 4th ed: Sage Publications; 2020.
Miles MB, Huberman AM. Qualitative data analysis: an expanded sourcebook (2nd ed): Sage Publications; 1994.
Smith JA, Flowers P, Larkin M. Interpretative phenomenological analysis: theory, method and research. Sage. 2009.
Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15:1277–88.
Glaser B, Strauss A. The discovery of grounded theory: strategies for qualitative research. Aldine De Gruyter. 1967.
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19:349–57.
Murray SA, Kendall M, Carduff E, Worth A, Harris FM, Lloyd A, et al. Use of serial qualitative interviews to understand patients' evolving experiences and needs. BMJ. 2009;339:b3702.
Thomson R, Holland J. Hindsight, foresight and insight: the challenges of longitudinal qualitative research. Int J Soc Res Methodol. 2003;6:233–44.
Morrow V, Tafere Y, Chuta N, Zharkevich I. "I started working because I was hungry": the consequences of food insecurity for children's well-being in rural Ethiopia. Soc Sci Med. 2017;182:1–9.
Solomon P, O'Brien KK, Nixon S, Letts L, Baxter L, Gervais N. Qualitative longitudinal study of episodic disability experiences of older women living with HIV in Ontario, Canada. BMJ Open. 2018;8:e021507.
Coombs MA, Parker R, de Vries K. Managing risk during care transitions when approaching end of life: a qualitative study of patients’ and health care professionals’ decision making. Palliat Med. 2017;31:617–24.
Vaghefi I, Tulu B. The continued use of mobile health apps: insights from a longitudinal study. JMIR Mhealth And Uhealth. 2019;7:e12983.
Andersen IC, Thomsen TG, Bruun P, Bødtger U, Hounsgaard L. Patients' and their family members' experiences of participation in care following an acute exacerbation in chronic obstructive pulmonary disease: a phenomenological-hermeneutic study. J Clin Nurs. 2017;26:4877–89.
Albrecht TA, Keim-Malpass J, Boyiadzis M, Rosenzweig M. Psychosocial experiences of young adults diagnosed with acute leukemia during hospitalization for induction chemotherapy treatment. JHPN. 2019;21:167–73.
PubMed Google Scholar
Corepal R, Best P, O'Neill R, Tully MA, Edwards M, Jago R, et al. Exploring the use of a gamified intervention for encouraging physical activity in adolescents: a qualitative longitudinal study in Northern Ireland. BMJ Open. 2018;8:e019663.
PubMed PubMed Central Google Scholar
Malin H, Liauw I, Damon W. Purpose and character development in early adolescence. J Youth Adolesc. 2017;46:1200–15.
Jensen AM, Pedersen BD, Olsen RB, Hounsgaard L. Medication and care in Alzheimer's patients in the acute care setting: a qualitative analysis. Dementia. 2019;18:2173–88.
SmithBattle L. Housing trajectories of teen mothers and their families over 28 years. Am J Orthop. 2019;89:258–67.
Denney-Koelsch EM, Côté-Arsenault D, Jenkins Hall W. Feeling cared for versus experiencing added burden: Parents' interactions with health-care providers in pregnancy with a lethal fetal diagnosis. Illn Crisis Loss. 2018;26:293–315.
Pyörälä E, Mäenpää S, Heinonen L, Folger D, Masalin T, Hervonen H. The art of note taking with mobile devices in medical education. BMC Med Educ. 2019;19:96.
Lindberg K, Mørk BE, Walter L. Emergent coordination and situated learning in a hybrid OR: the mixed blessing of using radiation. Soc Science Med. 2019;228:232–9.
Frost J, Wingham J, Britten N, Greaves C, Abraham C, Warren FC, et al. Home-based rehabilitation for heart failure with reduced ejection fraction: mixed methods process evaluation of the REACH-HF multicentre randomised controlled trial. BMJ Open. 2019;9:e026039.
Young JL, Werner-Lin A, Mueller R, Hoskins L, Epstein N, Greene MH. Longitudinal cancer risk management trajectories of BRCA1/2 mutation-positive reproductive-age women. J Psych Oncology. 2017;35:393–408.
Lewis M, Jones A, Hunter B. Women's experience of trust within the midwife-mother relationship. Int J Childbirth. 2017;7:40–52.
Mozaffar H, Cresswell KM, Williams R, Bates DW, Sheikh A. Exploring the roots of unintended safety threats associated with the introduction of hospital ePrescribing systems and candidate avoidance and/or mitigation strategies: a qualitative study. BMJ Qual Saf. 2017;26:722–33.
Castro A, Andrews G. Nursing lives in the blogosphere: a thematic analysis of anonymous online nursing narratives. J Adv Nurs. 2018;74:329–38.
Jensen AM, Pedersen BD, Olsen RB, Wilson RL, Hounsgaard L. "if only they could understand me!" acute hospital care experiences of patients with Alzheimer's disease. Dementia. 2018;19:2332–53.
Nash BH, Mitchell AW. Longitudinal study of changes in occupational therapy students' perspectives on frames of reference. Am J Occup Ther. 2017;71:7105230010p1–7.
Bright FAS, Kayes NM, McPherson KM, Worrall LE. Engaging people experiencing communication disability in stroke rehabilitation: a qualitative study. Int J Lang Commun Disord. 2018;53:981–94.
Superdock AK, Barfield RC, Brandon DH, Docherty SL. Exploring the vagueness of religion & spirituality in complex pediatric decision-making: a qualitative study. BMC Palliat. 2018;17:107.
Gordon L, Jindal-Snape D, Morrison J, Muldoon J, Needham G, Siebert S, et al. Multiple and multidimensional transitions from trainee to trained doctor: a qualitative longitudinal study in the UK. BMJ Open. 2017;7:e018583.
Cain CL, Frazer M, Kilaberia TR. Identity work within attempts to transform healthcare: invisible team processes. Hum Relat. 2019;72:370–96.
Klinga C, Hasson H, Andreen Sachs M, Hansson J. Understanding the dynamics of sustainable change: a 20-year case study of integrated health and social care. BMC Health Serv Res. 2018;18:400.
Balmer DF, Richards BF. Conducting qualitative research through time: how might theory be useful in longitudinal qualitative research? Adv Health Sci Educ Theory Pract. 2021;27:277–88.
Holland J. Qualitative longitudinal research: exploring ways of researching lives through time. ESRC National Centre for Research Methods Workshop; London: London South Bank University; 2007.
Nevedal AL, Ayalon L, Briller SH. A qualitative evidence synthesis review of longitudinal qualitative research in gerontology. Gerontologist. 2019;59:e791–801.
Download references
Acknowledgments
The authors wish to acknowledge Ellen Sejersted, librarian at the University of Agder, Kristiansand, Norway, who conducted the literature searches and Julia Andersson, research assistant at the Department of Nursing, Umeå University, Sweden, who supported the data management and took part in the initial screening phases of the project.
Open access funding provided by Umea University. This project was conducted within the authors’ positions and did not receive any specific funding.
Author information
Authors and affiliations.
Department of Nursing, Umeå University, Umeå, Sweden
Faculty of Health, Aarhus University, Aarhus, Denmark
Elisabeth O. C. Hall
Faculty of Health Sciences, University of Faroe Islands, Thorshavn, Faroe Islands, Denmark
Elisabeth O. C. Hall & Kristianna Lund Dam
Department of Health Care Sciences, Ersta Sköndal Bräcke University College, Stockholm, Sweden
Department of Health and Nursing Science, University of Agder, Kristiansand, Norway
Thomas Westergren & Liv Fegran
Department of Public Health, University of Stavanger, Stavanger, Norway
Thomas Westergren
Center for Clinical Research, North Denmark Regional Hospital, Hjørring, Denmark
Mona Kyndi Pedersen
Department of Clinical Medicine, Aalborg University, Aalborg, Denmark
Lovisenberg Diaconale Univeristy of College, Oslo, Norway
Hanne Aagaard
Department of Clinical Medicine-Randers Regional Hospital, Aarhus University, Aarhus, Denmark
Mette Spliid Ludvigsen
Faculty of Nursing and Health Sciences, Nord University, Bodø, Norway
You can also search for this author in PubMed Google Scholar
Contributions
ÅA conceived the study. ÅA, EH, TW, LF, MKP, HA, and MSL designed the study. ÅA, TW, and LF were involved in literature searches together with the librarian. ÅA and EH performed the screening of the articles. All authors (ÅA, EH, TW, LF, ÅK, MKP, KLD, HA, MSL) took part in the data charting. ÅA performed the data analysis and discussed the preliminary results with the rest of the team. ÅA wrote the 1st manuscript draft, and ÅK, MSL and EH edited. All authors (ÅA, EH, TW, LF, ÅK, MKP, KLD, HA, MSL) contributed to editing the 2nd draft. MSL and LF provided overall supervision. All authors read and approved the final manuscript.
Authors’ information
All authors represent the nursing discipline, but their research topics differ. ÅA and ÅK have previously worked together with QLR method development. ÅA, EH, TW, LF, MKP, HA, KLD and MSL work together in the Nordic research group PRANSIT, focusing on nursing topics connected to transition theory using a systematic review method, preferably meta synthesis. All authors have extensive experience with qualitative research but various experience with QLR.
Corresponding author
Correspondence to Åsa Audulv .
Ethics declarations
Ethics approval and consent to participate.
Not applicable.
Consent for publication
Competing interests.
The authors declare that they have no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1..
PRISMA-ScR checklist.
Additional file 2.
Data base searches.
Additional file 3.
Guidelines for data charting
Additional file 4.
List of excluded articles
Additional file 5.
Table of included articles (author(s), year of publication, reference, country, aims and research questions, methodology, type of data material, length of data collection period, number of participants)
Additional file 6.
Rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Audulv, Å., Hall, E.O.C., Kneck, Å. et al. Qualitative longitudinal research in health research: a method study. BMC Med Res Methodol 22 , 255 (2022). https://doi.org/10.1186/s12874-022-01732-4
Download citation
Received : 13 January 2022
Accepted : 22 September 2022
Published : 01 October 2022
DOI : https://doi.org/10.1186/s12874-022-01732-4
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Qualitative longitudinal research
- Method development
- Repeated data collection
BMC Medical Research Methodology
ISSN: 1471-2288
- General enquiries: [email protected]

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- HRB Open Res
- PMC8790707.1 ; 2021 Dec 20
- ➤ PMC8790707.2; 2022 May 6
Protocol for an exploratory, longitudinal single case study of a novel palliative care rehabilitative service
Fódhla n. ní chéileachair.
1 Department of Palliative Care, Mater Misericordiae University Hospital, Dublin, Dublin, Ireland
Bridget M. Johnston
2 Centre for Health and Policy Management, Trinity College Dublin, Dublin, Ireland
Cathy Payne
3 All Ireland Institute of Hospice and Palliative Care, Dublin, Ireland
Fiona Cahill
4 St. Francis Hospice, Dublin, Ireland
Lisa Mannion
Lisa mcgirr, associated data, underlying data.
No data is associated with this article.
Extended data
Open Science Framework: Palliat Rehab Service, https://doi.org/10.17605/OSF.IO/RA93N 47
This project contains a description of the novel service in line with the TIDieR checklist, an outline of the core foundations of the Adult Palliative Care Services Model of Care for Ireland and the elements of Palliat Rehab drawing on each foundation, and interview schedules for each sample.
Data are available under the terms of the Creative Commons Zero "No rights reserved" data waiver (CC0 1.0 Public domain dedication).
Version Changes
Revised. amendments from version 1.
Following the comments of reviewers, we now present an updated version of the Palliat Rehab protocol, which contains a number of changes in the interest of clarity and improved readability. The introduction section of the protocol now contains greater discussion of evidence in the field of palliative rehabilitation and the Adult Palliative Care Services Model of Care in Ireland, as the theoretical basis for the intervention. The methods section has been restructured to include new subsections entitled 'Intervention' and 'outcomes', and all relevant and existing information pertaining to each has now been moved under these headings. As this protocol details two components of data collection, these two components have now been clearly outlined as the 'Concurrent component', referring to data collection that occurs concurrently with the service delivery, and the 'Phased component', referring to data collection that occurs after the service delivery and that relates to the experience of relevant stakeholders. Amendments to Table 1 include a new heading of 'Eligibility Criteria for components of the study', in addition to specifying for which component(s) each sample group will be recruited. Table 2 has now been moved to the subsection 'Outcomes', as this details the specific quantitative measures to be collected. Smaller updates have been made to the Discussion and Conclusion to highlight that this protocol refers to a case study that is underway currently.
Peer Review Summary
Background: Early access to rehabilitation can improve quality of life for those with life-limiting illnesses and is highlighted as a core component of the Adult Palliative Care Services Model of Care for Ireland. Despite this, palliative rehabilitation remains under-utilised and under-developed. In 2020, the Sláintecare Integration Fund provided opportunity to pilot a novel rehabilitative palliative care service, “Palliat Rehab”. This protocol proposes a case study, which aims to advance understanding of the form, content, and delivery of the pilot service.
Methods: A prospective, longitudinal, mixed-methods, case study design will be used to describe the service and to explore the experiences of patients, informal carers and clinicians. Additionally, data collection instruments will be tested and the utility of outcome measures will be examined. Data will be collected from documentary, survey, and interview sources.
Quantitative data will be analysed using descriptive statistics, including chi-square tests for categorical variables, Mann-Whitney U tests for ordinal data, and t-tests/ ANOVA for continuous data. Qualitative data will be analysed using thematic analysis.
Conclusions: New pathways are required to advance service provision to ensure that patients receive the ‘right care, in the right place, at the right time’. This protocol outlines a case study which will aim to develop current understanding of the implementation and delivery of a novel rehabilitative palliative care service in Ireland and will consider its potential contribution to the achievement of Sláintecare goals. Investigating the service within its environmental context will lead to a better understanding of ‘how’ and ‘why’ things happen. Findings will be used to inform efforts to further develop and tailor the intervention.
Introduction
Rehabilitative palliative care has been defined as a paradigm integrating rehabilitation, enablement, self-management, and self-care into the model of palliative care to provide patients with support to enjoy the fullest possible life until death 3 . The unmet rehabilitative needs of those with serious illness are increasingly recognised- that is, the need to be normal and in control, the need for better every day functioning and mobility, and the need to alleviate the fear of being a burden 4
Interventions adopting a rehabilitative palliative care approach can benefit individuals with life-limiting illnesses 48 – 52 . Specific studies have pointed to the benefit of an exercise programme for patients with cancer-related fatigue 6 and advanced non-small cell lung cancer 7 . Recently, Nottelmann and colleagues conducted a randomised controlled trial of a novel, integrated rehabilitative palliative care programme for individuals newly diagnosed with advanced cancer and identified a benefit to their quality of life from the programme 8 . These results are increasingly relevant in the Irish context, as the number of older people living with a palliative care need in Ireland is projected to increase by 89% between 2016 to 2046 1 . This population will account disproportionately for disability burden, pain prevalence and health care use, leading to increased population health burdens and health care utilisation. It is estimated, for example, that there will be a 106% increase in requirement for the hours of healthcare delivered at home 1 . As such, rehabilitative care offers an important way for the Irish health system to re-tool to meet these challenges, yet it is an under-developed component of palliative care for all adults receiving services in Ireland 2 .
Though there may be substantial benefits to be gleaned from adopting a rehabilitative palliative care approach, difficulties implementing the approach have been noted internationally. In 2016, Thuesen and colleagues 5 conducted a literature review on the international evidence for coordination of rehabilitation and palliative care. This extensive review made notable recommendations for the implementation of rehabilitation in the palliative care approach, such as a coordinated programme that should be individualised to the needs of the patient, dynamically revised to suit their progress, and effectively assessed using outcome measures for all programme elements. Despite the growing evidence base for the benefits of offering rehabilitation programmes for individuals with palliative care 48 – 52 , the publication of Thuesen and colleagues 5 also highlighted substantial gaps in available guidelines for coordinating palliative care and rehabilitation in a single care approach. The authors concluded that there remained a lack of consensus on when and how rehabilitative palliative care should be offered and recommended that further research was required with regards to methods, activities, frameworks, and practical guidelines for service provision 5 . As such, the current knowledge base on designing, coordinating, and delivering rehabilitative palliative care interventions remains incomplete and requires greater development to facilitate the coordination of these approaches.
Rehabilitative Palliative Care in Ireland
In Ireland, the few studies which have been conducted to date on palliative care rehabilitation have been descriptive or exploratory in nature 9 – 11 , and the only interventional study that has been published has focused on health and social care professional education 12 . Rehabilitation was, however, highlighted in the Adult Palliative Care Services Model of Care for Ireland produced in 2019 2 . The Adult Palliative Care Services Model of Care for Ireland recognises the importance of rehabilitative palliative care as a core part of service provision, while acknowledging the deficits that exist in staffing and development of services 2 . The aim of the model of care is to ensure all individuals with a life-limiting illness in Ireland have access to the appropriate level of palliative care services to enhance their quality of life, irrespective of diagnosis and care setting. Included in the model of care is the optimal pathway of care for individuals with life-limiting illnesses, which entails a thorough needs assessment, initiating the correct care (e.g., specialist, generalist, integrated services), planning for ongoing and future care needs, engaging end-of-life care supports, and care for loved ones through the process of bereavement. Overall, the model of care acts as a guiding document for palliative care provision using eight core foundations to deliver an accessible and appropriate palliative care service.
Given the increasing demand for palliative care services in Ireland and the notable benefits of a rehabilitation approach in palliative care, greater coordination between palliative care and rehabilitation services is likely to prove a valuable approach in the health service. Greater integration of rehabilitation into palliative care in Ireland also aligns with the goals of healthcare reform in Ireland, as outlined in the Sláintecare Report. Established in 2017, Sláintecare is a ten-year reform programme in Ireland aimed at providing a more efficient and universal healthcare services, including the commitment to develop universal palliative care 13 , 53 . Responding to the urgent need to provide support to the healthcare system to test and scale ideas that meet Sláintecare goals, the Sláintecare Integration Fund was established in 2019. The Fund aims to support projects that:
- Demonstrate innovative ways in which citizens can engage in their own health,
- Represent best practice in the management of chronic diseases and caring for older people, and
- Encourage innovations in shift of care to the community or promoting hospital avoidance.
Following application to the Fund, our team was awarded a grant to deliver an integrated rehabilitation service for patients with palliative care needs and to conduct an exploratory, longitudinal case study. The novel intervention draws on the core foundations of the Model of Care 2 as a means of enhancing research and innovation capacities in palliative care by examining the feasibility of providing the integrated service between hospital and community care settings. A description of each core foundation is available in the Extended Data, accompanied by a brief outline of elements in the intervention drawing upon each one. The case study aims to advance understanding of the form, content, and delivery of the novel rehabilitative palliative care service (‘‘Palliat Rehab’’) in the provision of specialist palliative care for academic, policy and practice purposes.
This is a protocol for a case study which will examine a palliative rehabilitation intervention. The specific study objectives are:
- To describe the novel rehabilitative palliative care service that spans hospital and community settings.
- To explore the experiences of patients, informal carers and clinicians while receiving or providing the service.
- To test data collection instruments and examine the utility of selected outcome measures.
Guided by an exploratory case study framework 16 , and adopting a post-positivist approach 17 , this case study will examine the novel service, as delivered by one hospital organisation and one community-based organisation, for an 18-month period of service provision and will provide insight into the delivery of palliative care rehabilitation. ‘Palliat Rehab’ is a new service initiative, and a case study design was chosen because of the need to capture information to answer ‘how’, ‘what’ and ‘why’ questions using a naturalistic method 14 . Case studies allow for investigation of a contemporary phenomenon within its real-life context when the boundaries between phenomenon and context are not clearly evident 14 and provide an in-depth, multi-faceted understanding of issues that can help develop or refine theory 15 .
The scope of our study includes the rehabilitation service, the staff delivering the service, and the direct and indirect recipients of the service (patients and informal caregivers/family members). This study will comprise two components of data collection: a ‘concurrent’ component, where routine, quantitative data will be collected from participants during the intervention sessions, and a ‘phased’ component, where patients will be invited to contribute data on their experiences of Palliat Rehab using a quantitative survey and during semi-structured, qualitative interviews. Their informal caregivers and relevant staff members will also be invited to engage in semi-structured interviews on their views of the service as an additional element of the phased component. In doing so, the study will contribute to opening the ‘black box’ of palliative care rehabilitation interventions and provide transferable knowledge that will be of value to the future development of interventional studies of service delivery.
Study setting
The rehabilitation service will be provided by the Mater Misericordiae University Hospital (Mater Hospital) and St Francis Hospice for an 18-month period.
The Mater Hospital is a 630-bed teaching hospital providing local services for its catchment population of Dublin’s north inner city and a range of specialist services on a regional and national level. St Francis Hospice Dublin is a specialist palliative care service organisation providing in-patient, out-patient, and home-based services to people with progressive, life-limiting illness in the North Dublin area. The rehabilitation service will be delivered by a hospital-based senior occupational therapist and a community-based senior physiotherapist, both of whom work as members of specialist palliative care teams.
Eligibility Criteria
The case study will recruit participants from the specialist palliative care services of the Mater Hospital and the community palliative care services of St Francis Hospice Dublin. Overall, the following three groups of participants have been identified and will be recruited during this case study: patients who receive Palliat Rehab, informal caregivers/ family members of patients receiving the rehabilitation service, and staff engaging in either the design or delivery of Palliat Rehab.
For patients receiving palliative care in the Mater Hospital or in St. Francis Hospice, referral to Palliat Rehab will depend on a palliative needs assessment, where severe ill-health, symptom burden and/or cognitive deficit may preclude individuals from taking part. Needs assessments comprise holistic assessments of individual need that include, but are not limited to, assessment of physical condition, appraisals of pain, examination of function and mobility, discussion of potential difficulties completing activities of daily living, and identifying goals patients may have for their care. As rehabilitation needs can vary substantially between individuals and their conditions, however, inclusion will be determined on a case-by-case basis. If the specialist palliative team think that an individual has a rehabilitation need that could be met by the service, then the new service will be explained and offered to the patient by a team member. Specific eligibility criteria for each group have been highlighted in Table 1 , where criteria for patients refers to both the concurrent and phased components, and criteria for caregivers and staff refers to the phased component.
Intervention
Palliat Rehab will be delivered by an occupational therapist in the Mater Hospital and a physiotherapist in St. Francis Hospice. It has been observed that rehabilitation is best described as a process containing specific actions 21 , and for this reason, the bundle of interventions, based on individual rehabilitation needs, will be investigated rather than specific components. The occupational therapist and physiotherapist delivering Palliat Rehab will engage with the patients directly about their rehabilitation wants and needs and will construct individualised plans on a case-by-case basis. As the specific elements of each patient’s experience will vary, no set number of intervention sessions have been planned. The number of intervention sessions will depend on the patient’s health, their desire to continue with the service, and their ongoing connection with either the Mater Hospital and/or St. Francis Hospice. A description of the intervention service based on TIDIER criteria is available in the Extended data.
This case study will collect multiple outcome measures to describe the intervention, to explore the experiences of participants, and to assess the utility of particular quantitative measures for such an intervention. The quantitative outcome measures to be collected from consenting patient participants during the concurrent component are divided into three categories (demographic, service-usage, and health and symptom data) and are listed in Table 2 . By collecting these three categories of data, it is anticipated that this case study will be equipped to adequately describe the sample served, the experience of patients receiving the intervention, and the feasibility of embedding the service into the existing healthcare infrastructure using service-usage data. All quantitative data measures will be collected once following initial enrolment of each patient, with the exception of the Palliative Care Outcomes Collaborative (PCOC) scale, which will be collected at baseline during the first intervention session and repeatedly collected during each session thereafter.
For the phased component, patients receiving Palliat Rehab will be asked if they are willing to contribute survey data based on their satisfaction with the service. Outcomes relating to the phased component of the case study also include the qualitative interview data collected from all three participant groups to effectively explore the general experiences and views of the service from the patient, informal caregiver, and staff perspective.
Sample size
The sample size for a case study depends on the number of participants that is sufficient to describe the phenomenon 18 . As this case study design comprises two components, namely the concurrent component and the phased component, the rationale for each component’s sample size is described below.
Concurrent Component
The aim of the case study is not to test the rehabilitation service, therefore it would not be appropriate to use traditional power calculations when considering sample size for the quantitative data collection component of the case study. 20 The purpose of quantitative data collection in the case study is to contribute to the understanding of care delivery and stakeholder experience and to test data collection instruments and examine the utility of selected outcome measures. Considering the issue of justification of sample adequacy, anonymised, routine data will be collected on all patients who receive the service. , and all eligible patients will be offered the opportunity to participate in survey data collection.
Phased Component
Following the concurrent component, all patients who receive Palliat Rehab will be offered the opportunity to participate in a survey detailing their satisfaction with the service. The second element of the phased component refers to the qualitative interviews. As sample size estimation for qualitative interview samples is an area of conceptual debate and practical uncertainty 19 , the projected sample size is based on the concepts of data adequacy and research practicality. The population included within this case study is relatively homogeneous, as participants will be availing of one single palliative care rehabilitation service. A sample of 16–22 individuals will therefore be recruited for qualitative data analysis across three stakeholder groups; patients receiving the service (n= 4 –6), family members of individuals receiving the service ( n = 4–6), and clinicians involved in the design and/or delivery of the new service ( n = 8–10).
Recruitment
Patients. All potential participants will be provided with an information leaflet detailing the purpose of the data collection, the potential risks and benefits to participation, and data protection rights. Following a minimum of 24 hours, potential participants will be asked whether they are interested in being contacted by a researcher to discuss participation in the concurrent and phased components. Patients will be assured that they may receive Palliat Rehab through the concurrent component without further engaging in the phased component of the study. Once a patient receives input from the service, a researcher will make telephone contact with individuals who indicate that they are willing to be contacted and enquire if they are interested in participating in the phased component.
Caregivers. Patients receiving ‘Palliat Rehab’ will also be asked by either the physiotherapist, occupational therapist, or consultant to consider whether they wish for their primary caregiver to also be invited to participate in a separate Zoom or telephone interview. It will be explained that the reason for inviting their caregiver to participate is to include caregiver perspectives in the research study. It will again be emphasised that their decision or that of their caregiver will not influence the patient’s care in any way. Following a minimum of 24 hours and allowing sufficient time for the patient to discuss the matter with his/her caregiver, the patient will be asked whether their caregiver is interested in being contacted by a researcher to discuss participation. A researcher will telephone individuals who indicate that they are willing to be contacted and answer questions and provide information, as needed.
Staff. Clinical staff who have been involved in the design and/or delivery of the palliative care rehabilitation service will be invited to take part in two interviews by the Principal Investigator (PI). The researcher will provide the potential participant with written information on the study and the consent form and will be available to answer further questions, as needed. Both interviews will be separated by a minimum of 6 months to contrast learnings and applications of developed knowledge during the piloting of the intervention. It will be explained that the reason for inviting the staff member to participate is to include the perspectives of health and social care professionals in the study. Information will be provided to them regarding the study, the potential risks and benefits to participation, and data protection rights. It will be emphasised that the decision of the staff member will not influence or affect their career or work relationships in any way. If the staff member expresses interest in participating, the PI will send an individualised email introducing the staff member to the researcher.
Data collection
Using a mixed-methods approach, multiple sources of quantitative data will be collected in a sequential manner. Quantitative data collection will take place from service commencement, while qualitative interviewing will take place at two points- approximately 4–6 months after commencement of the service and in the final two months of service provision.
Quantitative data. Quantitative measures will include data that is recorded as a necessary or usual part of palliative care or rehabilitative palliative care service provision during patient assessments in patient charts or electronic patient records. All quantitative measures are summarised in Table 2 under three category headings: demographic data, service-usage data and, health and symptom data. Following the establishment of informed consent from patients, demographic, service use and health and symptom data necessary for the delivery of care will be collected by the service’s occupational therapist and/or physiotherapist. As part of the phased component, survey data on patient satisfaction will be collected on completion of engagement with the rehabilitation service intervention.
Qualitative data. Semi-structured interview schedules for the first set of interviews for each group of participants were developed using a five-step framework of design 26 . The five steps are as follows: (1) identifying the prerequisites for using semi-structured interviews; (2) retrieving and using previous knowledge; (3) formulating the preliminary semi-structured interview guide; (4) pilot testing the guide; and (5) presenting the complete semi-structured interview guide. Interviews across all three participant cohorts may take place in person or remotely according to the participant’s preference. Only an audio recording will be made regardless of method of interview. Interviews are estimated to last approximately 30–40 minutes and protocols will be piloted with volunteers in St. Francis Hospice to ensure question clarity, in addition to monitoring time demand.
Data management
Potential participants personal data will be processed under article 6 (1)(e) Public Interest and under article 9 (2)(j) Scientific Research of the General Data Protection Regulation (GDPR) 2016 27 , and data will be secured in accordance with the requirements of the Data Protection Act (2015). Data will be anonymised and where applicable, pseudonyms will be used in reports and publications.
Analytic plan. Data analysis will be iterative and will continue over the course of the study.
Descriptive statistics will be generated using R 28 to summarize participant characteristics across demographic and service usage domains, where categorical variables will be reported as raw numbers and percentages. Reports of continuous variables will include mean, median, range and standard deviation values. For repeated measures analysis of health and symptom data pre- and post-service engagement, significance of variations will be determined using x 2 tests or Fisher’s Exact Test, when required, for categorical data, Mann-Whitney U tests for ordinal data, and t-tests/ ANOVA for continuous data . 95% confidence intervals (CI) will be used, and significance levels will be assessed at the alpha level of .05.
Interview audio will be transcribed using Happy Scribe (2021) transcription software and reviewed using original audio-recordings to ensure accuracy, the removal of identifiable information and to engage in data familiarity. For qualitative data, reflexive thematic analysis 29 – 31 will be used to generate descriptive themes related to the experiences and perspectives of stakeholders on the novel service. Thematic analysis was selected for analysis given its flexibility in application, enabling the collation of differing perspectives and the iterative construction of common themes.
Coding will be conducted both inductively and deductively using the open-source QDA Miner programme (version Lite), where inductive coding will entail annotating similarities and intriguing features across the dataset. Deductive coding will comprise the construction of a deductive codebook based on the core foundations of the Adult Palliative Care Services Model of Care 2 , and contemporary literature on rehabilitation, integration and palliative care 32 – 34 .
Coding will be completed by three researchers forming a coding team with diverse academic backgrounds in health economics, rehabilitative palliative care, and psychology. These researchers will not be involved in the provision of the rehabilitative service. Coding will be completed through individual coding sessions and facilitatory discussions to gauge differences in interpretation and to fully explore the breadth of data collected. As the dataset will be coded progressively, base codes will be continually revised and refined in response to new facets of data. Theme construction will then be facilitated by the design of a coding tree to identify similar concepts generated during the coding process. To ensure regular reflection during the analytic process, a reflexive log will be maintained to track and detail aspects of the coding process to identify potential assumptions underlying their approach 31 . Qualitative analysis will be reported in line with the COREQ reporting guidelines 45 .
The construct validity, internal validity, external validity, and reliability of the data will be established through use of the following methods. First, the use of a protocol and exact documentation of each step of the process facilitates traceability 35 . Second, the use of multiple methods increases validity by providing multiple perspectives on the same phenomenon 35 . Third, a researcher diary will be used to record thoughts, feelings, and expectations that may at a later stage be used for data analysis 36 . Fourth, a well-structured database will be used for data management and will serve as the evidentiary source of conclusions 35 . Fifth, analytical techniques during data analysis such as explanation building and addressing rival explanations will be employed 37 . Sixth, the multidisciplinary composition of the team will allow the researchers to raise questions throughout the course of the study, particularly regarding the fit between the methods used and the results obtained, and study conclusions 37 . Finally, thick description will establish transferability 38 . Convergence of quantitative and qualitative data will be undertaken to describe the service and its implementation from the perspectives of patients, informal carers and clinicians.
The research protocol has been approved by the Mater Misericordiae University Hospital (IRB Ref 1/378/2113) and St Francis Hospice Dublin (Rec. approval 16/1/20).
The case study will be conducted in accordance with the ethical standards of the organisations and with the 1964 Helsinki declaration and its later amendments 39 . The protocol was designed giving consideration to best practice in palliative and rehabilitative care and ensuring that risks (e.g., participant distress occurring during interview) will be minimised to the greatest possible degree for patients, carers and staff. The autonomy of participants will be respected by providing informed choice. All participants will receive oral and written information prior to the interview, and written informed consent will be obtained prior to interview. Participants will be allotted a minimum time period of 24 hours to consider their interest in participating.Additionally, all participants will be informed that they may withdraw from the study, and/or withdraw their data, at any point without affecting their access to services. All data will be anonymized and will not be identifiable and will be managed securely.
Public and patient involvement
Due to required timeframes and available resources, public involvement in the development of the case study protocol has been at level one of the Public Participation Spectrum 40 developed by the International Association for Public Participation. A virtual meeting was held with members of Voices4Care in March 2021 where the study protocol was presented, and a question-and-answer session held. Voices4Care is an initiative of All Ireland Institute of Hospice and Palliative Care (AIIHPC) – an all-island organisation working to improve palliative and end-of-life care for patients and their families. Voices4Care is a volunteer group with members comprising people living with a life-limiting illness/with palliative care needs, informal carers of adults with palliative care needs, and people from the wider community interested in palliative care.
Dissemination plans
In keeping with the mission of the research to develop service provision and meet patient needs, knowledge exchange activities will be undertaken to support a dissemination plan that reaches the public, health and social care professionals and policy makers. Dissemination materials will be developed to meet the needs of individual groups and a final project report will be provided to the Sláintecare Programme Implementation Office. Additionally, the case study will be submitted for publication in a peer-reviewed journal. Findings will be presented at national and international meetings. A project webpage has been created and may be accessed at https://palliativerehab.ie/ . Information will also be shared via the Rehabilitative Palliative Care Slaintecare Project Twitter feed (@PalliativeRehab).
Study status
Data collection commenced in February 2020 but was interrupted by the COVID-19 pandemic. The palliative care rehabilitation service was suspended for a three-month period and data collection re-commenced in July 2020. Preliminary data collection is due to finish on December 31 st , 2021,with follow-up interviews with professional staff expected to be completed by May 2022.
Overall, this case study will examine Palliat Rehab by (i) outlining the structures and components of the integrated service, (ii) investigating the perspectives of key stakeholders, and (iii) analysing the chosen outcome measures for suitability in the intervention. Given the projected increases in both palliative care and rehabilitative needs among the Irish population over the next two decades 1 , this case study is likely to uncover valuable insights into offering an accessible and integrated services to meet these growing demands. Moreover, Palliat Rehab will uphold the aims of Sláintecare reform in the Irish healthcare system, which seeks to achieve a universal single-tier health and social care system where everyone has equitable access to services based on need, and not ability to pay 53 . Core Sláintecare goals are the achievement of a shift in care from the acute to the community setting to bring care closer to home for service users, and a focus on enablement and well-being. Palliative rehabilitation aligns well with these objectives as it seeks to integrate enablement, self-management, and self-care into the holistic model of palliative care.
Despite being recognised as an essential part of palliative care service provision 2 , rehabilitation services remain under-developed and under-utilised in Ireland and beyond. New pathways and models of care are required to advance service provision to ensure that patients receive the ‘right care, in the right place, at the right time, by the right people’. The development of ‘‘Palliat Rehab’’ offers opportunity to study an innovative service and consider its potential contribution to the achievement of Sláintecare goals. Investigating the rehabilitation service in-depth and within its environmental context will lead to a better understanding of ‘how’ and ‘why’ things happen. Case study findings will be of value in assessing whether there is evidence that supports the rehabilitation service, and will be used to inform efforts to further develop and tailor the intervention.
Limitations
Several limitations should be considered. The rehabilitation intervention is being delivered during a period of great change within health services that has been precipitated by the pandemic. This has resulted in a period of suspension of the service but has also impacted on usual ways of working (e.g., the requirement for physical distancing, utilisation of remote forms of communication). Detailed contextual description will be provided to enable others to understand the effect of the pandemic on service provision.
The case study will appraise the suitability of selected outcome measures for use within the rehabilitation service. This is of particular importance given that the clinical usefulness of function and mobility-based outcome measures for individuals receiving specialist palliative care are currently a topic of debate 41 , 42 . Selecting an appropriate outcome measure is a critical step in designing valid and useful clinical trials and outcome studies, as the best design cannot make up for the use of an inappropriate measure. It is possible that the quantitative measures may have limited utility in contributing to knowledge of effectiveness. However, the application of mixed methods methodology will ensure that the strengths of one approach complements the restrictions of another and qualitative data will be used to understand the meaningfulness, or otherwise, of the quantitative outcomes. While the design of the Palliat Rehab service was informed by expert opinion and the evidence base, the staffing of the team was limited by funding availability and the required timelines of the project. Case study findings will provide important data on this issue.
This case study aims to advance our knowledge of the implementation and delivery of a novel rehabilitative palliative care service in Ireland. By providing an in-depth description of the experiences of patients, carers and health and social care professionals, a better understanding of the ‘how’ and ‘why’ (or ‘why not’) of the service’s perceived effectiveness will be obtained. Findings will be used to develop and tailor the intervention and will inform the development of future interventional studies as part of the journey towards evidence-based service provision.
Data availability
[version 2; peer review: 2 approved, 1 approved with reservations]
Funding Statement
Funding was provided by the SláinteCare Integration Fund [Grant ID Number: 267, Assigned to Principle Investigator Prof. Karen Ryan].
Reviewer response for version 2
Jongkyu kim.
1 Department of Physical Medicine and Rehabilitation, Seoul Medical Center, Seoul, South Korea
Thank you for your enthusiasm to this research. I totally agreed with your responses. And I am hoping your next step of the Palliative Rehabilitation program.
Is the study design appropriate for the research question?
Is the rationale for, and objectives of, the study clearly described?
Are sufficient details of the methods provided to allow replication by others?
Are the datasets clearly presented in a useable and accessible format?
Not applicable
Reviewer Expertise:
Rehabilitation for the patients who taken care of pallitive care.
I confirm that I have read this submission and believe that I have an appropriate level of expertise to confirm that it is of an acceptable scientific standard.
Reviewer response for version 1
Jette Thuesen
2 Department of Public Health, Unit for User Perspectives and Community Interventions, University of Southern Denmark, Odense, Denmark
3 Center for Nutrition and Rehabilitation, Absalon University College, Holbæk, Denmark
Mai-Britt Guldin
1 REHPA, The Danish Knowledge Centre for Rehabilitation and Palliative Care, Odense University Hospital, Odense, Denmark
Dear Colleagues,
Thank you for this manuscript. We were excited to read that you had undertaken developing a protocol on a case study of a novel palliative care rehabilitation service. We think this is exactly the type of study that can lift this novel research area. Therefore, we appreciate the subject of your study.
This is a description of a protocol for a prospective, longitudinal, mixed-methods case-study design that describes a novel early access palliative rehabilitation service. The study will explore the experience of patients, carers, and clinicians by using documentary, survey and interview data.
While the topic is important and certainly of interest in promoting novel and early access to rehabilitation, the manuscript in its current form suffers from some important limitations which detract from its quality. Revisions are necessary to make the manuscript ready for indexing.
Below we have commented on some specific points that we find would improve the readability and validity of the study.
Introduction:
- Our main point in the introduction is that the references are not clear and the background for a palliative rehabilitation intervention should be clearer. Is reference # 3 a book?
- It is quoted that there is ‘growing evidence base’ on palliative rehabilitation, but it is not backed with references? A systematic literature search should give you an overview of several palliative rehabilitation intervention studies completed within the last ten years. To mention some, Feldstein and colleagues have published several papers on their interdisciplinary palliative rehabilitation program in 2016-2018.
- We would suggest also visiting the palliative rehabilitation projects from King’s College, London. Finally, we would suggest that the theoretical underpinnings of a palliative rehabilitation service are described better and the reference to The Adult Palliative Care Services Model for Ireland is supplemented with a figure or table that shows its contents. This would lift the understanding of the need for a palliat rehab service further, and make the service model much clearer to the reader and therefore the study protocol more transparent. We would also shorten the introduction regarding the Slaintecare goals in order for it to be interesting to a wider readership, or it needs to be apparent why this is important information to understand this protocol and the reader.
- The aim of the paper is to describe the protocol. However, the authors have chosen to describe the aims of the case study. This gets very confusing. We would suggest describing the aims of this paper clearly – which in our opinion is to present a protocol - and it would be of great help for a clear manuscript that a guidance is used for presenting a protocol. For instance the SPIRIT-statement.org or another guidance. Further, it would also be helpful with a development model or theoretical model to underpin the development and description of the protocol. This should preferably be differentiated from the aims of the case study. Moreover, the development of the palliative rehabilitation intervention might have been framed by a complex intervention development model such as the one described by Bleijenberg et al (2018). This would help you to structure the different background factors for designing the intervention (e.g. problem identification and definition, patient’s needs, theory, evidence etc).
- In the description of methods, we think the authors succeed in presenting why the case study design is the most appropriate for the proposed study. Nevertheless, also here the paper needs to be differentiated between this paper/the protocol and the study design which is described for the future study.
- There seems to be some points of confusion regarding the methods (and therefore a guidance on presenting protocols would be helpful): Initially, the study is described as an 18 months period. Later it is described as a 15 month period. The same point about sample size. Initially, it is described as ‘a single, holistic case’. Later it is described as ‘the sample size…depends on the number of participants that is sufficient’ and later again ‘a purposive sample of 16-22 individuals...’. Study setting and recruitment (sample) have repetitions which could be more omitted. These points need to be clearer, more aligned, and maybe even shorter so it is not stating the obvious.
- Additionally, it also seems the section about Sample also describes types of data that will be collected. Consider if these should be described under data collection instead.
Participation selection and recruitment:
- Eligibility assessment is described thoroughly and maybe a little lengthy. We would recommend shortening to ensure clarity and readability. Recruitment is also described at length and with other information in between. The recruitment procedure is difficult to get a clear picture of and could even profit from a figure with a flow chart which shows the procedure rather than the lengthy description. This would enhance transparency.
- Be aware that both in Sample and in recruitment, data sources are described. It would make the study more reader friendly to put all description on data sources under data collection.
- Maybe it could also be considered to differentiate between recruitment and study procedure. It seems both types of descriptions are put in the same long section. This makes it harder to understand.
- The section on ‘As discussions involving an individual’s experience with a life-limiting illness…’ is really about ethical considerations and would deserve to be moved to the ethics section of the protocol.
- Finally, we applaud the use of TIDIER to describe the service. However, we miss a whole section on describing the form and content of the intervention. Otherwise, the protocol seems incomplete and too abstract and ultimately uninteresting to a wider readership.
Data collection:
- We miss an overview of the case study’s research questions and the methods and materials. It is not clear what is actually being investigated by the methods mentioned.
- A suggestion could be to add a table that provides an overview of the different phases in the study procedure, the participants and which types of data are collected in the different phases. We had to read these aspects several times to grasp the idea of it.
- According to the health and system data, mentioned in table 2, it is not clear why these specific measures are being applied. We miss some arguments for selecting them as the most relevant measures to evaluate the goals of palliative rehabilitation. We suggest that the authors reflect on what are the relevant goals of palliative rehabilitation – and how should they be measured.
- Further, all the quantitative measurements scales that are proposed really should be presented with information on whether they are validated and can be compared to a larger data set (as this study only will collect data on very few participants). Measurement points should be presented together with measures.
- It is described, that the bundle of interventions will be investigated rather than specific components. How does that align with the ambition of ‘opening the black box’ as mentioned earlier in the paper.
- Finally, we would suggest to pay attention not only to the patients that are being included in the study but also to the patients choosing not to take part and to the dropouts as well. Previously, palliative rehabilitation intervention studies have documented a remarkable difference between patients who were considered eligible, patients who were included, and patients that completed (Chasen et al 2013; Jones et al 2013).
Data management:
- Data analyses of quantitative data should be seen according to the very small N of the study. Hence, there needs to be a reflection of the appropriateness of the statistical analysis plan – preferably with reference to former studies on the subject.
Public and patient involvement:
- This section is very hard to understand for a reader outside of Ireland. Authors could consider the international readership of the journal and make this section more widely understandable as there surely are good points to learn from.
Discussion:
- This section refers to The Slaintecare Report and Core Slaintecare goals. Unfortunately, as these have not been fully presented in the manuscript, this discussion does not seem readily understandable or even relevant to understand this protocol. Authors need to consider what is relevant information for the reader and for the presentation of the protocol.
Conclusion:
- As has been mentioned under introduction and aim, it is also relevant in the conclusion to differentiate between ‘this paper’ and the case study.
Best of luck with your manuscript.
Mai-Britt Guldin: Palliative Rehabilitation and Palliative Care Research and Education Jette Thuesen: Palliative Rehabilitation and Rehabilitation Research and Education
We confirm that we have read this submission and believe that we have an appropriate level of expertise to confirm that it is of an acceptable scientific standard, however we have significant reservations, as outlined above.
Thank you for your great study protocol. It is very interesting and I am looking forward to the result from this study protocol.
Major recommendations:
- This study protocol is for the program of 'Palliat Rehab', but showed only a webpage address. If possible, could you explain the summary of the 'Palliat Rehab' program contents?
- For the data and measures, a previous study for rehabilitation of palliative care patients noticed patients' satisfactions and dissatisfactions (Lee et al. (2018 1 )). Could you add measurements about patients' and caregivers' satisfaction?
I confirm that I have read this submission and believe that I have an appropriate level of expertise to confirm that it is of an acceptable scientific standard, however I have significant reservations, as outlined above.
Fódhla Ní Chéileachair
Mater Misericordiae University Hospital, Dublin, Ireland
Dear Dr. Kim,
We are delighted you took the time to review the article and welcome your comments!
In relation to the key components of Palliat Rehab, we would like to direct you to the OSF storage link in the Extended Data section, as a brief description of the service is available as a downloadable document in this file. Indeed, we do stress that differences are likely to be seen between the rehabilitation plans constructed for participants, as the service will be based on individual needs, and provided this service description as a broad overview of the Palliat Rehab programme. We also agree that an evaluation of patients' and caregivers' satisfaction would be a welcome addition. Unfortunately, the programme is currently underway, however we are keen to gather qualitative data on the experiences of patients and their caregivers using semi-structured interviews.
Many thanks for your contribution and your review. We look forward to disseminating findings of the current programme soon!
With best wishes,
Lubayna Fawcett
1 Physical Therapy Department, Mayo Clinic, Scottsdale, AZ, USA
2 Arizona State University, Tempe, AZ, USA
This article will contribute to the much needed 'way forward' in palliative rehabilitation. The study settings and sampling as well as the outcome measures tools can all be easily implemented/replicated even in low income countries.
In addition, this article underscores the essence of comprehensive palliative care, in which palliative rehabilitation is the critical and missing component by which to improve the quality of care for people with serious illnesses.
Palliative Rehabilitation/Cancer Care/Women's Health.
Dear Dr. Fawcett,
We're delighted with your comments on the protocol. Many thanks for taking the time to review this publication.
Install the app
Install this application on your home screen for quick and easy access when you’re on the go.
Just tap Share then “Add to Home Screen”
You are currently browsing offline
Discover ECPR's Latest Methods Course Offerings
I agree to receive your newsletters and accept the data privacy statement.
We use Brevo as our email marketing platform. By clicking below to submit this form, you acknowledge that the information you provided will be transferred to Brevo for processing in accordance with their terms of use .
Longitudinal Case Studies
Course dates and times.
Monday 8 to Friday 12 August 2016 Generally classes are either 09:00-12:30 or 14:00-17:30 15 hours over 5 days

Institution: Central European University
- Need to Know
This course is designed for students intending to use longitudinal case study methodology in their research projects. It will be especially useful for PhD students who are working on their theses, postdoctoral fellows who are transforming their theses into a monograph or series of articles as well as assistant professors who wish to employ longitudinal case study research in their published work. The course introduces the method of longitudinal case study analysis (LCA) as a hybrid of (1) process-tracing, (2) periodized within-case research design, and (3) historical comparative analysis (HCA)—combining different techniques for hypothesis testing by slicing and dicing the empirics within a single case study over time and, as a second step, extending these comparisons to one or more similar case studies across space. The course is heavily weighted toward examples, class exercises and workshopping student assignments, with significant instructor feedback. As such, the course is intended to guide students through the process of fitting an appropriately tailored longitudinal case study design to their research question, formulate a plan for testing their hypotheses using within- and cross-case temporal variation, develop a plan for approaching, collecting and analyzing data in the field, and, finally, writing up the results in a convincing narrative style.
Instructor Bio
Erin K. Jenne is a professor at CEU's Department of International Relations, where she teaches MA and PhD courses on qualitative and quantitative methods, nationalism and civil war, foreign policy analysis, international relations theory, ethnic conflict management, and international security.
Erin received her PhD in political science from Stanford University with concentrations in comparative politics, international relations and organisational theory.
She has received numerous grants and fellowships, including a MacArthur fellowship at Stanford University, a Center for Science and International Affairs (BCSIA) fellowship at Harvard University, a Carnegie Corporation scholarship, and a Fernand Braudel fellowship at European University Institute (EUI) in Florence, and a MINERVA Initiative grant on Chinese soft power from the US Department of Defense.
Erin recently published her second book, Nested Security: Lessons in Conflict Management from the League of Nations and the European Union (Cornell University Press, 2015). Her first book, Ethnic Bargaining: The Paradox of Minority Empowerment (Cornell University Press, 2007) won the Mershon Center’s Edgar S. Furniss Book Award in 2007 and was named a Choice Outstanding Academic Title by Choice magazine. Ethnic Bargaining is based on her dissertation, which won the 2001 Seymour Martin Lipset Award for Best Comparativist Dissertation.
She has published numerous book chapters and journal articles in International Studies Quarterly, Security Studies, Regional and Federal Studies, Journal of Peace Research, Civil Wars, Ethnopolitics, International Studies Review, Journal of Democracy, Research and Politics and PS: Political Science and Politics, Research and Politics and Europe-Asia Studies (forthcoming).
She currently sits on the editorial boards of Ethnopolitics, Foreign Policy Analysis , International Studies Review , and has served in several capacities on the Emigration, Ethnicity, Nationalism and Migration Section of the International Studies Association, the Association for the Study of Nationalities and the Comparative Politics Section of the American Political Science Association.
@erinjenne
Why did women gain substantive economic or political rights in some Islamic countries but not in others? What accounts for the variation in democratic consolidation across the countries of the post-communist world? Why did some advanced industrialized democracies implement extensive social welfare programs, but not others? While traditional comparative analysis promises answers to such questions, a full explanation often requires integrating primary record and field analysis with longitudinal data displays to build and test analytical narratives that can be generalized to all cases that meet the theory’s scope conditions.
Longitudinal Case Analysis (LCA) is a research tradition that combines techniques from historiography and longitudinal data analysis with those of John Stuart Mill’s comparative method and process-tracing to test social science theories that contain causal processes that are both long and/or slow-moving but that also involve micro-level causal mechanisms that play out during periods of rapid transition or change. Researchers have used LCA to explore topics ranging from the emergence of civil wars to collective action to the emergence of international norms and institutions. The study of these phenomena does not lend itself easily to quantitative or experimental analysis, but are instead well-served by joint-longitudinal-comparative analysis of multiple cases over time—which may be years, decades, or in rare cases, centuries.
The course is divided into three main parts: (1) developing theory and specifying causal mechanisms (paying close attention to the temporal component), (2) formulating the research design and planning data collection, and (3), establishing techniques of causal inference and writing up the cases in a compelling narrative form. Throughout, equal time is spent on seminars and workshops--a format that is intended to assist students in developing longitudinal case study designs tailored to their specific research agendas .
In the first part of the course (days 1 and 2), we explore the advantages and limitations of this hybrid method and discuss the range of research questions that lend themselves to LCA. We begin by exploring the principles of historical comparative analysis (used to assess theories of long and/or slow structural change), as well as periodized longitudinal analysis (used to assess causal mechanisms that recur through time), and finally process-tracing (used to assess causal mechanisms that involve rapid change. We discuss different ways in which these approaches can be combined to conduct longitudinal case studies that can test for complex causal processes hypothesized by the researcher (including case periodization, critical junctures, stable/unstable equilibria, feedback and cascading effects, agency and institutional change).
The key is to exploit the considerable within-case variation over time as well as across cases to adjudicate between competing accounts for the outcome of interest. In so doing, we not only establish the importance of a well-specified causal mechanism, but also explore various indicators that can be used to test for (and demonstrate) the mechanics of change within a single case over time. The first part of the course is thus devoted to developing a research design that combines a selection of techniques (e.g., at the macro-level, event periodization and small-N case selection; at the micro-level, interpretative document and/or ethnographic analysis) in a way that is adapted to the research question at hand.
The second part of the course (days 3 and 4) are aimed at executing the research design. Here, we cover the different types of data that are used in such work, including (1) archival data or primary sources), (2) secondary (usually scholarly) sources, (3) running data such as statistical records, and (4) interview or field data drawn from subjects who have first-hand memories of these phenomena. We discuss how to locate and record these data and how to use them separately or in combination, depending on the phenomenon to be explained as well as the hypothesized causal mechanism(s). The fourth day is devoted to the problem of causal and descriptive inference in over-time case study analysis. Threats to causal inference such as measurement validity and reliability are discussed as well as the problem of endogeneity, reverse causation and equifinality. We discuss how to handle these threats, which are endemic to qualitative case analysis, by using nested analysis, various techniques of external content and construct validation.
The third and final part of the course ( day 5 ) asks what makes a case study convincing to the reader. We examine different approaches toward developing an effective and convincing narrative form in the case ”write-up.” On day 5, we cover how to structure the data in a manageable format. We explore the usefulness of different software programs for ordering the data so that the researcher can ”see” the story and select a narrative style with which to “write up” the cases in a way that demonstrates the validity of the author’s causal argument. One example of this is the ”analytical narratives” approach in applied economics, which aims to demonstrate the logic of formal theories through a systematic exploration of a case study using a select set of data and empirics. A good analytical narrative is at once a compelling story told with “flair,” and a convincing investigative report; the aim is to both persuade and seduce the reader. When done well, these longitudinal case studies can linger on in the reader’s mind, giving life to an otherwise dull, abstract and ultimately forgettable theory. While specifically designed to complement formal game theory, the analytical narrative is equally well adapted for testing and illustrating less formalized theory.
This course does not have any special prerequisites, but students should have a basic familiarity with the comparative method and qualitative research design.
Software Requirements
There are no software programme requirements for the course, although there will be demonstrations of how various field (interview/archival/bibliographic) data management systems (all freeware or with free trial periods) can be used in the context of longitudinal case study analysis and write-up. Students will be notified in advance of the course as to which programmes will be demonstrated in the class, should they choose to download it in advance of the course.
Hardware Requirements
None - see software requirements, as participants may wish to bring their own laptops.
Archival Research
Lindsay Prior, “Repositioning Documents in Social Research,” Sociology , Vol. 42, No. 5 (2008), pp. 821-836.
Victor Jupp, “Documents and Critical Research,” in Roger Sapsford and Victor Jupp (eds.) Data Collection and Analysis (Sage Publications, 1996), pp. 298-316.
Louise H. Kidder, et al., Research Methods in Social Relations (New York: Holt Reinhart and Winston, 1986), chapter 12, pp. 299-311.
James M. Goldgeier, “Training Graduate Students in Conducting archival Research,” NewsNet (October 2004) [Describes GWU Cold War summer school program teaching students how to use Russian and U.S. archives in the study of foreign policy and IR]
Marc Trachtenberg, The Craft of International History: A Guide to Method (Princeton University Press, 2006).
Edward Ingram, “The Wonderland of the Political Scientist,” International Security , Vol. 22 (1997), pp. 53-63.
Michael R. Hill, Archival Strategies and Techniques (Newbury Park: Sage Publications, 1993), pp. 1-50.
Experimental and Quasi-Experimental Design
Albert D. Cover and Bruce S. Brumberg, “Baby Books and Ballots: The Impact of Congressional Mail n Constituent Opinion,” American Political Science Review , Vol. 76 (June 1982), pp. 347-359.
Rose McDermott, “Experimental Methods in Political Science,” Annual Review of Political Science , Vol. 5 (2002), pp. 31-61.
Macartan Humphreys and Jeremy Weinstein, “Field Experiments and the Political Economy of Development,” Annual Review of Political Science , Vol. 12 (2009), pp. 367-378.
Thad Dunning, “Improving Causal Inference: Strengths and Limitations of Natural Experiments,” Political Research Quarterly , Vol. 61 (2008), pp. 282-293.
Timothy N Cason and Vai-Lam Mui, “Testing Political Economy Models of Reform in the Laboratory,” American Economic Association, Papers and Proceedings , Vol. 93, No. 2 (May 2003), pp. 208-212.
Rose McDermott, Political Psychology in International Relations (Ann Arbor: University of Michigan Press, 2004).
Most-likely, Least-likely, and Deviant Cases
E. L. Morse, Foreign Policy and Interdependence in Gaullist France (Princeton University Press, 1973), chapter 5 on monetary policy. [least-likely case]
Jack S. Levy, “Case Studies: Types, Designs, and Logics of Inference. Conflict Management and Peace Science, Vol. 25, No. 1 (2008), pp. 1-18.
Harry Eckstein, “Case Studies and Theory in Political Science,” in Fred Greenstein and Nelson Polsby (eds.) Handbook of Political Science , Vol. 7 (Addison-Wesley, 1975), pp. 79-138.
William M. LeoGrande, “Cuban Dependency: A Comparison of Pre-Revolutionary and Post-Revolutionary International Economic Relations,” Cuban Studies , Vol. 9, No. 2 (July 1979), pp. 1-28. [most-likely case]
J. Berejekian, “The Gains Debate: Framing State Choice,” American Political Science Review , Vol. 91 (1997), pp. 789-805. [disciplined-configurative case study]
Alexander L. and Juliette L. George, Woodrow Wilson and Colonel House: A Personality Study (New York: John Day, 1956). [disciplined-configurative case study]
Richard Price, “A Genealogy of the Chemical Weapons Taboo,” International Organization , Vol. 49 (1995), pp. 73-103. [constructivist interpretation]
Arend Lijphart, The Politics of Accommodation: Pluralism and Democracy in the Netherlands (University of California Press, 1968). [deviant case study]
Bruce Russett, Grasping the Democratic Peace (Princeton University Press, 1993), chapter 3. [deviant case study]
Comparative Historical Analysis
Peter A. Hall, “Aligning Ontology and Methodology in Comparative Politics. In J. Mahoney & D. Rueschemeyer (Eds.), Comparative Historical Analysis in the Social Sciences (pp. 373-404). Cambridge, UK: Cambridge University Press, 2003).
James Mahoney, “Strategies of Causal Assessment in Comparative Historical Analysis,” in James Mahoney and Dietrich Rueschemeyer (eds) Comparative Historical Analysis in the Social Sciences (Cambridge University Press, 2003), chapter 10 (pp. 337-372).
Sven Steinmo, “Political Institutions and Tax Policy in the United States, Sweden, and Britain,” World Politics , Vol. 41, No. 4 (July 1989), pp. 500-535.
Theda Skocpol, “Doubly Engaged Social Science.” In Mahoney, James and Dietrich Rueschemeyer (eds): Comparative Historical Analysis in the Social Sciences (Cambridge University Press, 2003), pp. 407-428.
Theda Skocpol and Margaret Somers, “The Uses of Comparative History in Macrosocial Inquiry,” Comparative Studies in Society and History , Vol. 22, No. 2 (April 1980), pp. 174-197.
Theda Skocpol, States and Social Revolutions: A Comparative Analysis of France, Russia, and China (Cambridge: Cambridge University Press, 1979).
Barrington Moore, Jr., Social Origins of Dictatorship and Democracy: Lord and Peasant in the Making of the Modern World (Boston: Beacon Press, 1966).
Ruth Berins Collier and David Collier, Shaping the Political Arena: Critical Junctures, the Labor Movement, and Regime Dynamics in Latin America (Princeton University Press, 1991).
James Mahoney, “Long-Run Development and the Legacy of Colonialism in Spanish America,” American Journal of Sociology , Vol. 109, No. 1 (2003), pp. 51-106.
Alexander Hicks, Joya Misra, and Tang Nah Ng, “The Programmatic Emergence of the Social Security State,” American Sociological Review , Vol. 60, No. 3 (June 1995), pp. 329-349.
Jean Dreze and Amartya Sen, “China and India,” in Dreze and Sen (eds.) Hunger and Public Action (New York: Oxford University Press, 1989), chap. 11.
Daniel Ziblatt, “Rethinking the Origins of Federalism: Puzzle, Theory and Evidence from Nineteenth Century Europe,” World Politics (October 2004), pp. 70-98.
Gregory M. Luebbert, Liberalism, Fascism, or Social Democracy: Social Classes and the Political Origins of Regimes in Interwar Europe (New York: Oxford University Press, 1991).
Mixed Methods and Nested Analysis
Evan S. Lieberman, “Nested Analysis as a Mixed-Method Strategy for Comparative Research,” American Political Science Review , Vol. 99 (August 2005), pp. 435-452.
Todd D. Jick, “Mixing Quantitative and Qualitative Methods: Triangulation in Action,” Administrative Science Quarterly , Vol. 24, No. 4 (December 1979), pp. 602-611.
Jack Levy, “Qualitative Methods and Cross-Method Dialogue in Political Science ,” Comparative Political Studies , Vol. 40, No. 2 (February 2007), pp. 196-214.
Ingo Rohlfing, “What You See is What You Get: Pitfalls and Principles of Nested Analysis in Comparative Research,” Comparative Political Studies , Vol. 41, No. 11 (2008), pp. 1492-1514.
Michael Coppedge, “Thickening Thin Concepts and Theories: Combining Large N and Small in Comparative Politics,” Comparative Politics , Vol. 31, No. 4 (July 1999), pp. 465-476.
John Brewer and Albert Hunter, Foundations of Multimethod Research: Synthesizing Styles (Sage Publications, 2006).
Writing the Dissertation
Stephen Van Evera, Guide to Methodology for Students of Political Science (Cornell University Press, 1997), pp. 89-121.
Howard W. Becker, Writing for Social Scientists: How to Start and Finish your Thesis, Book or Article (University of Chicago Press, 1986).
“On Writing a Dissertation: Advice from Five Award Winners,” PS: Political Science and Politics (1986), pp. 61-70.
Patrick Dunleavy, Authoring a PhD Thesis: How to Plan, Draft, Write and Finish a Doctoral Dissertation (Palgrave Macmillan, 2003).
Monique Leijenaar and Emiliano Grossman, “Doing a PhD in Political Science in Europe: Information, Facts, Debate,” Paris: Thematic Network Political Science, 2009.
Michael Goldsmith (ed.), “Doctoral Studies in Political Science—A European Comparison,” Budapest: espNet, 2005.
Kate L. Turabian, A Manual for Writers of Research Papers, Theses, and Dissertations: Chicago Style for Students and Researchers (University of Chicago Press, 2007).
John M. Swales and Christine B. Feak, Academic Writing for Graduate Students: Essential Tasks and Skills (University of Michigan Press, 2004).
Jonathan P. Kastellec and Eduardo L. Leoni, “Using Graphs Instead of Tables in Political Science,” Perspectives on Politics , Vol. 5, No. 4 (2007), pp. 755-771.
Academic Writing and Publishing
William Strunk, Jr. and E. G. White, The Elements of Style , 2nd edition, (New York: Macmillan, 1972).
Rudolf Flesch, The Art of Readable Writing (New York: Collier, 1949).
Mary-Claire van Leunen, A Handbook for Scholars (New York: Oxford University Press, 1992).
William Germano, From Dissertation to Book (University of Chicago Press, 2005).
Teresa Pelton Johnson, “Writing for International Security —A Contributor’s Guide,” International Security , Vol. 16, No. 2 (September 1991), pp. 171-180.
Benjamin Frankel, “A Guide to Authors, for Contributors to Security Studies ,” Working Paper (November 2001).
Anne Lamont, “Shitty First Drafts,” in Bird by Bird: Some Instructions on Writing and Life (Anchor, 1995), pp. 21-27.
William Germano, Getting It Published: A Guide for Scholars and Anyone Else Serious about Serious Books (University of Chicago Press, 2001).
Kwan Choi, “How to Publish in Top Journals,” Manuscript posted at the website of Review of International Economics , http://www.roie.org/how.htm .
Gerald Schneider, Bernard Steunenberg, Katharina Holzinger, and Nils Petter Gleditsch, “Symposium: Why European Political Science is so Unproductive and What Should be Done About It,” European Political Science , Vol. 6, No. 2 (2007), pp. 156-191.
Paul J. Silvia, How to Write a Lot: A Practical Guide to Productive Academic Writing (Washington, DC: American Psychological Association, 2007).
Recommended Courses to Cover Before this One
Comparative Research Designs
Research Design Fundamentals
Recommended Courses to Cover After this One
Introduction to NVivo for Qualitative Data Analysis
Introduction to Qualitative Data Analysis with Atlas.ti
Causal Inference for Political and Social Sciences
Interpretive Interviewing
Field Research
Laggards go beyond catching up to become niche champions: a longitudinal case study in China
- Published: 11 April 2024
Cite this article
- Xinmin Peng 1 ,
- Abby Jingzi Zhou ORCID: orcid.org/0000-0002-1052-5842 2 ,
- Xiaomeng Liu 2 &
- Dianguang Liu 1
33 Accesses
Explore all metrics
Using a longitudinal case study on Cixing, which is a leading Chinese player in the flat knitting machine industry, this paper explores the process in which laggard firms catch up and exceed catching up to become niche champions in China. We propose a theoretical framework that illustrates the significance of contexts and response strategies for niche champions at different stages, focusing on the market and technology perspectives. In particular, the context is formed by the market ladder and technology modularization, requiring laggard firms to adopt appropriate market development and technology learning strategies in order to respond to the environment and achieve growth. During the catch-up stage, these companies should employ a market leveraging strategy and a technology deconstruction strategy to match the incumbents in the context of a pyramidal market ladder with low technology modularization. In the beyond-catch-up stage, as incumbents, they should adopt a market repositioning strategy and a technology reconstruction strategy to evolve into niche champions in the context of an upgraded market ladder with high technology modularization. Our research contributes to the literature on catch-up and niche champions by elucidating the process, contexts, and strategies of laggards in catching up and becoming niche champions in the global market. Practical insights are also offered to firms and policy makers in emerging economies.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
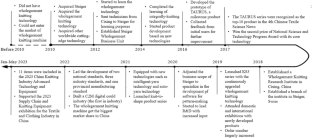
Data availability
The data used in this study are available upon request. Please contact the first author for access, subject to appropriate ethical and legal considerations.
The whole-garment technology represents a revolutionary approach of producing knitted wear as it can generate a complete garment in one piece without cutting or sewing. This technology involves a complex technical system that includes various scientific principles, engineering applications, and product development, requiring long-term accumulation.
https://www.ci-xing.com/news/300.html .
Abramovitz, M. (1986). Catching up, forging ahead, and falling behind. The Journal of Economic History, 46 (2), 385–406.
Article Google Scholar
Audretsch, D. B., & Lehmann, E. E. (2018). Internationalization strategies of hidden champions: Lessons from Germany. Multinational Business Review, 26 (1), 2–24.
Awate, S., Larsen, M. M., & Mudambi, R. (2012). EMNE catch-up strategies in the wind turbine industry: Is there a trade-off between output and innovation capabilities? EMNE Catch-Up strategies in the wind turbine industry. Global Strategy Journal, 2 (3), 205–223.
Awate, S., Larsen, M. M., & Mudambi, R. (2015). Accessing vs sourcing knowledge: A comparative study of R&D internationalization between emerging and advanced economy firms. Journal of International Business Studies, 46 (1), 63–86.
Baldwin, C. Y., & Clark, K. B. (2000). Design rules, volume 1: The Power of Modularity . MIT Press.
Binz, C., Gosens, J., Hansen, T., & Hansen, U. E. (2017). Toward Technology-sensitive catching-up policies: Insights from renewable energy in China. World Development, 96 , 418–437.
Brandt, L., & Thun, E. (2016). Constructing a ladder for growth: Policy, markets, and industrial upgrading in China. World Development, 80 (1), 78–95.
Bryman, A. (2016). Social research methods. Oxford university press.
Buckley, P. J., & Hashai, N. (2014). The role of technological catch up and domestic market growth in the genesis of emerging country based multinationals. Research Policy, 43 (2), 423–437.
Campagnolo, D., & Camuffo, A. (2010). The concept of modularity in management studies: A literature review. International Journal of Management Reviews, 12 (3), 259–283.
Cha, H., Wu, J., & Kotabe, M. (2021). The vulnerability problem of Business ecosystems under Global Decoupling. Management and Organization Review, 17 (3), 617–623.
China Textile Machinery Association (2023). Computerized flat knitting machine ushered in new opportunities for development (电脑针织横机迎来发展新机遇) Retrieved October 7, 2023, from https://www.ctma.net/contents/391/801.html
Chinese National Textile and Apparel Industrial Economics Research Institute (2018). China textile and garment industry operation report in the year 2017 (2017年中国纺织服装行业运行报告). Retrieved October 7, 2023, from http://lwzb.stats.gov.cn/pub/lwzb/gzdt/201804/t20180428_4871.html
Choi, S., Lee, J., & Park, H. W. (2020). A comparative study of sustainable transition from catch-up to post catch-up of South Korea and China. Sustainability, 12 (11), 4751.
Chung, M. Y., & Lee, K. (2015). How absorptive capacity is formed in a latecomer economy: different roles of foreign patent and know-how licensing in Korea. World Development, 66 , 678–694.
Cixing. (2023). Annual report . Retrieved October 9, 2023, from https://www.ci-xing.com/tzzgx.html
Cuervo-Cazurra, A. (2012). Extending theory by analyzing developing country multinational companies: Solving the Goldilocks debate. Global Strategy Journal, 2 (3), 153–167.
Cuervo-Cazurra, A., & Genc, M. (2008). Transforming disadvantages into advantages: Developing-country MNEs in the least developed countries. Journal of International Business Studies, 39 (6), 957–979.
Deng, Z., Ma, X., & Zhu, Z. (2022). Transactional dependence and technological upgrading in global value chains. Journal of Management Studies, 59 (2), 390–416.
Edmondson, A. C., & McManus, S. E. (2007). Methodological fit in management field research. Academy of Management Review, 32 (4), 1246–1264.
Eisenhardt, K. M. (1989). Building theories from case study research. The Academy of Management Review, 14 (4), 532–550.
Fixson, S. K., & Park, J. K. (2007). The power of integrality: linkages between product architecture, innovation, and industry structure. Research Policy, 37 (8), 1296–1316.
Frigant, V., & Talbot, D. (2005). Technological determinism and modularity: lessons from a comparison between aircraft and auto industries in Europe. Industry & Innovation, 12 (3), 337–355.
Gao, X. (2014). A latecomer’s strategy to promote a technology standard: the case of Datang and TD-SCDMA. Research Policy, 43 (3), 597–607.
Gao, R., & Sammartino, A. (2022). How does inward foreign direct investment shape emerging market firm invention patenting tendency? Evidence from China. Asia Pacific Journal of Management . https://doi.org/10.1007/s10490-022-09854-5 . online.
Gereffi, G., Humphrey, J., & Sturgeon, T. (2005). The governance of global value chains. Review of International Political Economy, 12 , 78–104.
Giachetti, C., & Marchi, G. (2017). Successive changes in leadership in the worldwide mobile phone industry: The role of windows of opportunity and firms’ competitive action. Research Policy, 46 (2), 352–364.
Gioia, D. A., Corley, K. G., & Hamilton, A. L. (2013). Seeking qualitative rigor in inductive research: Notes on the Gioia methodology. Organizational Research Methods, 16 (1), 15–31.
Glaser, B. G. (1965). The constant comparative method of qualitative analysis. Social Problems, 12 (4), 436–445.
Guennif, S., & Ramani, S. V. (2012). Explaining divergence in catching-up in pharma between India and Brazil using the NSI framework. Research Policy, 41 (2), 430–441.
Hakala, H. (2011). Strategic orientations in management literature: three approaches to understanding the interaction between market, technology, entrepreneurial and learning orientations: orientations in management literature. International Journal of Management Reviews, 13 (2), 199–217.
Hwang, H. R., & Choung, J. Y. (2014). The co-evolution of technology and institutions in the catch-up process: The case of the semiconductor industry in Korea and Taiwan. The Journal of Development Studies, 50 (9), 1240–1260.
Kang, H., & Song, J. (2016). Innovation and recurring shifts in industrial leadership: Three phases of change and persistence in the camera industry. Research Policy, 46 (2), 376–387.
Kiamehr, M., Hobday, M., & Hamedi, M. (2015). Latecomer firm strategies in complex product systems (CoPS): The case of Iran’s thermal electricity generation systems. Research Policy, 44 (6), 1240–1251.
Kotabe, M., Parente, R., & Murray, J. Y. (2007). Antecedents and outcomes of modular production in the Brazilian automobile industry: A grounded theory approach. Journal of International Business Studies, 38 (1), 84–106.
Langley, A. N. N., Smallman, C., Tsoukas, H., & Van de Ven, A. H. (2013). Process studies of change in organization and management: Unveiling temporality, activity, and flow. Academy of Management Journal, 56 (1), 1–13.
Lee, K., & Ki, J. H. (2017). Rise of latecomers and catch-up cycles in the world steel industry. Research Policy, 46 (2), 365–375.
Lee, K., & Lim, C. (2001). Technological regimes, catching-up and leapfrogging: Findings from the Korean industries. Research Policy, 30 (3), 459–483.
Lee, K., & Malerba, F. (2017). Catch-up cycles and changes in industrial leadership: Windows of opportunity and responses of firms and countries in the evolution of sectoral systems. Research Policy, 46 (2), 338–351.
Li, D., & Valentini, G. (2023). When are acquisitions a viable catch-up strategy? Some empirical evidence from China. Long Range Planning, 56 (1), 102265.
Li, D., Capone, G., & Malerba, F. (2019). The long march to catch-up: A history-friendly model of China’s mobile communications industry. Research Policy, 48 (3), 649–664.
Li, P. P., Prashantham, S., Zhou, A. J., & Zhou, S. S. (2022). Compositional springboarding and EMNE evolution. Journal of International Business Studies, 53 (4), 754–766.
Lopez-Vega, H., & Lakemond, N. (2021). Tapping into emerging markets: EMNEs’ strategies for innovation capability building. Global Strategy Journal, 12 (2), 394–417.
Luo, Y., & Tung, R. L. (2018). A general theory of springboard MNEs. Journal of International Business Studies, 49 (2), 129–152.
Magnusson, M., & Pasche, M. (2013). A contingency-based approach to the use of product platforms and modules in new product development. Journal of Product Innovation Management, 31 (3), 434–450.
Mahmood, I. P., & Singh, J. (2003). Technological dynamism in Asia. Research Policy, 32 (6), 1031–1054.
Mazzoleni, R., & Nelson, R. R. (2007). Public research institutions and economic catch-up. Research Policy, 36 (10), 1512–1528.
Miao, Y., Song, J., Lee, K., & Jin, C. (2018). Technological catch-up by east Asian firms: Trends, issues, and future research agenda. Asia Pacific Journal of Management, 35 (3), 639–669.
MIIT of China (Ministry of Industry and Information Technology of the People’s Republic of China) (2023). Notice of the General Office of the Ministry of Industry and Information Technology on Carrying out the Selection, Identification, Review and Evaluation of Niche Champion Enterprises in the Manufacturing Industry in 2023 ( 工业和信息化部办公厅关于开展2023年制造业单项冠军企业遴选认定和复核评价工作的通知 ). Retrieved October 7, 2023, from https://wap.miit.gov.cn/jgsj/zfs/qypy/art/2023/art_735d091e943449a4a34453b4426c939a.html
Park, K. H., & Lee, K. (2006). Linking the technological regime to the technological catch-up: Analyzing Korea and Taiwan using the US patent data. Industrial and Corporate Change, 15 (4), 715–753.
Parmigiani, A., Irwin, J., & Lahneman, B. (2022). Building greener motorhomes: How dual-purpose technical and relational capabilities affect component and full product innovation. Strategic Management Journal, 43 (6), 1110–1140.
Prencipe, A., Davies, A., & Hobday, M. (Eds.). (2003). The business of systems integration . Oxford University Press.
Prud’homme, D. (2016). Dynamics of China’s provincial-level specialization in strategic emerging industries. Research Policy, 45 (8), 1586–1603.
Qin, L., and Sun, S. L. (2022). Knowledge collaboration in global value chains: A comparison of supplier selection between a forerunner and a latecomer. Asia Pacific Journal of Management . https://doi.org/10.1007/s10490-022-09823-y . (online only)
Sanchez, R., & Mahoney, J. T. (2015). Modularity, flexibility, and knowledge management in product and organization design. Strategic Management Journal, 17 (S2), 63–76.
Scalera, V. G., Mukherjee, D., & Piscitello, L. (2020). Ownership strategies in knowledge-intensive cross-border acquisitions: Comparing Chinese and Indian MNEs. Asia Pacific Journal of Management, 37 (1), 155–185.
Schenkenhofer, J. (2022). Hidden champions: A review of the literature & future research avenues. Management Review Quarterly, 72 (2), 417–482.
Shepherd, D. A., Mcmullen, J. S., & Ocasio, W. (2017). Is that an opportunity? An attention model of top managers’ opportunity beliefs for strategic action. Strategic Management Journal, 38 (3), 5083–5094.
Simon, H. (1992). Lessons from Germany Midsize Giants. Harvard Business Review, 70 (2), 115–123.
Google Scholar
Simon, H. (2009). Hidden champions of the twenty-first century: Success strategies of unknown world market leaders . Springer.
Book Google Scholar
Song, M., Droge, C., Hanvanich, S., & Calantone, R. (2005). Marketing and technology resource complementarity: An analysis of their interaction effect in two environmental contexts. Strategic Management Journal, 26 (3), 259–276.
Sosa, M. E., Eppinger, S. D., & Rowles, C. M. (2004). The misalignment of product architecture and organizational structure in complex product development. Management Science, 50 (12), 1674–1689.
Swanborn, P. (2010). Case study research: What, why and how ? Sage Publications.
Venkateswaran, R. T. (2023). Is there an illusion of symmetry in cultural distance from Asia–pacific emnes? The role of business groups in navigating cultural distance through ambidextrous learning. Asia Pacific Journal of Management, 40 (3), 1169–1215.
Wei, J., Wang, D., & Liu, Y. (2018). Towards an asymmetry-based view of Chinese firms’ technological catch-up. Frontiers of Business Research in China, 12 (4), 12–20.
Witt, M. A., Lewin, A. Y., Li, P. P., & Gaur, A. (2023). Decoupling in international business: Evidence, drivers, impact, and implications for IB research. Journal of World Business, 58 (1), 101399.
Yang, M., & Ai, Q. (2023). Completion of high-tech MandAs by chinese firms: Knowledge distance, industry attractiveness and government involvement. Asia Pacific Journal of Management . (online) https://doi.org/10.1007/s10490-023-09923-3
Yin, R. K. (2009). Case study research: Design and methods (4th ed.). Sage.
Yu, X., Dosi, G., Grazzi, M., & Lei, J. (2017). Inside the virtuous circle between productivity, profitability, investment and corporate growth: An anatomy of Chinese industrialization. Research Policy, 46 (5), 1020–1038.
Download references
This study was financially supported by the National Natural Science Foundation of China (NSFC 72202111; 72172068; 71772097) and the Ministry of Education in China (22YJC630084).
Author information
Authors and affiliations.
Ningbo University, 818 Fenghua Road, Ningbo, Zhejiang, China
Xinmin Peng & Dianguang Liu
University of Nottingham Ningbo China, 199 Taikang East Road, Ningbo, Zhejiang, China
Abby Jingzi Zhou & Xiaomeng Liu
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Dianguang Liu .
Ethics declarations
Competing interests, additional information, publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Peng, X., Zhou, A.J., Liu, X. et al. Laggards go beyond catching up to become niche champions: a longitudinal case study in China. Asia Pac J Manag (2024). https://doi.org/10.1007/s10490-024-09961-5
Download citation
Accepted : 12 March 2024
Published : 11 April 2024
DOI : https://doi.org/10.1007/s10490-024-09961-5
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Niche champions
- Response strategies
- Find a journal
- Publish with us
- Track your research
- Open access
- Published: 11 April 2024
Glucose control during pregnancy in patients with type 1 diabetes correlates with fetal hemodynamics: a prospective longitudinal study
- Patrik Simjak 1 , 2 ,
- Katerina Anderlova 1 , 3 ,
- Dagmar Smetanová 2 ,
- Michal Kršek 3 ,
- Miloš Mráz 4 &
- Martin Haluzík 4
BMC Pregnancy and Childbirth volume 24 , Article number: 264 ( 2024 ) Cite this article
85 Accesses
1 Altmetric
Metrics details
Maternal diabetes adversely affects fetal cardiovascular system development. Previous studies have reported that the fetuses of mothers with diabetes exhibit both structural and functional changes; nevertheless, prior studies have not examined the association between glucose control and fetal cardiac morphology and performance. Thus, the objective was to determine the association between fetal cardiac morphology and function and maternal glucose control in type 1 diabetes and to compare the differences in measured cardiac parameters between the fetuses of mothers with diabetes and healthy controls.
In this prospective, longitudinal case-control study — including 62 pregnant women with type 1 diabetes mellitus and 30 healthy pregnant women — fetal cardiac assessment using B-mode, M-mode, and spectral pulsed-wave Doppler was performed in the second and third trimesters. In women with T1DM, glycated hemoglobin and data obtained from glucose sensors — including the percentage of time in, below, and above the range (TIR, TBR, and TAR, respectively), and coefficient of variation (CV) — were analyzed across three time periods: the last menstrual period to 13 (V1), 14–22 (V2), and 23–32 weeks (V3) of gestation. Fetal cardiac indices were compared between groups, and the correlation between glucose control and fetal cardiac indices was assessed.
At 28–32 weeks, the fetuses of women with T1DM exhibited increased left ventricular end-diastolic length, relative interventricular septum thickness, right ventricular cardiac output, and pulmonary valve peak systolic velocity compared with healthy controls. At 18–22 weeks, pulmonary and aortic valve diameters, left and right ventricular stroke volumes, and left cardiac output inversely correlated with the CV and glycated hemoglobin levels at V1 and V2. Furthermore, at 28–32 weeks, pulmonary and aortic valve diameters, left ventricular stroke volume, cardiac output, and right/left atrioventricular valve ratio inversely correlated with the TBR at V1, V2, and V3. Moreover, diastolic functional parameters correlated with the TAR and glycated hemoglobin levels, particularly after the first trimester.
In women with T1DM, maternal hyperglycemia during pregnancy correlates with fetal diastolic function, whereas glucose variability and hypoglycemia inversely correlate with fetal left ventricular systolic function in the second and third trimesters.
Key message
This prospective longitudinal study demonstrates that in women with T1DM, maternal hyperglycemia during pregnancy correlates with fetal diastolic function. In contrast, glucose variability and hypoglycemia inversely correlate with fetal left ventricular systolic function in the second and third trimesters.
Peer Review reports
Type 1 diabetes mellitus (T1DM) is a chronic metabolic disease caused by absolute insulin deficiency due to the autoimmune destruction of pancreatic B-cells. Usually diagnosed in childhood or early adulthood, T1DM inevitably affects reproduction. The reported prevalence of T1DM in pregnancy is 4.1–4.7 per 1000 pregnancies [ 1 , 2 ]. Maternal diabetes adversely affects fetal development in various ways, such as by significantly affecting the fetal cardiovascular system. Previous studies have reported that the fetuses of mothers with diabetes have more globular hearts, increased right and left sphericity indices, and subclinical systolic dysfunction in the second half of pregnancy [ 3 , 4 ]; fetal hyperinsulinemia owing to enhanced maternal-fetal glucose transport is thought to be the underlying cause. Nevertheless, prior studies have not examined the association between glucose control, and fetal cardiovascular morphology and performance. Additionally, T1DM and gestational diabetes (GDM) were often combined, regardless of the differences in etiopathogenesis and clinical presentation.
Glucose sensors have been used in the care of pregnant women with T1DM for several years. This creates an opportunity for the noninvasive, instant monitoring of glycemia at any time during the day, thereby enabling early treatment decisions. These wearables perform real-time continuous glucose monitoring (CGM) to alert the user when preset glucose targets are exceeded or flash glucose monitoring (FGM) that indicates glycemia when a reader is applied to the sensor. While recent studies have confirmed the safety and accuracy of both methods during pregnancy [ 5 , 6 ], CGM is associated with improved neonatal outcomes, presumably due to better diabetes compensation [ 7 ].
The adoption of glucose sensors allowed for the development of core metrics for understanding glycemic status — including the time in, below, and above the range (TIR, TBR, and TAR, respectively) — and the coefficient of variation (CV), which describe the effectiveness of treatment in more detail than the traditionally used glycated hemoglobin (A1c). Notably, the high sensitivity of the sensors also enables the detection of glycemic fluctuations in pregnant women with a negative oral glucose tolerance test [ 8 ]. Thus, these sensors provide an entirely new opportunity to study the relationship between diabetes compensation and the development of pregnancy-related complications.
The primary objective of this prospective study was to determine the association between fetal cardiac morphology and function and maternal glucose control in T1DM. Secondarily, we aimed to compare the differences in measured cardiac parameters between the fetuses of mothers with T1DM and healthy controls.
Subjects and methods
Study population.
This prospective, longitudinal case-control study included 64 consecutively recruited pregnant women with T1DM, and 32 matched healthy pregnant women. Pregnant women attending the combined first-trimester screening between April 2018 and December 2022 were recruited. The general exclusion criteria were multiple pregnancies, and fetal structural or chromosomal abnormalities diagnosed during the pregnancy. Women assigned to the control group had a standard 75 g oral glucose tolerance test performed between 24 and 28 weeks of gestation. Two women met the American Diabetes Association (ADA) criteria for diagnosis of GDM and were excluded from the analysis. All participants provided written informed consent for all study procedures, and the study protocol was approved by the Human Ethics Review Board.
Information on the maternal body mass index (BMI), age, race, method of conception (natural or assisted by in-vitro fertilization), cigarette smoking during pregnancy, and parity were recorded at the first visit. In women with T1DM, the disease duration (in completed years) was calculated, and diabetes-related morbidity, sensor type, and treatment modalities were recorded.
In all women with T1DM, glucose monitoring was initiated either before pregnancy or during the first trimester; a FGM system (FreeStyle® Libre™; Abbott, Inc.) or glucose sensors (G6®; DexCom, Inc., San Diego, CA, USA; or Guardian™ 4; Medtronic, Inc., Minneapolis, MN, USA) for real-time CGM of the interstitial fluid were used. Women with diabetes were followed-up every 4 weeks; if necessary, the diabetologist adjusted the treatment to ensure optimal disease control. The data obtained from sensors — including the TIR (time spent in target [3.5–7.8 mmol/l]), TBR (time spent below target [< 3.5 mmol/l]), TAR (time spent above target [> 7.8 mmol/l]) percentages — A1c, and CV were analyzed across three time periods: the last menstrual period to 13 weeks (V1); 14–22 weeks (V2); and 23–32 weeks (V3) of gestation. Insulin was administered via an insulin pump or multiple daily injections.
Standard perinatal outcomes were recorded after delivery, including gestational age, mode of delivery, birthweight, the incidence of preeclampsia, neonatal hypoglycemia, congenital malformations, NICU admission and umbilical artery pH.
Echocardiography and ultrasound assessment
In all women, fetal B-mode, M-mode, and spectral pulsed-wave (PW) Doppler examinations were performed in the second and early third trimesters (18–22 weeks and 28–32 weeks of gestation, respectively) as a part of the routine prenatal ultrasound examinations. One investigator (P.S.) performed all fetal ultrasound examinations using a VolusonTM E10 BT 18 ultrasound system (GE Healthcare, Chicago, Il, USA). All measurements were performed using a convex-array obstetric transducer (C2-9). M-mode was used to assess ventricular free and septal wall thicknesses, and chamber dimensions. An apical, basal, or lateral four-chamber view in B-mode was used to obtain measurements regarding the cardiac axis, cardiothoracic index, ventricular length, and ventricular and semilunar valve dimensions, as appropriate. The ventricular sphericity index was calculated as the ventricular end-diastolic diameter/end-diastolic length. The relative wall thicknesses of the ventricles and interventricular septum (IVS) were estimated as (2 × free wall or septal wall thickness)/ventricular end-diastolic diameter. PW Doppler with an angle correction of < 45° was used to obtain Doppler signals from the inflow and outflow tracts for the evaluation of diastolic and systolic function. The left ventricular (LV) myocardial performance index (MPI) was obtained from a single cardiac cycle by placing the sample volume at the junction of the anterior mitral valve leaflet and left outflow tract to simultaneously display ventricular filling and emptying. For the right ventricular (RV) MPI, inflow and outflow pulsed Doppler signals were obtained separately, and MPI was only calculated if the difference between the fetal heart rate in the inflow and outflow tracts was < 5 beats per minute. Fetal biometry was performed in all women, and the pulsatility indices of the uterine and umbilical arteries were assessed.
Intra- and interobserver reproducibility
The same investigator (P.S.) repeated the measurements on 20 randomly selected fetal echocardiograms obtained in the second and third trimesters in the same cardiac cycle. A second observer (D.S.) repeated the measurements using the same echocardiogram. Intraclass correlation coefficients (ICCs) were calculated to assess intra- and interobserver variability.
Statistical analysis
Sample size and power calculations were performed based on the assumption that in the second trimester, the mean septal thickness increases by 10% in the fetuses of women with poorly controlled diabetes compared with controls [ 9 ]. Assuming a standard deviation of 10%, with an alpha of 0.05 and a power of 85%, the required sample size should be 39 with an enrollment ratio of 2:1. The enrollment ratio in favor of women with T1DM was chosen with the primary outcome of the study in mind and accounted for the lower propensity of healthy pregnant women to comply with the study protocol.
The Shapiro-Wilk test was performed to assess the data distribution for normality. Normally distributed continuous variables were presented as mean ± SD, and nonnormally distributed variables as median (interquartile range). Nominal variables were presented as numbers (percentages). Maternal and fetal parameters were compared between groups using the independent-samples Student’s t -test or Mann-Whitney U-test for continuous variables, and Chi-squared test for categorical variables. The Friedman test was used to detect differences in diabetes compensation across the three time periods. Pearson’s correlation test was used to assess the relationship between diabetes compensation and fetal cardiac indices.
Pregnancy characteristics and diabetes control
In total, 94 pregnant women consented to participate in the study, including 64 with T1DM and 32 healthy controls; two women from the T1DM group were excluded from the analysis due to fetal anomalies (common arterial trunk and caudal regression syndrome); two women in the healthy control group met the American Diabetes Association (ADA) criteria for diagnosis of GDM and were excluded. No significant differences in the baseline population characteristics were observed between the groups, excluding a higher BMI in women with T1DM. As expected, birthweight was higher, and cesarean section, preeclampsia, and neonatal hypoglycemia were more frequent in the T1DM group.
The demographic characteristics and perinatal outcomes of the enrolled women are summarized in Table 1 . Of the 62 women with T1DM, 52 started using glucose sensors before conception, whereas the remaining started in the first trimester. CGM and FGM were performed in 44 and 18 women, respectively. Insulin was administered via insulin pump to 33 (53.2%) women, whereas 29 (46.8%) received multiple daily injections. Characteristics of women with type 1 diabetes mellitus are summarized in Table 2 . In women with T1DM, the mean A1c levels gradually decreased from preconception to V2, and then increased at V3. The same pattern was observed in the control group, but A1c was significantly lower in all visits. As expected, in women T1DM, A1c correlated with the TAR and CV during pregnancy. By contrast, A1c inversely correlated with the TIR. Furthermore, an inverse correlation was observed between the TBR at V1 (Table S1 ). Compared with the first trimester, women spent more TIR and less TAR at subsequent intervals. The glucose control of women in both study groups is summarized in Table 3 . The ADA criterion for good glucose control, a TIR > 70%, was achieved in 41% of women with diabetes at all follow-up periods.
Cardiac geometry and function
The groups were comparable regarding the estimated fetal weight and pulsatility indices in the umbilical and uterine arteries. No differences in fetal cardiac geometry and function were observed between the groups at 18–22 weeks. At 28–32 weeks, the fetuses of women with T1DM exhibited increased LV end-diastolic length, relative IVS thickness, RV cardiac output (RV-CO), and pulmonary valve peak systolic velocity compared with the fetuses of healthy controls. A summary of the cardiac parameters in women with T1DM and controls in the second and third trimesters is presented in Table 4 . The ICCs indicated moderate to excellent (ICC: 0.60–0.99) intra- and interobserver reliabilities (Table S2 ).
An inverse correlation between the CV and echocardiographic parameters was observed between 18 and 22 weeks. Specifically, pulmonary valve diameter and RV stroke volume (RV-SV) decreased with increasing CV prior to 14 weeks ( r = − 0.51, P = 0.001; r = − 0.35, P = 0.033; respectively). Additionally, the CVs at V1 and V2 inversely correlated with the LV-SV ( r = − 0.33, P = 0.043; r = − 0.41, P = 0.008; respectively), and aortic valve (AV) diameter and LV-CO at V2 ( r = − 0.31, P = 0.046; r = − 0.39, P = 0.011; respectively). An inverse correlation was also observed between A1c and AV diameter at V1 ( r = − 0.32, P = 0.018), and LV-SV and LV-CO at V1 and V2 ( r = − 0.37, P = 0.006; r = − 0.27, P = 0.042; r = − 0.31, P = 0.024; r − 0.27, P = 0.041; respectively). Thus, increased glycemic variability and A1c in the first half of pregnancy impaired mid-gestation ventricular systolic function, and decreased semilunar valve diameters contributing to decreased SVs.
At 28–32 weeks, the AV diameter inversely correlated with the TBR at V1, V2, and V3 ( r = − 0.38, P = 0.006; r = − 0.35, P = 0.008; r = − 0.37, P = 0.005; respectively), but positively correlated with A1c at V3 ( r = 0.30; P = 0.025). The TBR also inversely correlated with LV systolic function, represented by LV-SV ( r = − 0.33, P = 0.029; r = − 0.32, P = 0.017; r = − 0.29, P = 0.024; for V1, V2, V3 respectively) and LV-CO ( r = − 0.35, P = 0.023; r = − 0.34, P = 0.011; r = − 0.29, P = 0.029; for V1, V2, V3 respectively; Fig. 1 ). Moreover, LV-SV correlated with A1c at V3 ( r = 0.27; P = 0.047).

Scatterplots demonstrating the negative correlation between left ventricular cardiac output (LV-CO) and time below range (TBR) in the first 14 weeks (V1; r = -0.35, P = 0.023), at 14–22 weeks (V2; r = -0.34, P = 0.011), and at 23–28 weeks (V3; r = -0.29, P = 0.029) of gestation
By contrast, diastolic function markers correlated with A1c and TAR. At 28–32 weeks, the TAR correlated with RV A ( r = 0.29, P = 0.009; r = 0.32, P = 0.017; r = 0.29, P = 0.047; for V1, V2, V3 respectively), LV E ( r = 0.30, P = 0.034; r = 0.36, P = 0.008; for V2, V3 respectively), and LV A ( r = 0.29, P = 0.031 for V3). Similarly, A1c correlated with RV E ( r = 0.33, P = 0.014; r = 0.32, P = 0.020; for V2, V3 respectively), RV A ( r = 0.30, P = 0.007; r = 0.36, P = 0.006; for V2, V3 respectively), and LV E ( r = 0.28; P = 0.036; for V3). The correlations between glucose control and fetal cardiac geometry and function are summarized in Table 5 .
This study presents a detailed analysis of fetal cardiovascular hemodynamics during the second and early third trimesters of patients with T1DM in relation to glucose control, and a comparison with healthy controls. The results demonstrate that in the study population, where 41% of women achieved the recommended glucose control target (> 70% of the TIR) throughout pregnancy, significant changes in cardiac geometry and function were only observed in the early third trimester. Additionally, this study demonstrates for the first time that glucose variability and maternal hypoglycemia affect LV performance in the second and third trimesters. By contrast, hyperglycemia during pregnancy affects the fetal diastolic function. Thus, optimal control of T1DM enhances fetal hemodynamics. However, the extent to which improvements in fetal hemodynamics can translate into improved clinical outcomes remains to be elucidated.
Although the pathophysiology of impaired fetal cardiac development in maternal diabetes is complex and incompletely understood, increased transplacental glucose transport and subsequent fetal hyperinsulinemia are thought to be the main causes [ 10 ]. Fetal hyperinsulinemia can alter placental mRNA expression, leading to the dysregulation of insulin/insulin-like growth factor (IGF) systems [ 11 ]. IGF-1 is a potent stimulator of cell growth, and experimental studies have demonstrated that it promotes prenatal cardiomyocyte growth [ 12 ]. Additionally, a positive correlation between cord blood IGF-1 bioavailability and IVS thickness was observed in the newborns of mothers with diabetes [ 13 ]. Other major factors that influence fetal heart morphology and function include increased oxidative stress, subclinical low-grade inflammation, maternal obesity, triglyceridemia, and placental dysfunction [ 13 , 14 , 15 ].
Similar to previously published studies, we demonstrated distinct changes in fetal cardiac morphology in the fetuses of mothers with T1DM during the third trimester, compared with controls. These included increased heart area, greater LV-EDL, and a thicker IVS [ 16 ]. Other studies have reported a more globular heart shape with increased ventricular sphericity indices [ 4 , 17 ]; however, the cohorts in these studies mainly comprised women with gestational diabetes and fetal echocardiography was performed later in the third trimester, potentially explaining the noted discrepancies. A recent meta-analysis confirmed IVS thickening in the fetuses of women with T1DM; however, increased septal thickness has also been observed in the second trimester [ 16 ].
Previous research on pregnant women with diabetes has also revealed impaired fetal cardiac function, which can be demonstrated using various ultrasound examination techniques at different stages of pregnancy. The very first detectable manifestation of fetal heart function is the heart rate. One study found that pregnant women with pregestational diabetes (type 1 and 2) had a higher fetal heart rate in the first trimester compared to healthy women, regardless of their BMI [ 18 ]. However, our study found that the fetal heart rate was similar in both groups during the later trimesters.
Another parameter, fetal MPI, has been assessed by two recent meta-analyses concerning diabetes in pregnancy [ 16 , 19 ]. In the study by Depla et al., fetal MPI in women with pregestational diabetes and controls were comparable, but Sirico et al. observed higher MPI in fetuses of diabetic mothers in the third trimester. Although both were published in a similar time period, each had different study inclusion criteria, which affected the results. Nevertheless, the MPI may be confounded by coexisting complications that are common in women with diabetes, such as maternal obesity, fetal macrosomia, or placental function. We did not observe differences in left or right ventricular MPI between the groups, possibly due to the comparable estimated fetal weight and uteroplacental Doppler indices between the groups or the limited number of study participants. Nevertheless, fetal MPI was unrelated to glucose control in our cohort.
Furthermore, we failed to demonstrate impaired diastolic function in the second and early third trimesters using spectral PW Doppler, which is consistent with the results of another published study [ 20 ]. However, a lower diastolic strain rate was observed in this study, suggesting that speckle-tracking echocardiography is a more sensitive method for assessing fetal heart dysfunction [ 20 ]. These subtle subclinical changes likely precede diastolic dysfunction, as demonstrated using conventional ultrasound parameters during the third trimester [ 21 ]. A similar impairment of diastolic function was also observed in the fetuses of mothers with gestational diabetes [ 22 ]; thus, hyperglycemia-induced cardiac remodeling and the consequent fetal adaptation may be responsible for this phenomenon. Indeed, we observed a positive correlation between the percentage of time spent in hyperglycemia, A1c, and diastolic function, mainly regarding the RV A wave. In line with our findings, a lower right E/A ratio was observed in the fetuses of women with poorly controlled pregestational diabetes [ 20 , 23 ].
Regarding fetal systolic function in pregnancies complicated by T1DM, the evidence is inconclusive. A higher RV-SV was observed; however, the difference in CO was not significant after correcting for estimated fetal weight. A similar finding was observed at the end of the third trimester in a mixed cohort including the fetuses of mothers with GDM and T1DM [ 4 ]. In another study, RV systolic impairment was demonstrated using speckle-tracking echocardiography [ 24 ]. Although a difference in the LV-CO was not observed in the second and early third trimesters in the fetuses of women with T1DM, another study demonstrated a significant decrease in LV-CO at term [ 4 ]. In these fetuses, LV-CO was restored to values comparable to those in the healthy population early after birth, suggesting a suppressive effect of diabetes on heart function. A novel finding of our study was that LV-CO inversely correlated with glucose variability and A1c in the second trimester, and the percentage of time spent in hypoglycemia in the third trimester, independent of fetal weight.
As CO is dependent on the diameter of the corresponding semilunar valve and fetal heart rate an inverse correlation between the TBR and AV diameter contributed to this finding. Notably, up to 40% of women experience severe hypoglycemia during pregnancy [ 25 ]. Our finding that hypoglycemia impairs heart function is also supported by an earlier study that reported decreased fetal heart rate variability during maternal hypoglycemia episodes [ 26 ]. Nevertheless, maintaining a sufficient fetal CO is crucial to ensure adequate perfusion of the placenta, especially when fetal oxygen requirements peak in the late third trimester. Furthermore, women with T1DM exhibit increased placental angiogenesis, leading to a larger distribution volume and thus, a decreased afterload [ 27 ]. Strict compensation for diabetes with frequent episodes of hypoglycemia can lead to chronic hypoxia that may not manifest as overt fetal growth restriction, as the fetuses of pregnant women with diabetes are often predisposed to being macrosomic. We hypothesized that in most susceptible fetuses with diabetic fetopathy, this may even result in sudden intrauterine fetal demise in women with seemingly good compensation. Thus, with respect to strict glycemic control in pregnant women with T1DM, caution is necessary to prevent potentially harmful episodes of maternal hypoglycemia, especially in the third trimester.
This is the first prospective longitudinal study to evaluate the association between fetal cardiac geometry and function and glucose control in a cohort of women with T1DM. It highlights the importance of optimal glucose control in women with T1DM during pregnancy, as maternal hyperglycemia during pregnancy correlates with fetal diastolic function, whereas glucose variability and hypoglycemia inversely correlate with fetal left ventricular systolic function in the second and third trimesters.
The main strength of this study was the prospective monitoring of glucose control using glucose sensors, and ultrasound evaluation of fetal cardiac function by a multidisciplinary team of specialists in diabetology and fetal medicine. Another strength was the consecutive recruitment of women with diabetes to minimize selection bias. During the study period, the estimated weight and routine Doppler indices of fetuses of women with diabetes did not differ from those of healthy controls; thus, we believe that these variables had negligible confounding effects on the presented results.
The main limitation of the present study was that the sample size was too small to allow for adjustment for potential confounders. The reason for the inclusion of fewer healthy controls was the lower willingness of women to comply with the study protocol, which required all ultrasound examinations and delivery at the investigating centre. Recruitment of healthy controls was also undermined by anti-epidemic measures during the SARS-CoV 19 pandemic.
The ultrasound examinations were performed by a single examiner who was not blinded to the diagnosis of diabetes, which implies the possibility of bias. Therefore, the measurements were repeated by the second blinded observer resulting in moderate to excellent interobserver agreements.
Data availability
The raw data can be obtained on request from the corresponding author.
Abbreviations
Glycated hemoglobin
Atrial contraction peak velocity
Aortic valve
Cardiac output
Coefficient of variation
Early diastolic peak velocity
End-diastolic diameter
End-diastolic length
Estimated fetal weight
Interventricular septum
Left atrioventricular valve
Left ventricle
Myocardial performance index
Pulsatility index
Pulmonary valve
Right atrioventricular valve
Right ventricle
Stroke volume
Type 1 diabetes
Time above range
Time below range
Time in range
Fadl HE, Simmons D. Trends in diabetes in pregnancy in Sweden 1998–2012. BMJ Open Diabetes Res Care. 2016;4:e000221. https://doi.org/10.1136/bmjdrc-2016-000221
Article PubMed PubMed Central Google Scholar
Coton SJ, Nazareth I, Petersen I. A cohort study of trends in the prevalence of pregestational diabetes in pregnancy recorded in UK general practice between 1995 and 2012. BMJ Open. 2016;6:e009494. https://doi.org/10.1136/bmjopen-2015-009494
Yovera L, Zaharia M, Jachymski T, Velicu-Scraba O, Coronel C, de Paco Matallana C, et al. Impact of gestational diabetes mellitus on fetal cardiac morphology and function: Cohort comparison of second- and third-trimester fetuses. Ultrasound Obstet Gynecol. 2021;57:607–13. https://doi.org/10.1002/uog.22148
Article CAS PubMed Google Scholar
Patey O, Carvalho JS, Thilaganathan B. Perinatal changes in fetal cardiac geometry and function in diabetic pregnancy at term. Ultrasound Obstet Gynecol. 2019;54:634–42. https://doi.org/10.1002/uog.20187
Castorino K, Polsky S, O’malley G, Levister C, Nelson K, Farfan C, et al. Performance of the Dexcom G6 continuous glucose monitoring system in pregnant women with diabetes. Diabetes Technol Ther. 2020;22:943–7. https://doi.org/10.1089/dia.2020.0085
Article CAS PubMed PubMed Central Google Scholar
Scott EM, Bilous RW, Kautzky-Willer A. Accuracy, user acceptability, and safety evaluation for the FreeStyle Libre Flash glucose monitoring system when used by pregnant women with diabetes. Diabetes Technol Ther. 2018;20:180–8. https://doi.org/10.1089/dia.2017.0386
Feig DS, Donovan LE, Corcoy R, Murphy KE, Amiel SA, Hunt KF, et al. Continuous glucose monitoring in pregnant women with type 1 diabetes (CONCEPTT): a multicentre international randomised controlled trial. Lancet. 2017;390:2347–59. https://doi.org/10.1016/S0140-6736(17)32400-5
Tartaglione L, di Stasio E, Sirico A, Di Leo M, Caputo S, Rizzi A, et al. Continuous glucose monitoring in women with normal OGTT in pregnancy. J Diabetes Res. 2021;2021:9987646. https://doi.org/10.1155/2021/9987646
Atiq M, Ikram A, Hussain BM, Saleem B. Assessment of cardiac function in fetuses of gestational diabetic mothers during the second trimester. Pediatr Cardiol. 2017;38:941–5. https://doi.org/10.1007/s00246-017-1600-2
Article PubMed Google Scholar
Pauliks LB. The effect of pregestational diabetes on fetal heart function. Expert Rev Cardiovasc Ther. 2015;13:67–74. https://doi.org/10.1586/14779072.2015.988141
Tumminia A, Scalisi NM, Milluzzo A, Ettore G, Vigneri R, Sciacca L. Maternal diabetes impairs insulin and IGF-1 receptor expression and signaling in human placenta. Front Endocrinol (Lausanne). 2021;12:621680. https://doi.org/10.3389/fendo.2021.621680
Jonker SS, Louey S. Endocrine and other physiologic modulators of perinatal cardiomyocyte endowment. J Endocrinol. 2016;228:R1–18. https://doi.org/10.1530/JOE-15-0309
El-Ganzoury MM, El-Masry SA, El-Farrash RA, Anwar M, Abd Ellatife RZ. Infants of diabetic mothers: echocardiographic measurements and cord blood IGF-I and IGFBP-1. Pediatr Diabetes. 2012;13:189–96. https://doi.org/10.1111/j.1399-5448.2011.00811.x
Al-Biltagi M, Razaky O, El, Amrousy D, El. Cardiac changes in infants of diabetic mothers. World J Diabetes. 2021;12:1233–47. https://doi.org/10.4239/wjd.v12.i8.1233
Pisaneschi S, Boldrini A, Genazzani AR, Coceani F, Simoncini T. Feto-placental vascular dysfunction as a prenatal determinant of adult cardiovascular disease. Intern Emerg Med. 2013;8:S41–5. https://doi.org/10.1007/s11739-013-0925-y
Depla AL, De Wit L, Steenhuis TJ, Slieker MG, Voormolen DN, Scheffer PG, et al. Effect of maternal diabetes on fetal heart function on echocardiography: systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2021;57:539–50. https://doi.org/10.1002/uog.22163
Aguilera J, Semmler J, Coronel C, Georgiopoulos G, Simpson J, Nicolaides KH, et al. Paired maternal and fetal cardiac functional measurements in women with gestational diabetes mellitus at 35–36 weeks’ gestation. Am J Obstet Gynecol. 2020;223:e5741–57415. https://doi.org/10.1016/j.ajog.2020.04.019
Article Google Scholar
Sirico A, Sarno L, Zullo F, Martinelli P, Maruotti GM. Pregestational diabetes and fetal heart rate in the first trimester of pregnancy. Eur J Obstet Gynecol Reprod Biol. 2019;232:30–2. https://doi.org/10.1016/j.ejogrb.2018.11.003
Sirico A, Raffone A, Maruotti GM, Travaglino A, Paciullo C, Diterlizzi A, et al. Third trimester myocardial performance index in fetuses from women with hyperglycemia in pregnancy: a systematic review and Meta-analysis. Ultraschall Med. 2023;44(2):e99–107. https://doi.org/10.1055/a-1499-7265
Miranda JO, Cerqueira RJ, Ramalho C, Areias JC, Henriques-Coelho T. Fetal cardiac function in maternal diabetes: a conventional and speckle-tracking echocardiographic study. J Am Soc Echocardiogr. 2018;31:333–41. https://doi.org/10.1016/j.echo.2017.11.007
Fouda UM, Abou Elkassem MM, Hefny SM, Fouda RM, Hashem AT. Role of fetal echocardiography in the evaluation of structure and function of fetal heart in diabetic pregnancies. J Matern Fetal Neonatal Med. 2012;26:571–5. https://doi.org/10.3109/14767058.2012.743521
Hou Q, Yan F, Dong X, Liu H, Wu J, Li J, et al. Assessment of fetal cardiac diastolic function of gestational diabetes mellitus using dual-gate doppler. Med (Baltim). 2021;100:e26645. https://doi.org/10.1097/MD.0000000000026645
Article CAS Google Scholar
Menekse Beser D, Oluklu D, Uyan Hendem D, Yildirim M, Turgut E, Sahin D. Effect of glycemic control on fetal hearts of pregestational diabetic women by tissue doppler and M-mode imaging. Echocardiography. 2023;40:822–30. https://doi.org/10.1111/echo.15649
Wong SF, Chan FY, Cincotta RB, McIntyre HD, Oats JJN. Cardiac function in fetuses of poorly-controlled pre-gestational diabetic pregnancies – a pilot study. Gynecol Obstet Invest. 2003;56:113–6. https://doi.org/10.1159/000073191
Rosenn BM, Miodovnik M. Glycemic control in the diabetic pregnancy: is tighter always better? J Matern Fetal Med. 2000;9:26–34. https://doi.org/10.1002/(SICI)1520-6661(200001/02)9:1%3C29::AID-MFM7%3E3.0.CO;2-Z
Stangenberg M, Persson B, Stånge L, Carlström K. Insulin-induced hypoglycemia in pregnant diabetics. Acta Obstet Gynecol Scand. 1983;62:249–52. https://doi.org/10.3109/00016348309155801
Evers IM, Nikkels PGJ, Sikkema JM, Visser GHA. Placental pathology in women with type 1 diabetes and in a control group with normal and large-for-gestational-age infants. Placenta. 2003;24:819–25. https://doi.org/10.1016/s0143-4004(03)00128-0
Download references
Acknowledgements
Not applicable.
Funding for this work was provided by the Czech Health Research Council (NU20-01-00067) and the National Institute for Research of Metabolic and Cardiovascular Diseases (Programme EXCELES, ID Project No. LX22NPO5104), funded by the European Union – Next Generation EU.
Author information
Authors and affiliations.
Clinic of Gynecology, Obstetrics and Neonatology, First Faculty of Medicine, Charles University and General University Hospital, Prague, Czech Republic
Patrik Simjak & Katerina Anderlova
Gennet s.r.o, Fetal Medicine Center, Prague, Czech Republic
Patrik Simjak & Dagmar Smetanová
3rd Internal Clinic, First Faculty of Medicine, Charles University and General University Hospital, Prague, Czech Republic
Katerina Anderlova & Michal Kršek
Diabetes Centre, Institute for Clinical and Experimental Medicine, Prague, Czech Republic
Miloš Mráz & Martin Haluzík
You can also search for this author in PubMed Google Scholar
Contributions
M.H. and K.A. designed the study; K.A., P.S., D.S., M.M. collected the data; M.M. and M.K. analyzed the data and interpreted the results; P.S. drafted the manuscript. All authors reviewed the results and approved the manuscript.
Corresponding author
Correspondence to Katerina Anderlova .
Ethics declarations
Ethics approval and consent to participate.
The study was conducted in the accordance with the Declaration of Helsinki. The study protocol was approved by the Human Ethics Review Board of the First Faculty of Medicine and General University Hospital, Prague, Czech Republic (Reference: 24/19 Grant AZV VES 2020 VFN). Informed consent was obtained from all individuals included in this study.
Consent for publication
Competing interests.
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Simjak, P., Anderlova, K., Smetanová, D. et al. Glucose control during pregnancy in patients with type 1 diabetes correlates with fetal hemodynamics: a prospective longitudinal study. BMC Pregnancy Childbirth 24 , 264 (2024). https://doi.org/10.1186/s12884-024-06462-7
Download citation
Received : 19 November 2023
Accepted : 28 March 2024
Published : 11 April 2024
DOI : https://doi.org/10.1186/s12884-024-06462-7
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Fetal hemodynamics
- Glucose control
- Echocardiography
- Hypoglycemia
- Hyperglycemia
BMC Pregnancy and Childbirth
ISSN: 1471-2393
- Submission enquiries: [email protected]
- General enquiries: [email protected]
Predicting the risks of kidney failure and death in adults with moderate to severe chronic kidney disease: multinational, longitudinal, population based, cohort study
Affiliations.
- 1 Departments of Medicine and Community Health Sciences, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada.
- 2 Aberdeen Centre for Health Data Science, University of Aberdeen, Aberdeen, Scotland.
- 3 Department of Clinical Epidemiology, Department of Clinical Medicine, Aarhus University and Aarhus University Hospital, Aarhus, Denmark.
- 4 Department of Public Health, University of Copenhagen, Copenhagen, Denmark.
- 5 Departments of Medicine and Community Health Sciences, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada [email protected].
- PMID: 38621801
- DOI: 10.1136/bmj-2023-078063
Objective: To train and test a super learner strategy for risk prediction of kidney failure and mortality in people with incident moderate to severe chronic kidney disease (stage G3b to G4).
Design: Multinational, longitudinal, population based, cohort study.
Settings: Linked population health data from Canada (training and temporal testing), and Denmark and Scotland (geographical testing).
Participants: People with newly recorded chronic kidney disease at stage G3b-G4, estimated glomerular filtration rate (eGFR) 15-44 mL/min/1.73 m 2 .
Modelling: The super learner algorithm selected the best performing regression models or machine learning algorithms (learners) based on their ability to predict kidney failure and mortality with minimised cross-validated prediction error (Brier score, the lower the better). Prespecified learners included age, sex, eGFR, albuminuria, with or without diabetes, and cardiovascular disease. The index of prediction accuracy, a measure of calibration and discrimination calculated from the Brier score (the higher the better) was used to compare KDpredict with the benchmark, kidney failure risk equation, which does not account for the competing risk of death, and to evaluate the performance of KDpredict mortality models.
Results: 67 942 Canadians, 17 528 Danish, and 7740 Scottish residents with chronic kidney disease at stage G3b to G4 were included (median age 77-80 years; median eGFR 39 mL/min/1.73 m 2 ). Median follow-up times were five to six years in all cohorts. Rates were 0.8-1.1 per 100 person years for kidney failure and 10-12 per 100 person years for death. KDpredict was more accurate than kidney failure risk equation in prediction of kidney failure risk: five year index of prediction accuracy 27.8% (95% confidence interval 25.2% to 30.6%) versus 18.1% (15.7% to 20.4%) in Denmark and 30.5% (27.8% to 33.5%) versus 14.2% (12.0% to 16.5%) in Scotland. Predictions from kidney failure risk equation and KDpredict differed substantially, potentially leading to diverging treatment decisions. An 80-year-old man with an eGFR of 30 mL/min/1.73 m 2 and an albumin-to-creatinine ratio of 100 mg/g (11 mg/mmol) would receive a five year kidney failure risk prediction of 10% from kidney failure risk equation (above the current nephrology referral threshold of 5%). The same man would receive five year risk predictions of 2% for kidney failure and 57% for mortality from KDpredict. Individual risk predictions from KDpredict with four or six variables were accurate for both outcomes. The KDpredict models retrained using older data provided accurate predictions when tested in temporally distinct, more recent data.
Conclusions: KDpredict could be incorporated into electronic medical records or accessed online to accurately predict the risks of kidney failure and death in people with moderate to severe CKD. The KDpredict learning strategy is designed to be adapted to local needs and regularly revised over time to account for changes in the underlying health system and care processes.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Publication types
- Case Reports
- Aged, 80 and over
- Cohort Studies
- Glomerular Filtration Rate
- Kidney Failure, Chronic*
- North American People*
- Renal Insufficiency*
- Renal Insufficiency, Chronic* / complications
- Renal Insufficiency, Chronic* / epidemiology
Supplementary concepts
- Canadian people
- Open access
- Published: 15 April 2024
Life expectancy, long-term care demand and dynamic financing mechanism simulation: an empirical study of Zhejiang Pilot, China
- Xueying Xu 1 ,
- Yichao Li 2 &
- Hong Mi 2
BMC Health Services Research volume 24 , Article number: 469 ( 2024 ) Cite this article
39 Accesses
Metrics details
China has piloted Long-Term Care Insurance (LTCI) to address increasing care demand. However, many cities neglected adjusting LTCI premiums since the pilot, risking the long-term sustainability of LTCI. Therefore, using Zhejiang Province as a case, this study simulated mortality-adjusted long-term care demand and the balance of LTCI funds through dynamic financing mechanism under diverse life expectancy and disability scenarios.
Three-parameter log-quadratic model was used to estimate the mortality from 1990 to 2020. Mortality with predicted interval from 2020 to 2080 was projected by Lee-Carter method extended with rotation. Cohort-component projection model was used to simulate the number of older population with different degrees of disability. Disability data of the older people is sourced from China Health and Retirement Longitudinal Study 2018. The balance of LTCI fund was simulated by dynamic financing actuarial model.
Life expectancy of Zhejiang for male (female) is from 80.46 (84.66) years in 2020 to 89.39 [86.61, 91.74] (91.24 [88.90, 93.25]) years in 2080. The number of long-term care demand with severe disability in Zhejiang demonstrates an increasing trend from 285 [276, 295] thousand in 2023 to 1027 [634, 1657] thousand in 2080 under predicted mean of life expectancy. LTCI fund in Zhejiang will become accumulated surplus from 2024 to 2080 when annual premium growth rate is 5.25% [4.20%, 6.25%] under various disability scenarios, which is much higher than the annual growth of unit cost of long-term care services (2.25%). The accumulated balance of LTCI fund is sensitive with life expectancy.
Conclusions
Dynamic growth of LTCI premium is essential in dealing with current deficit around 2050 and realizing Zhejiang’s LTCI sustainability in the long-run. The importance of dynamic monitoring disability and mortality information is emphasized to respond immediately to the increase of premiums. LTCI should strike a balance between expanding coverage and controlling financing scale. This study provides implications for developing countries to establish or pilot LTCI schemes.
Peer Review reports
The lack of sufficient long-term care (LTC) for older individuals has become a pressing concern in both developed and developing countries with global population aging and increased longevity [ 1 ]. Although healthy life expectancy generally increased over last decades [ 2 ], the episode of disability in older people could have catastrophic impact on their household welfare [ 3 ]. Several developed countries, such as the Netherlands, Germany, and Japan, have established social long-term care insurance (LTCI) to address LTC demands of households with disabled older individuals. This approach proves more efficient in pooling disability risks than private LTCI [ 4 , 5 ]. Nonetheless, many developed countries had to reform their LTCI systems to deal with increasing aging population with LTC demands, often by raising premiums. Even though, these adjustments usually had time lags which affected the long-term sustainability of LTCI schemes. However, establishing social LTCI in developing countries proves more challenging than in developed countries because the lower income of residents restricts the financing capacity of LTCI. In addition, the lack of high-quality death registration and health survey data hinders optimizing LTCI systems design according to changing LTC demands, particularly in developing countries or small areas [ 6 ].
Massive evidence shows that there will be a steady and slow increase in life expectancy [ 7 , 8 , 9 ]. Evidence from developed countries shows that the long-term care needs increasing rapidly because of the increasing life expectancy [ 10 , 11 ]. The trend of the gap between life expectancy and healthy life expectancy is still inconclusive [ 12 ], which also affects the identification of LTC needs [ 13 ]. There is still mixed conclusion of disability and LTC demands trend in the future based on the three different assumptions of health transitions [ 14 , 15 , 16 ]. Whereas, there is less evidence regarding the assessment of LTC needs under different mortality scenarios. Zeng, et al. [ 17 ] calculated long-term care needs under different life expectancy scenarios, but the setting of life expectancy was relatively subjective. Besides, many studies in country-level controlled the impact of underreported mortality on the LTCI system by using modified mortality data [ 18 , 19 ], but few studies in the provincial level took that into consideration.
Most countries such as Germany and the Netherlands adopt a fixed percentage of income model to collect social LTCI premiums from individuals [ 20 ], and a few countries such as Singapore adopt a fixed amount premium model [ 21 ]. The premium of Germany LTCI has been 3.05% of gross income or 3.40% if individuals aged 23 and above without children since 2020 [ 22 ]. The Netherlands also has a tax-funded LTCI with the compulsory contribution of 9.65% of taxable income since 2017 [ 20 ]. In Singapore, fixed amount premium of LTCI is determined by the age of starting contribution and sex. The premium for a 30-year-old male (female) is around 200 (250) Singapore Dollars in 2020 [ 21 ], with an increase of 2% per year from 2020 to 2025 [ 23 ]. Financing parameters from both models should be adjusted regularly to ensure sustainability [ 24 , 25 ]. In China, both models are adopted in different LTCI pilot areas [ 26 ], but the areas that adopt the fixed amount of premium have not increased the premium level since the pilot, which affects long-term sustainability.
OECD countries will face high pressure of LTCI financing because of increasing average public LTC expenditures to 2.3% of GDP in 2040 for the future financing level of LTCI [ 27 ]. Therefore, an adjustment factor is suggested incorporated to simulate LTCI fund to reduce future financing pressure [ 22 ], but a higher short-term financing will bring greater resistance to reforms. Most simulation studies on China’s LTCI, based on fixed percentage of income model, demonstrated that LTCI financing will increase rapidly based on different disability scenarios [ 28 , 29 , 30 , 31 ]. Some studies also simulated LTCI financing based on fixed amount of premium model [ 32 , 33 ], but they did not consider its variation under different mortality scenarios. Only one study modified the mortality in a pilot city by using national mortality data when simulating the dynamic financing burden [ 34 ]. However, it only simulated to 2040 which did not cover plateau period of China’s aging.
China, as a developing country, pioneered social LTCI schemes in 2016. Local governments were granted significant autonomy, resulting in fragmented LTCI structures due to regional disparities in the pilot cities [ 35 ]. Thus it has become crucial to ensure the sustainability of China’s LTCI pilot areas. Zhejiang Province stands as a representative case among these pilot areas and its five cities (Tonglu, Ningbo, Jiaxing, Yiwu and Whenzhou) have piloted LTCI since 2017. Zhejiang has standardized disability assessments, coverage groups, benefit levels, and financing amounts of LTCI in province-level by 2022 [ 36 ]. It faces rapid aging ahead with high life expectancy in China. Notably, Zhejiang, one of the areas with fixed amount of premium of LTCI in China, has never increased its fixed premium since the pilot’s inception [ 36 ]. This lack of financing adjustment coupled with inflationary pressures strains Zhejiang’s LTCI fund. Zhejiang has capacities to facilitate LTCI operations through modified financing mechanism as the demonstration zone for the Initiative of Common Prosperity in China. Therefore, it can serve as a practical model for other developing countries establishing LTCI schemes to evaluate life expectancy and LTC demand parameters and guide its LTCI financing.
In summary, massive studies predict the LTC needs in developed countries and China. However, most of the studies on LTCI financing in China pilots overlook the potential death underreporting in census and uncertainty of mortality in projection period, which may misestimate the future LTC needs and financing pressure. In addition, current studies on the sustainability of China’s LTCI rarely involve the dynamic financing adjustment of fixed amount of premium model, and most studies do not cover the plateau period of China’s aging in the future, which may underestimate the financing level to achieve sustainable LTCI. Therefore, drawing from the Zhejiang Province case in China, this study proposes a dynamic financing mechanism to achieve a balance between sustainability and efficiency in social LTCI schemes, utilizing a simulation model with limited mortality and disability information. Our aim is to offer insights for developing countries to establish or pilot LTCI schemes. Three research questions will be addressed:
What is the long-term trend of life expectancy in Zhejiang from 1990 to 2080?
What extent of LTC demand will be reached among older people in Zhejiang from 2023 to 2080, with aging process?
What level of LTCI dynamic financing standards will achieve an actuarial equilibrium of the LTCI fund in Zhejiang, with rising life expectancy and LTC demand?
Data sources
For demographic data, the age-specific mortality and the population number by gender are from population census of Zhejiang Province in 1990, 2000, 2010 and 2020. The population census, which has been conducted once every 10 years since 1990, is a complete account of the entire population, mortality and fertility by age and sex in each census year and has the province-level representativeness of Zhejiang. Child mortality data is from Chinese Center for Disease Control and Prevention (CDC) in 1990–2013 [ 37 ], and official annual data of Zhejiang reported u p to 2020 [ 38 ]. Chinese CDC sorted and estimated under-5 mortality rates in China before 2013 with county-level and province-level representativeness, including data in Zhejiang. Data on the prevalence rate of disability of the older people is sourced from China Health and Retirement Longitudinal Study (CHARLS) in 2018. CHARLS is a national representative survey which covers a wide range of topics related to the adults aged 45 and above, including demographic information and health status. The national prevalence rate of disability by age and sex from CHARLS is used as a proxy for Zhejiang referring to existing research, due to lack of latest representative disability data in Zhejiang [ 39 ]. Older people are defined as those aged 60 and above based the statistical standards from World Health Organization [ 40 ], whose age groups are covered by CHARLS. The benefit criteria and financing criteria data is from the LTCI official regulations of pilot cities in Zhejiang [ 41 , 42 , 43 , 44 , 45 ]. Healthcare Consumer Price Index (CPI) from 2010 to 2020 in Zhejiang is from National Bureau of Statistics of China, covering the socio-economic indicators at province-level [ 46 ]. The change rate of total fertility of China from 2020 to 2080 is from World Population Prospects 2022 which forecasted fertility in country-level around the world [ 47 ].
Estimation of mortality pattern with three-parameter model life table approach
Model life tables methods are widely used in simulation of mortality for their effectiveness and accessibility to overcome the limited mortality information in developing countries [ 48 , 49 ]. Two-parameters log-quadratic model considering the child and adult mortality overcomes the shortage of Coale-Demeny and UN model life tables, among those model life tables methods [ 50 ]. Three-parameter log-quadratic model is designed on this to calculate the life table considering extra old-age mortality parameter with an adjustment of intercept with real census information [ 51 ]. It is so-called developing countries mortality database (DCMD) model which was adopted in the World Population Prospects 2019 since the three-parameter log-quadratic model life table was initially used in those developing countries without the high-quality mortality data [ 52 ]. The basic function of DCMD model is showed below:
This study used adjusted DCMD model to estimate the mortality in Zhejiang from 1990 to 2020 to make it usable for open population conditions. Child mortality ( \({\,}_{5}{q_0}\) ) is the first parameter of DCMD model, and adult mortality ( \({\,}_{{45}}{q_{15}}\) ) is the second parameter to be compared with estimated adult mortality ( \({\,}_{{45}}{\hat {q}_{15}}\) ) from two-parameter log-quadratic model with adjustment factor \(k\) . Specifically, child mortality by gender in consecutive years is estimated by sex ratio of child mortality in China [ 53 ]. Adult mortality in census years is calculated from census life table directly as the register completeness of adults’ death is higher in China [ 53 ]. Moreover, we averaged old-age mortality estimated from two-parameter log-quadratic model and from survival model for midpoint of old-age mortality between censuses (1995, 2005 and 2015) [ 51 ]. We averaged old-age mortality from two-parameter log-quadratic model and from census life table calculations for census years (1990, 2000, 2010 and 2020). The adjusted DCMD model was constructed on the incorporated old-age mortality. After that, the cubic hermite polynomial interpolation approach (pchip package in R) was adopted to estimate adult and old-age mortality from 1990 to 2020 [ 54 ]. The life table for consecutive years was estimated with DCMD model.
After that, Lee-Carter method extended with rotation (LC_ER) (mortcast package in R) was used to forecast the mortality up to 2080 [ 55 ], which provides critical death parameters to assess the LTCI demands in our case area. Since in low mortality countries, mortality decline is decelerating at younger ages and accelerating at older ages [ 56 ], the static assumption of mortality decline of traditional Lee-Carter model would be anomalous in long-term projection. LC_ER is a time-varying Lee-Carter model considering the changes of mortality decline between different age groups when modeling, which was widely recognized and adopted by World Population Prospects 2022 [ 57 , 58 ]. Therefore, potential LTCI demands change caused by changes in old-age mortality decline in long-term projections could be captured by LC_ER. The predicted mean of life expectancy would be set as the medium life expectancy scenario, and the lower and upper 95% predicted interval would be set as the low and high life expectancy scenarios.
Number of severe disabled older adults
LTCI beneficiaries refer to the severe disabled population according to the rules of LTCI in Zhejiang [ 36 ]. The study used the cohort-component projection (CCP) method to forecast the number of older population of Zhejiang from 2020 to 2080 [ 59 ]. The number of age-specific population by sex from Zhejiang population census 2020 was used as the base population of CCP model. Furthermore, the age-specific prevalence rate of disability from CHARLS 2018 was calculated. After that, the number of severe disabled older adults as the LTCI beneficiaries was calculated by multiplying age-specific older population and prevalence rate of disability. The basic project method is as follows:
\({\,}_{{x+1}}P_{x}^{{t+1}}\) represents the population of single age groups with the age of x to x + 1 at the t + 1 time. \(\left[ {{L^t}(x+1)/{L^t}(x)} \right]\) represents the survival ratio of age x to x + 1 at t time. \(N{I^*}\) represents the net migration numbers in the corresponding age group from the t to t + 1 period, from other regions to Zhejiang.
Our estimated mortality will be used in CCP model. Since the total fertility of Zhejiang is lower than that of China, this study assumed that the total fertility of Zhejiang would start at 1.04 in 2020 based on Zhejiang population census [ 60 ]. Then, the future trend of Zhejiang’s total fertility would follow the United Nations’ estimated change rate of total fertility of China from 2020 to 2080 [ 47 ]. For net migration, The Census Survival Ratio Method was used to estimate the migration pattern based on the census data [ 61 ]. As one of the highest net in-migration provinces since 2010, Zhejiang will face the lower net in-migration intensity and be close to migration equilibrium in 2040 [ 62 ]. Based on this, it is assumed that the net migration rate in Zhejiang will experience a linear decrease and realize migration equilibrium by 2045.
Disability is defined as a difficulty in performing at least one of six Activities in Daily Living (ADL) [ 63 ], including bathing, dressing, eating, getting in/out of bed, using the toilet, and controlling urination and defecation in CHARLS. Then, mild disability is defined as having difficulty in 1–2 items of ADL, moderate disability as having difficulty in 3–4 items of ADL, and severe disability as having difficulty in at least 5 items of ADL [ 64 , 65 ]. Based on the discussion on the Disease Expansion, Disease Compression and Dynamic Equilibrium Theory [ 66 ], three different scenarios in changing disability were calculated [ 16 ]: a 0.8% annual decrease for age-specific prevalence rate of disability as the low disability scenario, the constant age-specific prevalence rate of disability as the middle disability scenario, and a 0.8% annual increase for age-specific prevalence rate of disability as the high disability scenario.
Dynamic financing actuarial model of social LTCI schemes
The study built a macro simulation model to further simulate the expenditure, financing and fund balance of LTCI based on the projection of severe disabled older population ( \(DisOP\) ) aged 60 and above and contribution population ( \(CP\) ) of LTCI aged 20 and above. The macro model is showed below:
In Formula (4), \(LTCE\) means LTC expenditures, \(HbdcCost\) , \(IcCost\) , \(HbdmcCost\) and \(NhcCost\) represent the unit cost of home-based daily living care (HBDC), institutional care, home-based daily living & medical care (HBDMC) and nursing hospital care per person per year, respectively. Among them, HBDC means that beneficiaries only receive formal daily living care services at home but without any medical care. HBDMC means that beneficiaries receive both formal daily living care services and professional medical care services at home. The difference of institutional care and nursing hospital care lies in that the former focuses more on daily living care, while the latter specializes in medical care. From 2023 to 2080, the unit cost of each type of LTC services is given an increase of 2.25% annually based on the average increase of healthcare CPI from 2010 to 2020. \(\alpha \) means the percentage of different types of LTC services utilization. Formula (5) describes the dynamic financing model and current balance of LTCI every year. \(premiu{m_{{t_0}}}\) is the fixed amount of premiums of LTCI in our base period. \(\lambda \) is annual growth of the amount of LTCI premiums. Formula (6) shows the accumulated balance of LTC fund which is determined by the current balance and the accumulated balance in previous period. \(\gamma \) is the interest rate of LTCI fund which represents the time value of the LTCI fund. Taking the inflation rate (2.25%) as a reference in the simulation process, we test the minimum value of \(\lambda \) that ensures a consistently positive accumulated balance in the LTCI fund up to 2080 across various disability scenarios.
Parameters of LTCI schemes in Zhejiang Province, China
The policies of LTCI schemes in five pilot cities in Zhejiang are sorted in Additional Table 1 (see Additional file 1 ) [ 41 ]. The LTCI schemes in Jiaxing City are representative among five pilot cities of LTCI in Zhejiang. Firstly, Jiaxing is the first city covering all employees and urban and rural residents equitably with the same benefits and premium since the adoption of LTCI (in 2017), which has navigated the reform of LTCI in Zhejiang. Secondly, LTCI benefits in Jiaxing are at the middle level among the five pilot cities, which is representative of average level in Zhejiang. The maximum benefits of HBDC in Jiaxing are lower than those in Yiwu and Wenzhou, and equal to those in Tonglu and Ningbo. Besides, the maximum benefits of institutional care are also lower than those in Yiwu, but higher than those in Tonglu and Ningbo. Overall, Jiaxing’s LTCI benefits stay average in Zhejiang. Thirdly, LTCI financing criteria in Jiaxing align with Ningbo and Tonglu (90 Chinese Yuan (CNY)/person/year), reflecting the standards across five cities. Therefore, this study adopted Jiaxing’s LTCI criteria as the parameters of LTCI simulations in Zhejiang. The unit costs of HBDC, institutional care, HBDMC and nursing hospital care are set at 1200 CNY/month, 2100 CNY/month, 1680 CNY/month and 1680 CNY/month in 2024 according to LTCI maximum benefits in Jiaxing (see Additional Table 1 , Additional file 1 ) [ 41 ]. The contributory group of LTCI is the group participating in social health insurance, whether retired or not. The LTCI financing parameter \(premiu{m_{{t_0}}}\) is based on a fixed amount of premiums in Jiaxing, of which the standard is 90 CNY/person/year [ 41 ].
Chinese government proposed a model of elderly care named “9073” model: 90% of older people receive home-based care, 7% receive community care and 3% receive institutional care [ 67 ]. “9073” model represents the prospects of China’s elderly care and is therefore suitable for the long-term simulation in this study [ 29 , 62 ]. Specifically, proportion of HBDC ( \({\alpha _{\text{1}}}\) ), institutional care ( \({\alpha _2}\) ), and combination of HBDMC and nursing hospital care ( \({\alpha _3}\) + \({\alpha _4}\) ) are set at 90%, 3% and 7%, respectively. Disabled older people can choose to receive HBDMC at home or receive nursing hospital care at medical institutions when facing medical care needs. It is free to choose the locations for these two LTC services, and it is quite similar to receiving community care in nature, as it also allows the option of receiving services at home or at community centers. Additionally, the LTCI benefits of these two LTC services in Jiaxing are equal. Therefore, we grouped them together when determining the beneficiaries’ choice of LTC services type ( \({\alpha _3}\) + \({\alpha _4}\) ). We set the interest rate of LTCI fund at 2.5% based on current interest rate of 5-year time deposit in China’s banks [ 68 ]. The sources of each parameter for simulation framework of the study are demonstrated in Additional Fig. 1 (see Additional File 1 ).
The mortality pattern and life expectancy of Zhejiang
The estimated mortality of Zhejiang from 1990 to 2020 is demonstrated in Fig. 1 based on adjusted DCMD model. Overall, the mortality for male and female presents a declining trend. Specially, the child mortality had a continued decline during the estimation period, but the adult mortality and old-age mortality had a slight increase between 1990 and 2000, then with a sharp decline between 2000 and 2020 afterwards.
We further predict the life expectancy at birth with 95% confidential interval under the LC_ER model from 2020 to 2080. The estimated and predicted life expectancy is demonstrated in Fig. 2 . Life expectancy of female had a stable increase from 1990 to 2020. While there was a slight decline of life expectancy of male from 1990 to 2000, then there was a rapid increase until 2020. The model results based on historical information show that life expectancy of both female and male will have an upward trend from 2020 to 2080. Besides, the gender difference in life expectancy will remain relatively stable in the future. In 2020, life expectancy was 80.46 years for male, 84.66 years for female. In 2080, the life expectancy will reach 89.39 [86.61, 91.74] years for male, 91.24 [88.90, 93.25] years for female. Besides, the age-specific rates of mortality decline of Zhejiang from 2021 to 2080 estimated by LC_ER are illustrated in Additional Fig. 2 (see Additional File 1 ).

Mortality pattern of Zhejiang in 1990–2020 based on adjusted DCMD model

Estimated and predicted life expectancy of Zhejiang in 1990–2080
The simulation of long-term care demand and expenditures in Zhejiang
Based on CCP method, the study has projected the number of older people and the number of severely disabled older people with different scenarios of disability in Zhejiang from 2020 to 2080 (shown in Table 1 ). It is illustrated that the population aged 60 and above in Zhejiang will firstly expand to around 2060 and then shrink until 2080. The number of older people with disabilities, especially those with severe disability, reflects the long-term care demand from a demographic perspective. We found that the number of older people with severe disability will continue to increase to 2080 under both medium and high disability scenarios. However, the number of older people with different degrees of disability will increase before 2060, and then decline slightly in the following 20 years under the low disability scenario. We also found that the number of severely and moderately disabled older people will be of little difference before 2050, which means that severe and moderate LTC demand is roughly equal.
Besides, the results of LTC demand under the high and low life expectancy scenarios are illustrated in Additional Table 2 and Additional Table 3 (see Additional file 1 ). It can be seen that Zhejiang Province will have a higher LTC demand under the scenario of higher life expectancy. The number of older people with severe disability under 95% upper interval of life expectancy in 2080 is 154 thousands higher than that under the predicted mean of life expectancy. And the number of older people with severe disability under 95% lower interval of life expectancy in 2080 is 169 thousands lower than that under the predicted mean of life expectancy. This result demonstrates the importance of mortality level prediction for assessing LTC demand.
Our study further calculated the LTCI expenditure paid by insurance fund every year from 2020 to 2080 to analyze the future long-term care demand in our case area from a financial perspective. The expenditure from LTCI illustrates an upward trend from 2023 to 2080 (see Fig. 3 ), with the higher price of long-term care services and increasing number of severe disabled older people. The LTCI expenditure is still increasing although there will be a slight decline in severe disabled older people under low disability scenario.

Projection of Long-term care insurance expenditure in Zhejiang, 2024–2080. Notes Results are based on the predicted mean of life expectancy
The simulation of LTCI fund under diverse disability and financing scenarios
The accumulated balance of LTCI fund from 2022 to 2080 is simulated on different dynamic financing growth scenarios in order to test how to make LTCI achieve actuarial balance in the long run. The accumulated balance and current balance of LTCI fund in Zhejiang are shown in Figs. 4 and 5 . When we set the annual premium growth rate at 2.25% which is equal to the average increase of healthcare CPI, there will be a deficit of current balance before 2028. As a result, the accumulated balance will become negative in 2032 under medium disability scenario, under high disability scenario in 2030 and under low disability scenario in 2036. This result shows that LTCI fund can only be sustainable within 12 years if the financing level grows at a low pace from 2024.

Accumulated balance of LTCI fund under different financing and disability scenarios. Notes Results are based on the predicted mean of life expectancy

Current balance of LTCI fund under different financing and disability scenarios. Notes Results are based on the predicted mean of life expectancy
The minimum annual premium growth is further tested to achieve the positive accumulated balance of LTCI fund under various scenarios from 2022 to 2080. We found that when the annual premium growth rate equals to 4.20%, LTCI fund will realize the long-term sustainable under low disability scenario, which means that the 4.20% financing growth standard is effective to make LTCI sustainable at a relatively low premium level under low disability scenario; however, it will still face the risk of the shortage of financing with 4.20% annual premium growth under the medium and high disability scenarios after 2039 and 2033.
Furthermore, the accumulate balance of LTCI fund remains at a moderate surplus and will not face a shortage until 2080 under the medium disability scenario when the annual premium growth rate equals 5.25%. Although the current balance of LTC fund will be negative in 2043 to 2058 under 5.25% annual premium growth (see Fig. 5 ), the accumulated surplus before 2042 and continuous interest will still realize the accumulated surplus of LTCI fund (5.83 billion CNY) in 2058. Overall, the annual premium growth rate at 5.25% is the best parameter choice if the age-specific prevalence rate of disability in Zhejiang Province is projected to remain stable. Finally, LTCI will be sustainable under all disability scenarios when the premium increases by 6.25% per year. However, this level will put a heavy payment burden on the residents, and there will be a large amount of fund redundancy if the disability does not continue to increase.
The simulation of LTCI fund under diverse life expectancy and financing scenarios
The impact of different life expectancy trend on the sustainability of LTCI schemes is further discussed. The simulation results of accumulated balance of LTCI fund under predicted mean, 95% upper confidential interval and lower confidential interval of life expectancy scenarios are demonstrated in Fig. 6 . It is learned that the sustainability of the LTCI fund will face a completely different situation in the long-term because of the difference trends in life expectancy even under the same disability level and financing level. Under the 5.25% annual premium growth rate and medium disability scenario, LTCI fund will become accumulated deficit under 95% upper interval of life expectancy after 2045. However, the LTCI fund will always remain in surplus before 2080 with the predicted mean or lower 95% interval of life expectancy. Therefore, the balance of LTCI fund is sensitive to life expectancy. In addition to affecting LTC expenditures when other conditions are the same, life expectancy is also related the total amount of financing by the number of contributors, thereby influencing the sustainability of LTCI fund.

Current and accumulated balance of LTCI under different life expectancy scenarios. Notes Results are based on the 5.25% annual premium growth rate scenario and medium disability scenario
This study shows two novel contributions to the existing literature. The first contribution is that we have found an important but often overlooked point that LTCI financing is sensitive to the variability of life expectancy in the long-term. In 2080, the 95% upper interval of the life expectancy in Zhejiang Province will be 2.01 years for female (2.35 years for male) higher than the predicted mean, and its cumulative impact will make LTCI unsustainable 35 years in advance. This finding shows that the accurate estimation of life expectancy is critical for assessing the sustainability of social insurance schemes like LTCI [ 69 , 70 ], and also reveals the significance of life expectancy analysis in this study, because health factors can be dynamically monitored through the evaluation and reimbursement records within the LTCI system [ 34 , 71 ], but life expectancy estimation will become difficult due to the lack of timely statistical data. Besides, the study also finds that LTCI financing is also sensitive to the variability of prevalence rate of disability in the long-term. Only 4.20% annual growth of premium can make Zhejiang’s LTCI sustainable under a disability compression assumption. However, the 6.25% annual growth of premium is necessary for Zhejiang’s LTCI sustainability under disability expansion assumption. The results are consistent with some existing research with various disability scenarios [ 28 , 72 ]. The overall incidence of disability will face a growing trend with population aging [ 17 ]. Therefore, proposing health promotion and postponing disability actions to reduce the incidence and duration of severe disability among older people will mitigate the pressure of LTCI funding [ 73 ].
The second contribution is that Zhejiang’s LTCI financing needs to grow at a relative high speed annually (5.25% under the medium scenario) to achieve sustainability in the long-term. It should be noticed that the LTCI financing parameters to achieve short-term and long-term fund equilibrium are different, and it is clear that long-term fund balance is a necessary condition to ensure the sustainability of the system [ 22 , 29 ]. If the accumulated surplus of the LTCI fund in Zhejiang Province before 2050 is used as a criterion for determining sustainability, as many studies have done [ 19 , 74 ], our results indicate that Zhejiang LTCI fund is projected to experience an accumulating deficit for over 20 years after 2050. Like Zhejiang, there are also several pilot cities in China that have adopted the fixed amount of premium model without premium adjustment [ 32 ]. LTCI funds in these regions will run the risk of accumulating deficits in the short term [ 43 ]. China and other countries adopting social LTCI need to adjust the scale of premium in a timely and dynamic manner to cope with the long-term LTCI financing pressure since China’s aging plateau will continue after 2060 [ 47 ].
Our simulation results can also be used as a reference for countries and regions that adopt a fixed percentage of income model of LTCI financing although we focus on the fixed amount model of LTCI financing. The study finds that LTCI premium in Zhejiang needs to increase by 5.25% per year to ensure sustainability to 2080 under the assumption of disability with dynamic equilibrium. However, the growth rate may exceed the income growth rate of some countries in the context of declining global economic growth [ 75 ]. Therefore, even those countries based on a fixed percentage of income model need adjust financing parameters dynamically [ 1 ]. In LTCI fund management, China and other countries can learn from Germany’s experience to deal with the long-term impact of population aging, which has established a demographic reserve fund which saves 0.1% of premium every year for payment in the future [ 25 ].
Reasonable coverage and benefits are also important factors to achieve sustainable LTCI. Like developed countries, the LTCI pilot cities in Zhejiang Province cover all urban and rural residents. However, most of the LTCI pilot cities in China only cover urban employees [ 35 ]. Therefore, the analysis of LTCI in Zhejiang Province in this paper provides implications for other LTCI pilot cities in China to expand the coverage and promote the equity of receiving LTC. Besides, it should be noted that this study only considers the older adults with severe disabilities according to the rules when estimating LTC needs in Zhejiang Province [ 36 ]. Whereas, it is not only the families of severely disabled groups that face the burden of long-term care [ 17 ]. Moderately disabled people in some developed countries and pilot cities in China are also covered by LTCI [ 76 , 77 ]. Even considering only severe disability, our simulation results show that only a high premium growth rate can make the system sustainable in the long run. Therefore, LTCI policymakers need to comprehensively weigh residents’ payment pressure and long-term care benefits, and make a balance between expanding coverage and increasing financing with the aim of protecting the most vulnerable groups.
This study has explored and built a long-term care insurance system that can be a reference for China and other developing countries to provide LTC services for the disabled older adults in the future. The strength of this study is that a more accurate life expectancy estimation based on the DCMD model is adopted when estimating dynamic financing of LTCI. However, this paper still has some limitations. Firstly, the paper only considers the activities of daily living when estimating the prevalence rate of disability of older people in Zhejiang Province, but does not consider cognitive function, perception and communication function due to the lack of data. Secondly, this study only considers the expenditure cost of LTC in the simulation analysis, but does not consider the operating cost of the LTCI system. Thirdly, this study only considers the total amount of financing for LTCI, but does not discuss the financing structure including individual contributions, government subsidies, and pooling funds. Finally, this study focuses only on the case in Zhejiang, but does not simulate the LTCI financing standard for actuarial equilibrium in other LTCI pilot areas in China.
In summary, this study estimates and predicts the mortality rate in Zhejiang Province from 1990 to 2080 through the DCMD model and LC model, and further evaluates the increasing LTC need in Zhejiang Province in the future. The LTCI dynamic financing in Zhejiang Province under different disability scenarios and life expectancy scenarios is simulated on the LTCI expenditure forecast results, and it is found that only by maintaining a relatively high level (5.25% under medium scenario) of premium growth can Zhejiang’s LTCI be sustainable in the long run. Our empirical case in Zhejiang offers implications for developing countries and LTCI pilot areas that lack high-quality mortality information to establish and dynamically optimize LTCI financing. Therefore, policy makers are called upon to assess the sustainability of LTCI from a long-term perspective, and regularly monitor changes in residents’ health and life expectancy to ensure that LTCI fund can meet LTCI expenditure and control the financing burden.
Data availability
In this study, all the data sources are publicly available. The data calculated in this study is available upon request to the corresponding author.
Abbreviations
Long-term care
- Long-term care insurance
China Health and Retirement Longitudinal Study
Center for Disease Control and Prevention
Consumer Price Index
Developing Country Mortality Database
Lee-Carter method extended with rotation
Cohort-component projection
Chinese Yuan
Home-based daily living care
Home-based daily living & medical care
Chen L, Zhang L, Xu X. Review of evolution of the public long-term care insurance (LTCI) system in different countries: influence and challenge. BMC Health Serv Res. 2020;20:1–21.
Article CAS Google Scholar
Collaborators GBD, Ärnlöv J. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950–2019: a comprehensive demographic analysis for the global burden of Disease Study 2019. Lancet. 2020;396(10258):1160–203.
Article Google Scholar
Cullinan J, Gannon B, O’Shea E. The welfare implications of disability for older people in Ireland. Eur J Health Econ. 2013;14:171–83.
Article PubMed Google Scholar
Karagiannidou M, Wittenberg R. Social Insurance for Long-Term Care. J Popul Ageing. 2022;15(2):557–75.
Article PubMed PubMed Central Google Scholar
Brown JR, Finkelstein A. The private market for Long-Term Care Insurance in the United States: a review of the evidence. J Risk Insur. 2009;76(1):5–29.
Cardoso T, Oliveira MD, Barbosa-Póvoa A, Nickel S. Modeling the demand for long-term care services under uncertain information. Health Care Manag Sc. 2012;15:385–412.
Liou L, Joe W, Kumar A, Subramanian SV. Inequalities in life expectancy: an analysis of 201 countries, 1950–2015. Soc Sci Med. 2020;253:112964.
Leon DA, Jdanov DA, Shkolnikov VM. Trends in life expectancy and age-specific mortality in England and Wales, 1970–2016, in comparison with a set of 22 high-income countries: an analysis of vital statistics data. Lancet Public Health. 2019;4(11):e575–82.
Vollset SE, Goren E, Yuan C-W, Cao J, Smith AE, Hsiao T, Bisignano C, Azhar GS, Castro E, Chalek J. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: a forecasting analysis for the global burden of Disease Study. Lancet. 2020;396(10258):1285–306.
Spillman BC, Lubitz J. The effect of longevity on spending for acute and long-term care. New Engl J Med. 2000;342(19):1409–15.
Article CAS PubMed Google Scholar
Schulz E, Leidl R, König H-H. The impact of ageing on hospital care and long-term care—the example of Germany. Health Policy. 2004;67(1):57–74.
Cao X, Hou Y, Zhang X, Xu C, Jia P, Sun X, Sun L, Gao Y, Yang H, Cui Z. A comparative, correlate analysis and projection of global and regional life expectancy, healthy life expectancy, and their GAP: 1995–2025. J Glob Health. 2020;10(2).
Rickayzen BD, Walsh DE. A multi-state model of disability for the United Kingdom: implications for future need for long-term care for the elderly. Brit Actuar J. 2002;8(2):341–93.
Crimmins EM, Beltrán-Sánchez H. Mortality and morbidity trends: is there compression of morbidity? J Gerontol B-Psychol. 2011;66(1):75–86.
Chatterji S, Byles J, Cutler D, Seeman T, Verdes E. Health, functioning, and disability in older adults—present status and future implications. Lancet. 2015;385(9967):563–75.
Bai C, Chen H, Wang Z, Zeng Y. Regional Comparative Research of Home-based care needs and costs Predictionfor Disabled elders in China. China Econ Quart. 2022;22(02):653–76.
Google Scholar
Zeng Y, Chen H, Wang Z, Land KC. Implications of changes in households and living arrangements for future home-based care needs and costs for disabled elders in China. J Aging Health. 2015;27(3):519–50.
Vanella P, Heß M, Wilke CB. A probabilistic projection of beneficiaries of long-term care insurance in Germany by severity of disability. Qual Quant. 2020;54(3):943–74.
Zhang L, Fu S, Fang Y. Prediction the contribution rate of long-term care insurance for the aged in China based on the balance of supply and demand. Sustainability-Basel. 2020;12(8):3144.
Villalobos Dintrans P. Designing long-term care systems: elements to consider. J Aging Soc Policy. 2020;32(1):83–99.
Fong JH, Borowski A. Long-term care insurance reform in Singapore. J Aging Soc Policy. 2022;34(1):73–90.
Bahnsen L, Wimmesberger FM. Curbing the demographic drifting dune in long-term care insurance financing: the case of Germany. Int Soc Secur Rev. 2023;76(1):35–56.
Central Provident Fund Board of Singapore. CareShield Life premiums and subsidies. 2020. https://www.cpf.gov.sg/member/healthcare-financing/careshield-life/careshield-premiums-and-subsidies . Accessed 01 February 2024.
Kim H, Kwon S. A decade of public long-term care insurance in South Korea: policy lessons for aging countries. Health Policy. 2021;125(1):22–6.
Nadash P, Doty P, von Schwanenflügel M. The German long-term Care Insurance Program: evolution and recent developments. Gerontologist. 2018;58(3):588–97.
Feng Z, Glinskaya E, Chen H, Gong S, Qiu Y, Xu J, Yip W. Long-term care system for older adults in China: policy landscape, challenges, and future prospects. Lancet. 2020;396(10259):1362–72.
Biase Pd, Dougherty S. From local to national: delivering and financing effective long-term care. Paris: OECD Publishing; 2023. https://doi.org/10.1787/578b296f-en .
Book Google Scholar
Zhang L, Fu S, Wang Y, Fang Y. Research on the optimization of financing scheme of long-term care insurance in China based on system dynamics simulation. Front Public Health. 2022;10:908864.
Guo P, Li Y. Innovation and financial sustainability in China’s long-term care insurance: an empirical analysis of the Nantong pilot. Front Public Health. 2022;10:1024491.
Zhang L, Fu S, Fang Y. Research on financing mechanism of long-term care insurance in Xiamen, China: a system dynamics simulation. Front Public Health. 2021;9:714044.
Mi H, Ji M, Liu W. Long-term Care Insurance Blue Book 2018: research on long-term Care Insurance in Qingdao, China. Beijing, China: China Human Resources Social Security Publishing Group Co, Ltd; 2019.
Chen H, Zhao S, Cui B. An evaluation study on the risk of financial deficit for the long-term care insurance pilots: based on analysis of the operational scheme in the 15 first-batch pilots. Chin J Health Policy. 2021;14(12):42–50.
Yang H, Fan W, Jiang W. Estimation of the financing burden of long-term care insurance funds:comparative analysis based on 8 LTC insurance pilot regions. Chin J Health Policy. 2023;16(06):1–9.
Chen H, Zhao S. Financial sustainability of the long-term Care Insurance-based on Microsimulation and Claims Data. Insur Stud. 2021;(10): 64–78.
Zhou W, Dai W. Shifting from fragmentation to integration: a systematic analysis of long-term care insurance policies in China. Int J Integr Care. 2021; 21(3).
Zhejiang Healthcare Security Administration. Guiding Opinions on Deepening the Pilot Program of the Long-Term Care Insurance System. 2022. http://ybj.zj.gov.cn/art/2022/6/28/art_1229113757_2409463.html . Accessed 14 April 2023.
Wang Y, Li X, Zhou M, Luo S, Liang J, Liddell CA, Coates MM, Gao Y, Wang L, He C. Under-5 mortality in 2851 Chinese counties, 1996–2012: a subnational assessment of achieving MDG 4 goals in China. Lancet. 2016;387(10015):273–83.
Zhejiang Provincial Statistics Bureau. Statistical monitoring report of children’s development planning in Zhejiang Province. 2020. http://tjj.zj.gov.cn/art/2020/9/30/art_1229129214_3637001.html . Accessed 14 April 2023.
Liu H. Research on disability grading based on ICF functional framework: empirical evidence from Zhejiang Province, China. Front Public Health. 2021;9:616180.
WHO. World report on ageing and health. World Health Organization; 2015.
Jiaxing Municipal Bureau of Healthcare Security. Long-term care insurance pilot implementation opinion for standard creation and efficiency improvement in Jiaxing city. 2023. https://ybj.jiaxing.gov.cn/art/2023/12/22/art_1229562038_2504155.html . Accessed 24 January 2024.
Wenzhou Healthcare Security Administration. Wenzhou City’s Implementation Plan for Deepening the Pilot of Long-term Care Insurance System (2023–2025). 2023. https://ybj.wenzhou.gov.cn/art/2023/5/24/art_1229135971_2022182.html . Accessed 02 February 2024.
Ningbo Municipal People’s Government. Guiding Opinions of the General Office of the Ningbo Municipal People’s Government on Deepening the Pilot of the Long-term Care Insurance System. 2022. https://www.ningbo.gov.cn/art/2022/9/13/art_1229533176_1752149.html . Accessed 02 February 2024.
Yiwu Healthcare Security Administration. Notice on adjusting some provisions of the. Yiwu City Long-term Care Insurance System Implementation Opinions (Trial). 2023. https://www.yw.gov.cn/art/2023/11/22/art_1229355060_52809.html . Accessed 02 February 2024.
Tonglu Healthcare Security Administration. Notice from Tonglu Medical Security Bureau on adjusting some policies of long-term care insurance. 2022. http://www.tonglu.gov.cn/art/2022/11/22/art_1229740453_1827580.html . Accessed 02 February 2024.
National Bureau of Statistics of China. National Data. 2023. https://data.stats.gov.cn/index.htm . Accessed 2 June 2023.
United Nations. World Population Prospects 2022. 2022. https://population.un.org/wpp/ . Accessed 27 July 2023.
Liu Z, Zheng H, Wu Y, Wang S, Liu Y, Hu S. Self-rated healthy life expectancy changes in Jiangxi Province of China by gender and urban–rural differences, 2013–2018. Front Public Health. 2021;8:596249.
Pandey SP, Adair T. Estimation of national and subnational all-cause mortality indicators in Nepal, 2017. BMC Public Health. 2022;22(1):1–11.
Wilmoth J, Zureick S, Canudas-Romo V, Inoue M, Sawyer C. A flexible two-dimensional mortality model for use in indirect estimation. Pop Stud-J Demog. 2012;66(1):1–28.
Li N, Mi H, Gerland P. Using child, adult, and old-age mortality to establish a Developing Countries Mortality Database (DCMD). Demography and Health Issues: Population Aging, Mortality and Data Analysis. 2018:51–62.
United Nations. World Population Prospects 2019: Methodology of the United Nations population estimates and projections. 2019. https://population.un.org/wpp2019/Publications/Files/WPP2019_Methodology.pdf . Accessed 27 July 2023.
Li C, Mi H. Assessments of provincial mortality in China’s 2010 population census based on the developing Countries Mortality Database model life table. J Popul Res. 2021;38(2):169–96.
WHO. WHO methods and data sources for life Tables 1990–2016. 2018. https://cdn.who.int/media/docs/default-source/gho-documents/global-health-estimates/lt_method_2016.pdf . Accessed 27 July 2023.
Li N, Lee R, Gerland P. Extending the Lee-Carter method to model the rotation of age patterns of mortality decline for long-term projections. Demography. 2013;50(6):2037–51.
Chen Z, Shi Y, Shu A. Managing Mortality and Aging Risks with a Time-Varying Lee–Carter Model. In: Healthcare-Basel : 2023: MDPI; 2023: 743.
Basellini U, Camarda CG, Booth H. Thirty years on: a review of the Lee–Carter method for forecasting mortality. Int J Forecast. 2023;39(3):1033–49.
United Nations. World Population Prospects 2022: Methodology of the United Nations Population Estimates and Projections. 2023. https://population.un.org/wpp/Publications/Files/WPP2022_Methodology.pdf . Accessed 01 February 2024.
Preston SH, Heuveline P, Guillot M. Demography: measuring and modeling population processes. Blackwell; 2000.
Zhejiang Provincial Bureau of Statistics. Part One of the Series Analysis of the Seventh Census of Zhejiang Province: Total Number and Distribution. 2022. https://tjj.zj.gov.cn/art/2022/7/22/art_1229129214_4955981.html . Accessed 01 Feb 2024.
Zachariah KC. A note on the census survival ratio method of estimating net migration. J Am Stat Assoc. 1962;57(297):175–83.
Deng Y, Liu S, Cai J, Lu X, Nielsen CP. Spatial pattern and its evolution of Chinese provincial population: methods and empirical study. J Geogr Sci. 2015;25:1507–20.
Jette AM. How measurement techniques influence estimates of disability in older populations. Soc Sci Med. 1994;38(7):937–42.
Manton KG, Gu X, Lamb VL. Change in chronic disability from 1982 to 2004/2005 as measured by long-term changes in function and health in the US elderly population. P Natl Acad Sci Usa. 2006;103(48):18374–9.
Chen L, Shi X. Forecast of China’s Long-Term Care Insurance Fund demand. Chin J Popul Sci. 2021;06:54–67.
Cai L, Lubitz J. Was there compression of disability for older americans from 1992 to 2003? Demography. 2007;44(3):479–95.
Hu B, Li B, Wang J, Shi C. Home and community care for older people in urban China: receipt of services and sources of payment. Health Soc Care Comm. 2020;28(1):225–35.
Zhu M, He M, Ma Z. Improving long-term Care Insurance: Model Selection and System Design. Chin J Popul Sci. 2023;01:3–20.
Lamnisos D, Giannakou K, Jakovljevic M. Demographic forecasting of population aging in Greece and Cyprus: one big challenge for the Mediterranean health and social system long-term sustainability. Health Res Policy Sy. 2021;19(1):21.
Bai R, Liu Y, Zhang L, Dong W, Bai Z, Zhou M. Projections of future life expectancy in China up to 2035: a modelling study. Lancet Public Health. 2023.
Liu C, Shu R, Liang H, Liang Y. Multimorbidity patterns and the disablement process among Public Long-Term Care Insurance Claimants in the City of Yiwu (Zhejiang Province, China). Int J Env Res Pub He. 2022;19(2):645.
Schut FT, Van Den Berg B. Sustainability of Comprehensive Universal Long-Term Care Insurance in the Netherlands. Soc Policy Admin. 2010;44(4):411–35.
Campbell JC, Ikegami N, Gibson MJ. Lessons from public long-term care insurance in Germany and Japan. Health Affair. 2010;29(1):87–95.
Kim N. Long-term care services expenditure projection in South Korea from 2015 to 2050. Int J Health Plan M. 2015;30(1):45–56.
International Monetary Fund. World Economic Outlook Update. 2023. https://www.imf.org/en/Publications/WEO/Issues/2023/07/10/world-economic-outlook-update-july-2023 . Accessed 15 August 2023.
Zhu Y, Österle A. China’s policy experimentation on long-term care insurance: implications for access. Int J Health Plan M. 2019;34(4):e1661–74.
Rhee JC, Done N, Anderson GF. Considering long-term care insurance for middle-income countries: comparing South Korea with Japan and Germany. Health Policy. 2015;119(10):1319–29.
Download references
Acknowledgements
We would like to thank Professor Xiangming Fang from Zhejiang University, Professor Guangdi Chen from Zhejiang University and Chengxu Long from King’s College London for their constructive advice during the research process of the paper. We would also like to appreciate any comments from the 34th REVES meeting.
This work was supported by the Major Project of Zhejiang Provincial Natural Science Foundation of China (LD21G030001).
Author information
Authors and affiliations.
School of International Studies, Zhejiang University, Hangzhou, China
School of Public Affairs, Zhejiang University, Hangzhou, China
Yichao Li & Hong Mi
You can also search for this author in PubMed Google Scholar
Contributions
All authors contributed to the conception and design of the study, as well as the planning of analyses. XX and YL drafted the manuscript and performed the simulation analyses. YL & HM planned and prepared the simulation analyses. All authors took part in the revision of the manuscript for important intellectual content.
Corresponding author
Correspondence to Yichao Li .
Ethics declarations
Ethics approval and consent to participate.
Not applicable.
Consent for publication
Competing interests.
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Xu, X., Li, Y. & Mi, H. Life expectancy, long-term care demand and dynamic financing mechanism simulation: an empirical study of Zhejiang Pilot, China. BMC Health Serv Res 24 , 469 (2024). https://doi.org/10.1186/s12913-024-10875-7
Download citation
Received : 26 August 2023
Accepted : 18 March 2024
Published : 15 April 2024
DOI : https://doi.org/10.1186/s12913-024-10875-7
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Life expectancy
- Dynamic financing model
- Simulation analysis
- Zhejiang province
BMC Health Services Research
ISSN: 1472-6963
- General enquiries: [email protected]
IMAGES
VIDEO
COMMENTS
Revised on June 22, 2023. In a longitudinal study, researchers repeatedly examine the same individuals to detect any changes that might occur over a period of time. Longitudinal studies are a type of correlational research in which researchers observe and collect data on a number of variables without trying to influence those variables.
Case-control studies look at a single subject or a single case, whereas longitudinal studies are conducted on a large group of subjects. 3. Does a longitudinal study have a control group? Yes, a longitudinal study can have a control group. In such a design, one group (the experimental group) would receive treatment or intervention, while the ...
A classic example of longitudinal case study is the study of Middletown (a mid-sized city in Midwestern United States) by Lynd and Lynd , once in mid-1920s and again in mid-1930s. Though it is basically a descriptive case study, the primary focus of the authors was the transition from an agricultural to an industrial economy, which occurred in ...
A longitudinal study (or longitudinal survey, or panel study) is a research design that involves repeated observations of the same variables (e.g., people) over long periods of time (i.e., uses longitudinal data ). It is often a type of observational study, although it can also be structured as longitudinal randomized experiment. [1]
A longitudinal study is an experimental design that takes repeated measurements of the same subjects over time. These studies can span years or even decades. Unlike cross-sectional studies, which analyze data at a single point, longitudinal studies track changes and developments, producing a more dynamic assessment.
CRD and LRD. Based on the number of time periods for which the same variable is measured, the research designs in social sciences are broadly classified into two types: CRD and LRD. In CRD, the researcher collects the data on one or more than one variable for a single time period for each case in the study. The researcher measures the variables ...
Employing a fully longitudinal mixed methods case study design, we examined the physical and psychological changes in a chronically ill older person via telenursing video consultations. We collected daily measures of his physical state and conducted clinical interviews before and during the COVID-19 pandemic. Our two-step approach integrated ...
Instead, we called it a longitudinal case study. It was relatively easy to conduct a longitudinal case study when we (the authors) and our participants were all at the same institution. The challenges came a few years later when our careers moved us to different institutions, 2500 km apart, and our participants moved into 22 different ...
A longitudinal study alleviates the problem since it involves multiple observations of the same population over a longer period of time. A major benefit of a longitudinal study is that researchers can examine changes within individuals and groups in the target population. To return to the previous example, longitudinal data can demonstrate ...
The Framingham study is widely recognised as the quintessential longitudinal study in the history of medical research. An original cohort of 5,209 subjects from Framingham, Massachusetts between the ages of 30 and 62 years of age was recruited and followed up for 20 years.
Longitudinal case studies would seem to be a natural research strategy for investigating behaviour over time, however whilst there are guidelines [56], [73] emerging in the empirical software engineering research community on the design, conduct and reporting of case studies, there is very little attention directed in these guidelines at ...
A longitudinal study is observational and involves the continuous and repeated measurements of selected individuals followed over a period of time. Quantitative and qualitative data is gathered on "any combination of exposures and outcome." ... Handling attrition in longitudinal studies: the case for refreshment samples. Stat Sci, 28 (2 ...
Qualitative longitudinal research (QLR) comprises qualitative studies, with repeated data collection, that focus on the temporality (e.g., time and change) of a phenomenon. The use of QLR is increasing in health research since many topics within health involve change (e.g., progressive illness, rehabilitation). A method study can provide an insightful understanding of the use, trends and ...
Background. Longitudinal qualitative methods are becoming increasingly used in the health service research, but the method and challenges particular to health care settings are not well described in the literature.We reflect on the strategies used in a longitudinal qualitative study to explore the experience of symptoms in cancer patients and their carers, following participants from diagnosis ...
This chapter reports the methods and findings from the longitudinal qualitative case study. In line with contemporary process evaluation guidance, this is an in-depth, pre-planned and theoretically driven longitudinal, comparative, qualitative case study to support understanding of two complex interventions that aim to reduce UI in women.53 In this chapter, we refer to the interview ...
Case study often implies the collection of unstructured data and qualitative analysis of those data. Additionally, it is often argued that the aim of case study research should be to capture cases in their uniqueness, rather than to use them as a basis for wider generalization or theoretical inference of some kind. Hence, it often raises a fundamental issue about the aspect of trustworthiness ...
In this report, the authors describe a first-of-its-kind longitudinal study conducted in 2019/2020 that followed 26 veterans experiencing homelessness in Los Angeles. The authors use the information provided by veterans about their housing, health, and service experiences to identify factors related to engaging in care and attaining stable housing.
Participants. The six children (three girls and three boys) participating in the present case study were recruited from a large longitudinal population-based study, performed at the Child Neuropsychiatric Clinic (CNC) in Gothenburg (Kantzer et al., Citation 2013, Citation 2018).The children were initially identified by a general ASD screening at age 2.5 years at the public child health-care ...
In the special issue of Qualitative Research, different researchers apply discrete approaches to make sense of narrative stability and change in a set of case-studies from the Foley Longitudinal Study (Dunlop, 2019; Fivush et al., 2019; McLean et al., 2019; Pasupathi & Wainryb, 2019; Singer, 2019). Researchers and articles with separate ...
Case studies is a way of data collection (a method) while the longitudinal studies deal with time for the data collection or it can be a way to measure one thing over and over again. Therefore, in ...
Changes in Thinking for Speaking: A Longitudinal Case Study. Gale Stam, Gale Stam [email protected] National Louis University, Department of Psychology, 5202 Old Orchard Road, Room 208, Skokie, IL, 60077-4409. Search for more papers by this author. Gale Stam, Gale Stam [email protected]
The aim of the paper is to suggest an approach to longitudinal multiple case studies. We use an example of an on-going multiple case study aiming at capturing the processes of strategizing in terms of how the networking of start-up companies interplays with their ideas of future network positions. The paper concludes by suggesting the use of a ...
This protocol proposes a case study, which aims to advance understanding of the form, content, and delivery of the pilot service. Methods: A prospective, longitudinal, mixed-methods, case study design will be used to describe the service and to explore the experiences of patients, informal carers and clinicians. Additionally, data collection ...
The course introduces the method of longitudinal case study analysis (LCA) as a hybrid of (1) process-tracing, (2) periodized within-case research design, and (3) historical comparative analysis (HCA)—combining different techniques for hypothesis testing by slicing and dicing the empirics within a single case study over time and, as a second ...
longitudinal study; case study; psychological support; Acknowledgments. The authors would like to express their gratitude for the effort put into organizing the research, goodwill, and full cooperation to the Warden of the Penitentiary Facility in Trzebinia, Lt. Col. Tomasz Wacławek.
Using a longitudinal case study on Cixing, which is a leading Chinese player in the flat knitting machine industry, this paper explores the process in which laggard firms catch up and exceed catching up to become niche champions in China. We propose a theoretical framework that illustrates the significance of contexts and response strategies for niche champions at different stages, focusing on ...
This prospective, longitudinal case-control study included 64 consecutively recruited pregnant women with T1DM, and 32 matched healthy pregnant women. Pregnant women attending the combined first-trimester screening between April 2018 and December 2022 were recruited. The general exclusion criteria were multiple pregnancies, and fetal structural ...
Objective: To train and test a super learner strategy for risk prediction of kidney failure and mortality in people with incident moderate to severe chronic kidney disease (stage G3b to G4). Design: Multinational, longitudinal, population based, cohort study. Settings: Linked population health data from Canada (training and temporal testing), and Denmark and Scotland (geographical testing).
Longitudinal qualitative studies have been designed as longitudinal at the outset and therefore have a specific focus on temporality, processes and social change. They often have an implicit theory of social change informing the analyses. Re-studies revisit the field site or community, and update or challenge the work of earlier researchers ...
China has piloted Long-Term Care Insurance (LTCI) to address increasing care demand. However, many cities neglected adjusting LTCI premiums since the pilot, risking the long-term sustainability of LTCI. Therefore, using Zhejiang Province as a case, this study simulated mortality-adjusted long-term care demand and the balance of LTCI funds through dynamic financing mechanism under diverse life ...