
An official website of the United States government
The .gov means it's official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- Browse Titles
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on the Health of Select Populations; Committee on the Evaluation of Research Management by DoD Congressionally Directed Medical Research Programs (CDMRP). Evaluation of the Congressionally Directed Medical Research Programs Review Process. Washington (DC): National Academies Press (US); 2016 Dec 19.


Evaluation of the Congressionally Directed Medical Research Programs Review Process.
- Hardcopy Version at National Academies Press
2 Overview of the Congressionally Directed Medical Research Programs
The Department of Defense's (DoD's) Congressionally Directed Medical Research Programs (CDMRP) has a well-established process for managing the review and selection of funding applications that it receives for its medical research programs. This chapter presents an overview of that process and provides a brief overview of CDMRP's organization and structure. The current functions of the program office, how it is funded, and its place within the health care hierarchy of DoD are described. The chapter also includes a brief summary of CDMPR's program processes from program initiation and goal setting through application solicitation and review to award negotiation. This chapter is intended to provide general information about CDMRP in order to set the stage for the subsequent chapters that detail the specific steps in the review process.
- THE CURRENT CDMRP
CDMRP views its role in the medical research community as a leader in advancing medical and scientific research and filling research gaps “by funding high impact, high risk and high gain projects that other agencies may not venture to fund” ( CDMRP, 2016a ). The vision and mission statements for CDMRP can be found in Box 2-1 . CDMRP currently manages 29 research programs (see Box 2-2 ), including several programs on behalf of other DoD offices, in particular, the Defense Health Agency (DHA). Each research program has its own specific vision and mission statement.
CDMRP Vision and Mission.
2016 CDMRP Research Programs.
CDMRP has emphasized that its research programs and funded applications need to be relevant to the health of service members, veterans, and their families. The committee is aware that the military health care system (TRICARE) is one of the largest health care systems in the world and cares not only for active duty and retired service members, but also for their families ( TRICARE, 2016 ). Thus, health-related issues that affect service members or their dependents would fall within the purview of DoD medical research. The scope of research performed by DoD has been a topic of debate in the U.S. Senate. In June 2016, the Senate voted that it would not put restrictions on the DoD money used for medical research so that it may continue to benefit military members and their families and also the general public ( Tritten, 2016 ).
CDMRP is located within the U.S. Army Medical Research and Materiel Command (USAMRMC), headquartered at Fort Detrick, Maryland (see Figure 2-1 ). The USAMRMC established the CDMRP program office in response to congressional funding for research initiatives; it decides how CDMRP is staffed and how it functions. Although CDMRP is based within the Department of the Army, the program office also has involvement from both the Department of the Navy and the Department of the Air Force. Over the years, CDMRP leadership has come from all three branches, with representatives from each service having served as CDMRP director.
CDMRP organizational chart. NOTE: DHA = Defense Health Agency; RDA = Research, Development, and Acquisition; USAMRAA = U.S. Army Medical Research Acquisition Activity. SOURCE: Adapted from Salzer, 2016d.
As noted in Box 2-2 , CDMRP provides management support for several research programs on behalf of the DHA's Research, Development, and Acquisition Directorate. DHA receives core funds 1 from Congress for these research programs, which have a strong military focus. Each of those programs is aligned with one or more joint program committees (JPCs), but the level of involvement in a program is at the discretion of the JPC. JPC membership consists of both DoD and non-DoD medical and military technical experts and representatives from the Department of Veterans Affairs and the Department of Health and Human Services. The largest DHA research program for which CDMRP provides management support is the Defense Medical Research and Development Program (DMRDP), which is overseen by the following six 2 JPCs:
- medical training and health information services (JPC-1),
- military infectious diseases (JPC-2),
- military operational medicine (JPC-5),
- combat casualty care (JPC-6),
- radiation health effects (JPC-7), and
- clinical and rehabilitative medicine (JPC-8).
JPCs support DMRDP and other CDMRP programs with a strong active-duty military focus by providing guidance, through programmatic review of applications and by making funding recommendations ( Resnik et al., 2013 ). CDMRP states that JPCs also engage in strategic planning activities that may feed into the CDMRP vision setting process ( Salzer, 2016a ). CDMRP staff and contractors work closely with the JPCs to provide program and award management support for JPC research initiatives ( CDMRP, 2016b ).
Although all CDMRP research programs are aligned with at least one JPC, programs that do not have a strong military health focus such as the Breast Cancer Research Program, the Autism Research Program, and the Parkinson's Research Program do not necessarily have substantial input from the affiliated JPC. The strongly JPC-aligned programs are an integral part of CDMRP, but they require different chain-of-command procedures and approvals from those that CDMRP generally uses to manage its other research programs ( Salzer, 2016a ; Santullo, 2016 ).
- CDMRP FUNDING
Funding for CDMRP research programs is appropriated on an annual basis. Congress, in response to advocacy groups and other interested parties, selects which programs will be funded and at what level each year. Language in the appropriations bills can range from very specific instructions on how to spend the money for a program to quite vague statements or just the line item; this can result in considerable variation in program funding and focus. Figure 2-2 provides an example of line items for CDMRP research programs as well as an example of accompanying congressional language from the Department of Defense Appropriations Act, 2016.
Examples of language in the Department of Defense Appropriations Act, 2016, funding CDMRP programs: (A) excerpt of sample line items in the budget; (B) text to note specific instructions for the Peer Reviewed Cancer Research Programs. SOURCE: Senate Report (more...)
Although appropriations for individual research programs (and thus CDMRP) in general can (and occasionally do) vary from year-to-year, in most cases funding for the individual programs has stayed relatively consistent since their inception; however, a few programs have been discontinued because of a lack of congressional funding (e.g., defense women's health, osteoporosis, genetic studies of food allergies). Table 2-1 shows the funding history for each program and the number of programs funded by year, and Figure 2-3 summarizes the growth of CDMRP since 1992. Funding for CDMRP as a whole increased by $433.3 million in 2014 from $557.7 million to $991.0 million, and increased again in 2015 by $33.4 million to a total of $1.024 billion. The initial program, the Breast Cancer Research Program, has been funded since 1992 for a total of more than $3 billion, and the Prostate Cancer Research Program (begun in 1997) and the Peer Reviewed Medical Research Program (begun in 1999) have both received more than $1 billion. The Psychological Health/Traumatic Brain Injury Research Program, a program that the CDRMP administers on behalf of three JPCs, is the fourth largest program at just over $800 million, and has been funded for the past 8 years.
CDMRP Funding History (in Millions) for Each Program by Year.
The growth of CDMRP programs and funding since 1992 as shown in Table 2-1.
- OVERVIEW OF THE CDMRP REVIEW PROCESS
All CDMRP research programs follow the same general multi-step process for soliciting, reviewing, and making funding decisions for applications (see Figure 2-4 ). These steps are conducted by two panels: the programmatic panel and the peer review panel. The application review cycle (the left side of Figure 2-4 in blue) spans approximately 12 months, beginning with the annual congressional appropriation of funds and ending with a list of funding recommendations being submitted to USAMRMC for approval. Award negotiation and implementation may take an additional year.
The CDMRP review process. Note that the programmatic panel conducts several steps in the review process: vision setting (Step 1; see Chapter 4); the development of the investment strategy, which results in the release of program announcements (Step 2; (more...)
After CDMRP receives its appropriations, it has 2 years by law to obligate the money; thus, each CDMRP award is fully funded up front. However, even though each award is fully funded, principal investigators do not necessarily receive all their funding at once; rather, milestones are established and must be met for the release of further funds. Program announcements (see Chapter 4 ) specify the maximum length of the award over which money may be allocated; the length of the award may not exceed 5 years ( IOM, 2004 ).
The second part of the process is the award management cycle (the right side of Figure 2-4 in red), in which recommended awards are selected and approved for funding, negotiations are undertaken to finalize the awards, and the progress of the awards is then monitored from initiation through to closeout. In this report, the committee evaluates the CDMRP review process only up to the point of the funding recommendations (Step 5).
The five major steps in the application review process considered by the committee (in yellow in Figure 2-4 ) are as follows ( CDMRP, 2015a ):
Vision Setting ( Chapter 4 ): When the congressional appropriation process is complete, CDMRP receives funds for each research program.
For existing programs, the first step in the process is the vision setting meeting held by the programmatic panel. Vision setting occurs in months 1–4 of the program cycle to identify research gaps and to define an investment strategy for that year (that is, to choose award mechanisms and topics) to address those gaps. The annual investment strategy identifies the award mechanisms to be used for each research program; the award mechanisms result in program announcements that drive the application process.
If the appropriation is for a new research program, a one-time stakeholders meeting is held before the first vision setting meeting to help scope out the Congressional intent for the program as well as research needs.
Program Announcement Release ( Chapter 4 ): Following the vision setting meeting, a program announcement for each award mechanism is developed by the CDMRP program manager and released by the CDMRP contracting office within 2–5 months of the meeting. In some cases, a pre-announcement will be released to alert interested parties to an upcoming program announcement. Interested researchers can sign up to be electronically notified when new program announcements are released or can find the program announcements online. Program announcements notify the research community that new funding opportunities are available for that program and delineate the information that must be submitted to CDMRP for each application.
The electronic biomedical research application portal, eBRAP, is used for a variety of program activities, including application submission, notification of availability of program announcements, and communications with applicants. Although government owned, it is maintained by the peer review contractor.
Pre-Application Screening, Review, and Invitation to Submit Full Application ( Chapter 4 ): Applications must be submitted individually in response to a specific program announcement; no other applications are accepted. Most programs use a pre-application step to reduce the number of full applications to be reviewed. Pre-application submission requirements and screening criteria are specified in the program announcement. Some program announcements for specific award mechanisms, such as the Clinical Consortium Research Site Award, use letters of intent as the pre-application and do not have screening criteria. Pre-applications are typically submitted and screened by the programmatic panel during months 5–8. Applications that meet the pre-application screening criteria, as determined by the programmatic panel, are then invited to submit a full application.
Peer Review ( Chapter 5 ): Between months 7 and 11, full applications are received and undergo review for scientific and technical merit by the peer review panel; this represents the first tier of CDMRP's two-tier review process. The results of the peer review (both numeric scores and narrative summaries) are submitted to the programmatic panel.
Programmatic Review ( Chapter 6 ): Following peer review, applications are reviewed by the same programmatic panel as in steps 1 and 3 to determine programmatic relevance and portfolio balance, in addition to considering the scores and summaries from peer review. Programmatic review (months 9–14) serves as the second tier of the two-tier review process and results in a list of applications that are recommended for funding, along with a list of alternate applications that may be considered for funding if sufficient funds become available.
The committee notes that CDMRP established an Inquiry Review Panel to address questions and appeals by applicants regarding either peer or programmatic review of their applications. The committee was informed that less than 0.5% of applications have re-review requests (Colonel Wanda Salzer, CDMRP director, personal communication, October 16, 2015).
Once the list of funding recommendations has been completed, it must be approved or concurred with by the commanding general, USAMRMC, and/or the DHA's Research, Development and Acquisition Directorate.
Awards that have been approved for funding move into the award-management phase (the right side of Figure 2-4 in red). Award management begins with award negotiations, which can take more than 1 year to complete (months 11–24). Finally, once an award is in place, it is actively managed and monitored by CDMRP throughout its duration. Award management includes, but is not limited to, progress reports from the research institution and financial reporting. When an award's end date approaches, preparations are made to close the award, and the closure is finalized approximately 6 months after the period of performance has expired.
Core funds are part of the annual DoD budget set by Congress and the president (known as the President's Budget). The CDMRP appropriations are not considered to be DoD core funds.
There is no JPC-3 or JPC-4 committee.
- Cite this Page National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on the Health of Select Populations; Committee on the Evaluation of Research Management by DoD Congressionally Directed Medical Research Programs (CDMRP). Evaluation of the Congressionally Directed Medical Research Programs Review Process. Washington (DC): National Academies Press (US); 2016 Dec 19. 2, Overview of the Congressionally Directed Medical Research Programs.
- PDF version of this title (3.3M)
In this Page
Recent activity.
- Overview of the Congressionally Directed Medical Research Programs - Evaluation ... Overview of the Congressionally Directed Medical Research Programs - Evaluation of the Congressionally Directed Medical Research Programs Review Process
Your browsing activity is empty.
Activity recording is turned off.
Turn recording back on
Connect with NLM
National Library of Medicine 8600 Rockville Pike Bethesda, MD 20894
Web Policies FOIA HHS Vulnerability Disclosure
Help Accessibility Careers
Department of Defense Congressionally Directed Medical Research Programs
Dod search tools & resources, research programs.
Breast Cancer Research Program (March Pre-app deadlines)
Peer Reviewed Medical Research Program (March/April Pre-app deadlines)
Amyotrophic Lateral Sclerosis Research Program (April Pre-app deadlines)
Ovarian Cancer Research Program (April/May Pre-app deadlines)
Autism Research Program (April Pre-app deadlines)
Epilepsy Research Program (May Pre-app deadlines)
Lung Cancer Research Program (May/July Pre-app deadlines)
Peer Reviewed Alzheimer's Research Program (May Pre-app deadlines)
Spinal Cord Injury Research Program (May Pre-app deadlines)
Tick-Borne Disease Research Program (May Pre-app deadlines)
Military Burn Research Program (May Pre-app deadlines)
Peer Reviewed Cancer Research Program (May/July Pre-app deadlines)
Tuberous Sclerosis Complex Research Program (June Pre-app deadlines)
Orthotics and Prosthetics Outcomes Research Program (June Pre-app deadlines)
Traumatic Brain Injury and Psychological Health Research Program (June Pre-app deadlines)
Joint Warfighter Medical Research Program (June Pre-app deadline)
Peer Reviewed Orthopaedic Research Program (June Pre-app deadlines)
Bone Marrow Failure Research Program (June Pre-app deadlines)
Rare Cancers Research Program (June/July Pre-app deadlines)
Multiple Sclerosis Research Program (June/July Pre-app deadlines)
Prostate Cancer Research Program (June/August Pre-app deadlines)
Lupus Research Program (July Pre-app deadlines)
Parkinson's Research Program (July Pre-app deadlines)
Reconstructive Transplant Research Program (July Pre-app deadlines)
Pancreatic Cancer Research Program (July/September Pre-app deadlines)
Combat Readiness-Medical Research Program (July Pre-app deadlines)
Vision Research Program (July/August Pre-app deadlines)
Melanoma Research Program (July/August Pre-app deadlines)
Kidney Cancer Research Program (July/September Pre-app deadlines)
Hearing Restoration Research Program (August Pre-app deadline)
Neurofibromatosis Research Program (August Pre-app deadlines)
Duchenne Muscular Dystrophy Research Program (August Pre-app deadlines)
Combat Casualty Care Research Program (August Pre-app deadline)
Chronic Pain Management Research Program (August Pre-app deadline)
Toxic Exposures Research Program (September Pre-app deadlines)
More programs to be posted soon. The most up to date information may be found on the DoD Funding Opportunities webpage.
Funding Opportunity: DOD CDMRP Releases FY 2024 Peer Reviewed Medical Research Program Solicitations
Lewis-Burke Associates has provided campus with a report about the Department of Defense (DOD) Congressionally Directed Medical Research Programs (CDMRP) FY24 Peer Reviewed Medical Research Program (PRMRP) solicitations. For FY 2024, Congress has allocated $370 million for PRMRP in over forty topic areas. The PRMRP aims to support medical research projects of clear scientific merit that lead to clear and impactful advances in the health care of service members, veterans, and beneficiaries. Those interested should carefully review the submission requirements for each funding mechanism and the “Strategic Goals” of each FY 2024 PRMRP topic area in each solicitation.
Department of Defense Medical Research Office

Mayo Clinic researchers work closely with the Department of Defense and military leadership, contributing significantly to the medical and technological support of active duty personnel, veterans and wounded warriors.
The Department of Defense Medical Research Office links Mayo Clinic researchers to the medical research needs of the U.S. Department of Defense (DOD) and its service branches. The relationship harnesses Mayo Clinic's wide-ranging expertise and the dynamic application of health-related innovation and technology.
The Medical Research Office helps advance specialized research by securing new and ongoing funding, fostering relationships, and identifying new defense medical research opportunities.
Working in concert with the Military Medicine Program at Mayo Clinic, the Medical Research Office promotes the multidisciplinary strength of Mayo Clinic's faculty and its collaborative history with the Department of Defense.
Strategically, the Department of Defense Medical Research Office oversees Mayo Clinic's diverse portfolio of DOD -funded research. It serves as a liaison for Mayo Clinic researchers to present their interests and introduce innovative ideas for special projects across the spectrum of DOD medical research objectives.
Dozens of Mayo Clinic researchers receive funding for special projects that are advancing areas of national health, sustainability, security and education by developing new technologies and solutions.
The main liaison of the Medical Research Office is the Mayo Clinic Strategic Funding Office for Research. The goal of the Strategic Funding Office for Research is to link the research needs of the DOD with Mayo Clinic research interests and secure funding for research and development.
Through new applications of advanced science and medicine, Mayo Clinic researchers have produced hundreds of solutions to address challenges faced by the Department of Defense in keeping the U.S. military operating efficiently and safely. DOD research entities include the Office of Naval Research, the Army Research Office and the Air Force Office of Scientific Research.
The Department of Defense Medical Research Office evolved from a long and successful partnership with the U.S. government. Numerous Mayo Clinic faculty and staff have been or are members of the U.S. military. The cornerstone of Mayo Clinic's rich heritage and commitment to military service can be traced back to the earliest days of Mayo Clinic history, starting with Dr. William Worrall Mayo's service to the U.S. Army and his medical contributions during the Civil War. This tradition of service is part of Mayo Clinic's strategic makeup and core beliefs and continues today through Mayo Clinic's efforts directly related to training, supporting and healing members of the military.
Contact us if you need more information about research conducted by physicians and scientists related to the Department of Defense or military medicine.
Focus Areas
Research spans a wide range of disciplines, including aerospace medicine, biomechanics, amputation, traumatic brain injury and vaccines.
More about research at Mayo Clinic
- Research Faculty
- Laboratories
- Core Facilities
- Centers & Programs
- Departments & Divisions
- Clinical Trials
- Institutional Review Board
- Postdoctoral Fellowships
- Training Grant Programs
- Publications
Mayo Clinic Footer
- Request Appointment
- About Mayo Clinic
- About This Site
Legal Conditions and Terms
- Terms and Conditions
- Privacy Policy
- Notice of Privacy Practices
- Notice of Nondiscrimination
- Manage Cookies
Advertising
Mayo Clinic is a nonprofit organization and proceeds from Web advertising help support our mission. Mayo Clinic does not endorse any of the third party products and services advertised.
- Advertising and sponsorship policy
- Advertising and sponsorship opportunities
Reprint Permissions
A single copy of these materials may be reprinted for noncommercial personal use only. "Mayo," "Mayo Clinic," "MayoClinic.org," "Mayo Clinic Healthy Living," and the triple-shield Mayo Clinic logo are trademarks of Mayo Foundation for Medical Education and Research.
Florida State University
FSU | University Announcements
University Announcements
U.s. department of defense funding for health research.

Beth Hodges, Director of FSU Research Development
Registration is now open for the Congressionally Directed Medical Research Programs (CDMRP) workshop on Jan. 22!
The Deputy Director and Program Managers from the U.S. Department of Defense will present an overview of CDMRP, cover specific programs upcoming in FY2024, and provide guidance on application submissions.
Of note, research does not need to be conducted in military populations and faculty interested in basic and translational medical research on a variety of health conditions are encouraged to attend.
This workshop is co-sponsored by FSU Research Development and FSU Health.
Register today !
- National Eye Institute
Defense-Related Research Funding
Welcome to NAEVR's Defense research Advocacy Center, where you can access our position on Fiscal Year (FY) 2024 federal funding for Department of Defense medical research programs , view recent Legislative Updates, view summaries of past AEVR-sponsored Congressional Briefings on Capitol Hill (featuring DOD-sponsored research) and read about the NAEVR advocacy and AEVR educational activities in the Contributor Reports .
To learn more about the range of medical research programs managed by the Department of Defense or to search through the abstract database, click here .
Department of Defense Vision Research Program
House appropriations committee approves fiscal year 2024 department of defense appropriations bill with $20 m for vision research program.
06/22/2023 - On June 22 the House Appropriations Committee approved its Fiscal Year (FY) 2024 Defense spending bill which includes $20 million funding for the Department of Defense's (DOD) Vision Research Program… Read More
NAEVR Defense Funding Session Features DOD Vision Program Manager, Insights into the FY2023 Program Announcement
05/01/2023 - VRP Program Manager Tian Wang, PhD, addresses the audience NAEVR’s April 24 Defense-Related Vision Research Opportunities session at the ARVO Annual Meeting in New Orlean… Read More
NAEVR Attends 8th Military Vision Symposium on Innovation and Unmet Needs for Ocular Injury
03/06/2023 - The Military Vision Symposium Speakers The National Alliance for Eye and Vision Research (NAEVR) was pleased to support and participate in the Military Vision Symposium o… Read More
Congress Passes, President Signs Fiscal Year 2023 Omnibus
01/03/2023 - On December 29, President Biden signed the Consolidated Appropriations Act of 2023, a $1.7 trillion Omnibus Fiscal Year (FY) 2023 Appropriations bill which combined all FY2023 spending bills into one… Read More
House Appropriations Committee Approves Fiscal Year 2023 Department of Defense Appropriations Bill with $20 M for Vision Research Program
06/23/2022 - On June 22 the House Appropriations Committee approved its Fiscal Year (FY) 2023 Defense spending bill which includes $20 million in VRP funding, the fifth year that the program has been funded at th… Read More
NAEVR Hosts Defense Research Funding Session at ARVO Annual Meeting
05/12/2022 - VRP Program Manager Tian Wang, PhD, speaks to the audience Click here to watch the video. For the first time since the start of the pandemic, the NAEVR Defen… Read More
NAEVR and ARVO Host Defense Research Funding Opportunities Webinar
06/04/2021 - CDMRP Vision Program Manager Tian Wang, PhD On June 2 NAEVR, along with the Association for Research in Vision and Ophthalmology (ARVO), held a special Defense Research Fundi… Read More
DOD Vision Research Program Releases FY2021 Program Announcements
05/17/2021 - On May 14, the Department of Defense’s (DOD) Vision Research Program (VRP) released its Fiscal Year (FY) 2021 Program Announcements, with $20 million available for research. This year marks the third… Read More
View Defense-Related Research Funding Archive
Department of Defense: Lupus Research Program
Providing more than $86 million for high-impact research on lupus.
The Lupus Foundation of America led the fight to secure lupus research funding through the Department of Defense’s (DoD) Congressionally Directed Medical Research Program (CDMRP). To date, our efforts have generated more than $86 million to fund high-impact, high-quality research to identify ways to more effectively diagnose and treat lupus.
Just over a year after our advocacy efforts began in 2003, Congress first included lupus as an area eligible for funding through the Department of Defense’s Peer Reviewed Medical Research Program (PRMRP). The PRMRP is a sub-program of the CDMRP that provides grants to researchers around the world on topics determined each year by Congress.
Between 2005 and 2016, thanks to the ongoing outreach of lupus advocates, Congress included lupus in the PRMRP. The program allocated more than $21 million to 22 different lupus research studies looking into every aspect of diagnosing and treating the disease.
Throughout this period, we continued to build the case for a research program dedicated specifically to lupus at the DoD. Such a program would mean more opportunities to fund lupus research that would benefit not only military personnel, but everyone with lupus.
In May 2017, Congress responded to our advocacy by creating the Lupus Research Program and providing it with $5 million.
Today, the Lupus Research Program is funding promising research by some of the most well-known, accomplished researchers in the world. Congress continues to recognize the importance of this program and has already provided it with $45 million. Supported by our advocates at every step of the way, this is the story of how we got here.
Research Funded by the Lupus Research Program
- 2022 (fiscal year 2021 funding)
- 2021 (fiscal year 2020 funding)
- 2020 (fiscal year 2019 funding)
- 2019 (fiscal year 2018 funding)
- 2018 (fiscal year 2017 funding)
2009: CEO Sandra C. Raymond testified before the Senate Defense Subcommittee on the need for lupus research at DoD.
2009: We authored and released Lupus and the Military, which explored the connection between America’s soldiers and lupus.
2010: Foundation representatives met with CDMRP officials at Ft. Detrick to discuss a lupus-specific research program at the DoD.
2012: We led the creation of the Caucus, which would come to champion the Lupus Research Program.
2016: We worked with the Caucus to circulate a Dear Colleague letter, showing broad support for lupus-specific research at the DoD.
2017: President Trump signed legislation creating the Lupus Research Program and funding it with $5 million in its first year.
Why is the Department of Defense supporting lupus research?
Congress established the CDMRP in 1992 because it recognized that maintaining and promoting the health of Department of Defense personnel was essential to the country’s national security. Any disease or condition that affects the American public will also affect the military, making medical research a priority for the Pentagon.
With the U.S. military more diverse than it has ever been, both in gender and in race, lupus will increasingly affect its members. Of the more than 1.5 million Americans living with lupus, it is estimated that 9 in 10 are women, and the disease is 2 to 3 times more common among women of color. Minority women tend to develop lupus at a younger age, experience more serious complications, and are more likely to die from the disease.
In 2016, women represented 16% of all active duty service members, and 56% of those women were minorities. As the military becomes more diverse, more of their personnel will be affected by lupus.
People in the military are exposed to several factors that are associated with the development of lupus and other autoimmune diseases, including post-traumatic stress disorder (PTSD), chemicals and toxins, ultraviolet (UV) light, and certain drugs and infectious agents. Research funded by the Lupus Research Program will study these triggers and try to determine what effect they have on the immune system.
Read our full 2009 report on lupus and the military .
How our advocacy supports the Lupus Research Program
Congressional funding is not keeping pace with current needs: in the Lupus Research Program’s first three years, for example, the DoD was able to fund only 38 of the 334 (less than 12%) high-quality applications they received.
Congress must appropriate funding for the Lupus Research Program every year. Because priorities can shift, it’s important to have advocates who are willing to tell their members of Congress how important this program is to people with lupus and their loved ones and why it deserves increased funding.
Sign up to become an advocate , and we’ll let you know when your outreach in support of the Lupus Research Program can make an impact.
If you have lupus and served in the military, tell us your story ! Your story will help us show Congress how lupus affects our military and that more must be done to understand the disease and accelerate the search for new treatments.
Get resources, news, ways to get involved and MORE.
There are multiple chapters near you. Select your preferred chapter.
Supporting lupus patients and advocates in Arizona.
Serving the District of Columbia, Maryland, and Northern Virginia.
Serving southern Illinois up to and including Springfield, Kansas, and Missouri
Serving north, central and west Texas, including Dallas/Fort Worth, San Antonio, Austin, El Paso, Lubbock, and surrounding areas
Serving northern and central Illinois, Indiana, Iowa, Michigan, and Minnesota
Serving Connecticut, Massachusetts, Maine, New Hampshire, northern and central New Jersey, New York, Rhode Island, and Vermont
Serving Pennsylvania, Delaware and Southern New Jersey
Serving Houston, Beaumont, Corpus Christi, Harlingen and surrounding areas in Texas
There are multiple walks near you.
This website uses cookies to ensure you get the best experience. Learn more
N-acetylcysteine as a treatment for substance use cravings: A meta-analysis
- Find this author on Google Scholar
- Find this author on PubMed
- Search for this author on this site
- ORCID record for Emma L Winterlind
- ORCID record for Samantha G Malone
- ORCID record for Michael R Setzer
- ORCID record for Mikela A Murphy
- For correspondence: [email protected]
- Info/History
- Preview PDF
N-acetylcysteine (NAC) may serve as a novel pharmacotherapy for substance use and substance craving in individuals with substance use disorders (SUDs), possibly through its potential to regulate glutamate. Though prior meta-analyses generally support NACs efficacy in reducing symptoms of craving, individual trials have found mixed results. The aims of the this updated meta-analysis were to (1) examine the efficacy of NAC in treating symptoms of craving in individuals with a SUD and (2) explore subgroup differences, risk of bias, and publication bias across trials. Database searches of PubMed, Cochrane Library, and ClinicalTrials.gov were conducted to identify relevant randomized control trials (RCTs). The meta-analysis consisted of 9 trials which analyzed data from a total of 623 participants. The most targeted substance in the clinical trials was alcohol (3/9; 33.3%), followed by tobacco (2/9; 22.2%) and multiple substances (2/9; 22.2%). Meta-analysis, subgroup analyses, and leave-one-out analyses were conducted to examine treatment effect on craving symptoms and adverse events. Risk of bias assessments, Eggers tests, and funnel plot tests were conducted to examine risk of bias and publication bias. NAC did not significantly outperform placebo in reducing symptoms of craving in the meta-analysis (SMD = 0.189, 95% CI = -0.015 - 0.393). Heterogeneity was very high in the meta-analysis (99.26%), indicating that findings may have been influenced by clinical or methodological differences in the study protocols. Additionally, results indicate that there may be publication bias present. There were no between-group differences in risk of AEs. Overall, our findings are contrary to those of prior meta-analyses, suggesting limited impact of NAC on substance craving. However, the high heterogeneity and presence of publication bias identified warrants cautious interpretation of the meta-analytic outcomes.
Competing Interest Statement
The authors have declared no competing interest.
Funding Statement
This work was supported by funding from the National Institute on Alcohol Abuse and Alcoholism (R01-AA030041) and the Department of Defense (HU0001-22-2-0066).
Author Declarations
I confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been obtained.
The details of the IRB/oversight body that provided approval or exemption for the research described are given below:
The meta-analysis used only openly available data that were originally presented by trial authors of each trial included in the meta-analysis. One study (Roten et al., 2013) did not include follow-up data in their publication but provided it upon request. DOIs/ClinicalTrial ID of included trials: Schmaal et al., 2011: https://doi.org/10.1159/000327682 Yoon, 2013: NCT00568087 Roten et al., 2013: https://doi.org/10.1016/j.addbeh.2012.11.003 Back et al., 2016: https://doi.org/10.4088/JCP.15m10239 Schulte et al., 2017: https://doi.org/10.1177/0269881117730660 Back, 2021: NCT02911285 McKetin et al., 2021: https://doi.org/10.1016/j.eclinm.2021.101005 Back, 2023: NCT02966873 Morley et al., 2023: https://doi.org/10.1093/alcalc/agad044
I confirm that all necessary patient/participant consent has been obtained and the appropriate institutional forms have been archived, and that any patient/participant/sample identifiers included were not known to anyone (e.g., hospital staff, patients or participants themselves) outside the research group so cannot be used to identify individuals.
I understand that all clinical trials and any other prospective interventional studies must be registered with an ICMJE-approved registry, such as ClinicalTrials.gov. I confirm that any such study reported in the manuscript has been registered and the trial registration ID is provided (note: if posting a prospective study registered retrospectively, please provide a statement in the trial ID field explaining why the study was not registered in advance).
I have followed all appropriate research reporting guidelines, such as any relevant EQUATOR Network research reporting checklist(s) and other pertinent material, if applicable.
Data Availability
The R code used to conduct analyses and create forest and funnel plots can be accessed using this link: https://github.com/ewinterli/NAC-meta-analysis
https://github.com/ewinterli/NAC-meta-analysis
View the discussion thread.
Thank you for your interest in spreading the word about medRxiv.
NOTE: Your email address is requested solely to identify you as the sender of this article.

Citation Manager Formats
- EndNote (tagged)
- EndNote 8 (xml)
- RefWorks Tagged
- Ref Manager
- Tweet Widget
- Facebook Like
- Google Plus One
- Addiction Medicine (323)
- Allergy and Immunology (627)
- Anesthesia (163)
- Cardiovascular Medicine (2363)
- Dentistry and Oral Medicine (287)
- Dermatology (206)
- Emergency Medicine (378)
- Endocrinology (including Diabetes Mellitus and Metabolic Disease) (833)
- Epidemiology (11755)
- Forensic Medicine (10)
- Gastroenterology (701)
- Genetic and Genomic Medicine (3722)
- Geriatric Medicine (348)
- Health Economics (632)
- Health Informatics (2388)
- Health Policy (929)
- Health Systems and Quality Improvement (894)
- Hematology (340)
- HIV/AIDS (780)
- Infectious Diseases (except HIV/AIDS) (13298)
- Intensive Care and Critical Care Medicine (767)
- Medical Education (365)
- Medical Ethics (104)
- Nephrology (398)
- Neurology (3483)
- Nursing (197)
- Nutrition (522)
- Obstetrics and Gynecology (672)
- Occupational and Environmental Health (661)
- Oncology (1818)
- Ophthalmology (535)
- Orthopedics (218)
- Otolaryngology (286)
- Pain Medicine (232)
- Palliative Medicine (66)
- Pathology (445)
- Pediatrics (1030)
- Pharmacology and Therapeutics (426)
- Primary Care Research (418)
- Psychiatry and Clinical Psychology (3169)
- Public and Global Health (6128)
- Radiology and Imaging (1275)
- Rehabilitation Medicine and Physical Therapy (743)
- Respiratory Medicine (825)
- Rheumatology (379)
- Sexual and Reproductive Health (372)
- Sports Medicine (322)
- Surgery (400)
- Toxicology (50)
- Transplantation (172)
- Urology (145)
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- My Account Login
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Open access
- Published: 09 May 2024
Population health implications of exposure to pervasive military aircraft noise pollution
- Giordano Jacuzzi ORCID: orcid.org/0009-0005-4351-5682 1 ,
- Lauren M. Kuehne ORCID: orcid.org/0000-0002-0054-613X 2 ,
- Anne Harvey 3 ,
- Christine Hurley 3 ,
- Robert Wilbur 4 ,
- Edmund Seto ORCID: orcid.org/0000-0003-4058-0313 5 &
- Julian D. Olden ORCID: orcid.org/0000-0003-2143-1187 1
Journal of Exposure Science & Environmental Epidemiology ( 2024 ) Cite this article
545 Accesses
71 Altmetric
Metrics details
While the adverse health effects of civil aircraft noise are relatively well studied, impacts associated with more intense and intermittent noise from military aviation have been rarely assessed. In recent years, increased training at Naval Air Station Whidbey Island, USA has raised concerns regarding the public health and well-being implications of noise from military aviation.
This study assessed the public health risks of military aircraft noise by developing a systematic workflow that uses acoustic and aircraft operations data to map noise exposure and predict health outcomes at the population scale.
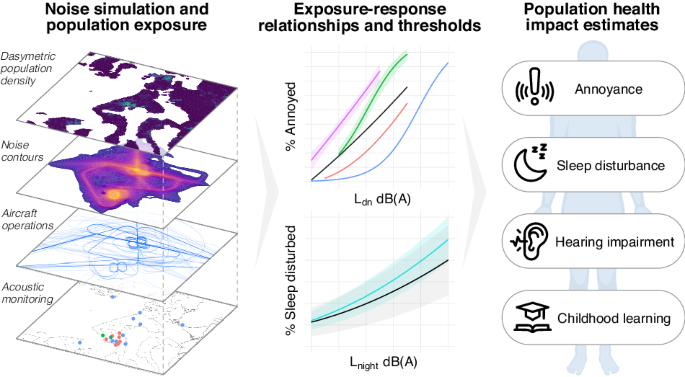
Acoustic data encompassing seven years of monitoring efforts were integrated with flight operations data for 2020–2021 and a Department of Defense noise simulation model to characterize the noise regime. The model produced contours for day-night, nighttime, and 24-h average levels, which were validated by field monitoring and mapped to yield the estimated noise burden. Established thresholds and exposure-response relationships were used to predict the population subject to potential noise-related health effects, including annoyance, sleep disturbance, hearing impairment, and delays in childhood learning.
Over 74,000 people within the area of aircraft noise exposure were at risk of adverse health effects. Of those exposed, substantial numbers were estimated to be highly annoyed and highly sleep disturbed, and several schools were exposed to levels that place them at risk of delay in childhood learning. Noise in some areas exceeded thresholds established by federal regulations for public health, residential land use and noise mitigation action, as well as the ranges of established exposure-response relationships.
Impact statement
This study quantified the extensive spatial scale and population health burden of noise from military aviation. We employed a novel GIS-based workflow for relating mapped distributions of aircraft noise exposure to a suite of public health outcomes by integrating acoustic monitoring and simulation data with a dasymetric population density map. This approach enables the evaluation of population health impacts due to past, current, and future proposed military operations. Moreover, it can be modified for application to other environmental noise sources and offers an improved open-source tool to assess the population health implications of environmental noise exposure, inform at-risk communities, and guide efforts in noise mitigation and policy governing noise legislation, urban planning, and land use.
Similar content being viewed by others

Underwater acoustic analysis reveals unique pressure signals associated with aircraft crashes in the sea: revisiting MH370

Bayesian statistics and modelling

Ambient carbon dioxide concentration correlates with SARS-CoV-2 aerostability and infection risk
Introduction.
The adverse effects of noise pollution, or unwanted or disturbing sound, on human physical and psychological health are widely recognized. Documented impacts range from annoyance and stress to elevated risk of sleep disturbance, cardiovascular disease, hearing impairment, and compromised childhood learning [ 1 , 2 , 3 , 4 , 5 ]. Recognition of these impacts and their associated costs to public health have highlighted the problem of increasing environmental noise originating from diverse human activities [ 6 , 7 ]. Of these, noise from pervasive aviation is a primary and growing cause of concern internationally and has been reported to elicit more severe health impacts than other sources of transportation noise [ 8 , 9 , 10 ].
The ability to assess the health consequences of aircraft noise is fundamental to inform affected communities about risks, devise strategies to mitigate impacts, and guide policy to protect or restore public health. In recent decades, growing scientific inquiry has led to the development of quantitative exposure-response relationships that directly link aircraft noise exposure with estimated population health outcomes [ 9 , 11 , 12 ]. However, while policies enacted in a handful of regions (e.g., European Noise Directive, Environmental Quality Standards for Noise) have improved the assessment of environmental noise exposure and health impacts, regulatory actions to reduce noise pollution and/or mitigate exposures have largely been slow and irregular [ 13 , 14 , 15 , 16 ]. Furthermore, compared to research in civil aviation noise (i.e., commercial and private aircraft), studies concerned with the health implications of noise from military aviation specifically have faced unique challenges (e.g., intermittent or unpublished operations, a lack of data to inform exposure-response relationships) that have limited the scale and scope of data available to assess population health risks [ 17 , 18 , 19 ].
Noise regimes of military aviation differ dramatically in their level, spectra, repetition, and character [ 17 , 18 , 20 , 21 , 22 , 23 ]. Unlike commercial aircraft noise, which is consistent and largely predictable in the frequency of events and duration of exposure, noise from military activity can vary widely over time. Military air bases are ubiquitous around the world, and a small but growing body of research has begun to investigate the unique human health implications of military aircraft noise exposure. For example, noise from military aviation can elicit different, and often greater, impacts on human disturbance and health compared to civil aviation [ 19 , 24 , 25 ]. These studies remain in the minority, leading to insufficient understanding to inform impacted communities and guide specialized policy [ 7 ]. Furthermore, military airfields and air spaces may often be exempted from or subject to differing regulations for noise assessment and mitigation [ 26 , 27 ], leading to a policy or regulatory vacuum whereby communities must petition for such actions. For example, although federal policy allows compensation for sound insulation in high exposure areas around civilian airports in the US, this policy applies only to “public use airports” [ 27 ]. While the spatiotemporal extent of operations and noise exposure from American civilian transportation is readily available (e.g., US National Transportation Noise Map [ 28 ]), corresponding data on how military aircraft operations are the source of noise permeating across space and time is reported much less often to the public.
In recent years, public concern has grown regarding noise experienced by communities in Washington State, USA, from military training activities at Naval Air Station Whidbey Island (NASWI) [ 29 ]. Since the US Navy consolidated its fleet of EA-18G Growler aircraft at NASWI and expanded flight operations in 2013, noise exposures have grown dramatically for residents of multiple counties [ 17 , 18 ]. An environmental impact statement was conducted in accordance with the National Environmental Protection Act, which provided evidence for community annoyance, speech and classroom interference, as well as an increase in the probability of awakening and the population vulnerable to potential hearing loss due to military aircraft noise events [ 30 ]. However, the assessment of population health impacts has consistently come under scrutiny, and as early as 2017 the Washington State Board of Health concluded that available data was insufficient to assess the impacts of a proposed operational increase, and a full public health risk assessment was needed [ 31 ]. This was supported by a subsequent review that found that operations around NASWI largely exceeded those of all health-related studies of military low-elevation flights worldwide [ 17 ]. A lawsuit jointly filed by a citizens group and Washington State in 2019 ultimately resulted in a 2022 ruling that the Navy did not adequately consider ramifications for childhood learning, and a subsequent order to reconduct the environmental impact statement [ 32 ].
The present study sought to address this knowledge gap by conducting a transparent and reproducible quantitative assessment of military aviation noise and its implications for public health and well-being at a regional scale. Employing a novel workflow for evaluating the human health impacts of noise pollution, we quantify the sonic character and spatiotemporal distribution of aircraft noise exposure by integrating acoustic monitoring and simulations of aircraft activity with a population density map to ultimately derive a suite of population health outcomes, including estimates of annoyance, sleep disturbance, hearing impairment, and compromised childhood learning throughout the study region. This research was guided by input from community partners, and public webinars reported routinely on progress and outcomes throughout the entire study period. Results from this study provide evidence for the pervasive noise pollution, and resulting public health implications, stemming from military aviation at NASWI. More broadly, it provides a workflow to systematically assess the population health risks of noise pollution from sources other than military aircraft, which could be used as a basis for future environmental and public health impact assessments.
Materials and methods
Study region.
Military training operations at NASWI originate from two primary airfields on Whidbey Island, Washington State, USA (Fig. 1 ). Ault Field is located approximately 5 km from the city of Oak Harbor, the largest community in Island County, while Outlying Landing Field (OLF) Coupeville is located 4 km from the town of Coupeville. Aircraft operations conducted at NASWI range from sessions of repeated closed-pattern routines (including “touch-and-go” field carrier landing practice, FCLP), to interfacility transfers and arrivals from and departures to off-station areas, including the Olympic Military Operations Area (MOA) on the Olympic Peninsula (the primary location of electronic warfare and air-to-air combat training). The flight paths for these operations extend across northwestern Washington, from the Pacific coast to the Cascade Mountains, encompassing the counties of Clallam, Jefferson, Island, San Juan, Skagit, and Snohomish, in Washington State, USA.

Monitoring locations are shown from the US Navy, JGL Acoustics Inc., and the National Park Service. The Swinomish Reservation and Samish Tribal Designated Statistical Area are indicated in yellow and green, respectively.
Analysis workflow
Acoustic metrics characterizing individual aircraft noise events and cumulative exposure levels were derived from acoustic data recorded at monitoring locations and used to validate a model simulating noise exposure across the entire study region. Modeled spatial predictions, expressed as noise contours, were overlaid with a dasymetric population density map to estimate population noise exposures at a fine spatial scale. Established thresholds and exposure-response functions were used to estimate the effect of the noise regime on multiple population health outcomes. This analysis workflow is detailed in Fig. 2 .

Data are shown as oblongs, while models and processing steps are shown as rectangles.
Acoustic monitoring data and metrics
Acoustic monitoring data consisted of sound pressure level (SPL) measurements collected during previous investigations into military aircraft noise, primarily from locations near the Ault and Coupeville airfields or their associated flight paths, both on Whidbey Island and throughout the surrounding region. Congress passed unique legislation in 2019 requiring the Navy to conduct acoustic monitoring around NASWI during four discrete weeks in 2020–2021, and at one location within the Olympic MOA for 365 days [ 33 ]. These data were obtained from the Naval Facilities Engineering Systems Command [ 34 ]. Additional monitoring data from 2015 to 2019 were obtained from JGL Acoustics, Inc. and the National Park Service Night Skies and Natural Sounds Division [ 21 , 35 , 36 ]. In total, 20 unique locations were examined (Supplementary Table S 1 ). SPL measurements were conducted with a class 1 sound level meter at a 1 Hz sampling rate and included A frequency-weighted equivalent continuous SPL L Aeq and, where available, A-weighted fast time-weighted maximum SPL L AFmax and peak C-weighted L Cpeak . Frequency spectrum measurements consisted of Z-weighted L Zeq in one-third octave bands and were only available for a subset of locations. Further details regarding data collection can be found in the relevant references [ 21 , 35 , 36 , 37 ].
We calculated a suite of acoustic metrics to characterize noise from single overflight events and cumulative noise levels associated with aircraft operations. Metrics were selected for their ubiquity in domestic and international standards and policy for land use compatibility, and because they provide the basis for exposure-response relationships concerning human health impacts [ 7 , 9 , 11 , 12 , 38 , 39 , 40 ]. All metrics throughout this study use A frequency weighting unless otherwise specified.
Single event metrics included the sound exposure level L E (also referred to as SEL), the 1-second average event maximum L max , the fast time-weighted maximum L Fmax , and (when available) the instantaneous C-weighted peak sound pressure level L Cpeak . All metrics were calculated in accordance with standards established by the International Organization for Standardization (ISO) and the Navy [ 11 , 37 ]. The spectral content of noise events was measured in one-third octave frequency bands for a subset of monitoring locations near Coupeville airfield (locations 6-10) having a high prevalence of FCLP aircraft events. Spectrums were energy-averaged for individual events, then energy-averaged within sites to yield a representative FCLP for each location.
Overflight events were detected from continuous SPL time-series data according to guidelines established in ISO 20906 and the SAE Aerospace Recommended Practice [ 38 , 41 ], and following the approach used by the Navy for noise monitoring [ 37 ]. A 10 second moving average was applied to each SPL time-series, smoothing the signal and reducing small variations that might otherwise be incorrectly labeled as events. An individual event was detected when this level exceeded a threshold varying with ambient conditions; ISO procedures recommend estimating background sound by the 95% exceedance level of total sound L 95 , and aircraft maxima should measure at least 15 dB above residual sound [ 38 ]. We note that some time-series data were collected only during periods of active aircraft operations (Supplementary Table S 1 ) and lacked a representative reference background. The threshold for event detection for these time-series was the maximum value between the L 95 of the hour (+/−30 min) and a baseline 35 dB + 15 = 50 dB ambient value for each second. An event was determined to terminate when the level fell and remained below the threshold for 5 s. Detected events containing multiple peaks above a local exceedance threshold (e.g., due to rapid flybys or multiple aircraft operating simultaneously) were subdivided into individual events corresponding with each peak. Detected acoustic events at locations 1–12 were cross-referenced against reported events from the Navy [ 34 ] and verified as military aircraft events accordingly. Detected events at locations 13–20 were manually verified by a trained observer [ 21 , 35 , 36 ].
Cumulative metrics quantify noise exposure over periods of time and form the basis of most community or public health impact assessments. Calculated cumulative metrics included: L dn , the day-night average sound level (also referred to as DNL), with a +10 dB penalty applied to nighttime periods (22:00-07:00); L den , the day-evening-night average sound level, with a penalty of +5 and +10 dB applied to evening (19:00-22:00) and nighttime (22:00-07:00) periods, respectively; L night , the equivalent continuous sound pressure level during nighttime hours; and L eqH , the equivalent continuous sound pressure level over a specified time period H , such as 24 h. Cumulative noise exposure within the Olympic MOA was quantified only with L dnmr , the onset-rate adjusted monthly day-night average sound level, as it is conventionally used to account for the sporadic nature and potentially high onset rates of noise within special-use airspace [ 37 ].
Cumulative acoustic metrics were calculated for every monitoring location and date, including L dn , L den , L night , L eq24h , and hourly L eq . These metrics were computed directly from continuous time-series measurements L eq,1s , rather than an aggregation of individual noise events L E , in accordance with ISO standards [ 11 ] and to enable direct comparisons of ambient noise levels on days with and without flight operations.
Aircraft operations data and simulation models
Detailed flight operations records were obtained from the Naval Facilities Engineering Systems Command for the four weeklong monitoring periods in 2020 and 2021, which were designed to capture “a range of flight operations across a range of seasonal weather conditions… during periods of high, medium, and low flight activity” [ 34 , 37 ]. These records documented flight profile and track activity from Ault Field and OLF Coupeville, as well as maintenance and engine run-up operations. Records for training routes and airspace profiles within the Olympic MOA were also obtained for a 365-day period within 2020 and 2021. These data were originally collected for the Navy Real-Time Aircraft Sound Monitoring Study [ 33 ] and presented a unique opportunity to investigate direct links between military aircraft operations and the noise regime.
We used the Noisemap software suite to simulate and spatially map noise exposure across the study region [ 42 ]. Noisemap is a noise modeling tool approved by the United States Department of Defense and used by the Navy to predict noise from flight operations. It integrates airfield operational data, flight profile specifications (including track, altitude, and speed), and a library of reference noise measurements with environmental terrain data to simulate the acoustic propagation of generated noise and resulting exposure at a grid of points on the ground level. The number of operations used by Noisemap is based on the average annual day, or the average number of airfield operations that would occur during a single day assuming 365 days of flying per year [ 37 ]. The average number of total operations during the four discrete monitoring periods was approximately 83% of the projected total operations for an “average year” at NASWI for 2021 [ 30 ], thus underestimating true flight activity at the annual scale.
Operations data were summarized as the total number of operations per flight profile for each period, and the mean number of operations per flight profile was calculated across all monitoring periods. This yielded a final model representing average flight activity across all periods throughout the year. Noisemap then simulated this activity, including additional noise due to maintenance and preflight ground run-up operations, such that the total predicted aircraft noise exposure was the accumulated noise exposure generated from all active operations of aircraft on all flight profiles [ 42 ].
The Noisemap model produced noise exposure contours in 1 dB increments for L dn , L night , and L eq24h from a grid of points spaced evenly at a standard distance of 914 m, or 3000 ft. The model also calculated noise exposure at specific locations corresponding to monitoring locations 1–11 to enable comparison of simulated noise metrics with those empirically measured by acoustic monitoring in the field. A second simulation was created to estimate noise exposure within the Olympic MOA using operations data averaged across the year.
Lastly, we applied the models to simulate the health impacts of alternative noise regimes by scaling the relative quantity of total flight operations across the range of 50–150%, ultimately projecting the response of population health outcomes to decreases or increases in aircraft activity. While this included estimates for the total number of operations projected for 2021 from the Navy environmental impact statement, it should be noted that this simple scaling of operations quantities from the four discrete monitoring periods does not accurately reflect the true operations and fleet composition active throughout 2021, and the projected population impact estimates are not representative, but rather demonstrative.
Population noise exposure
US population distributions are often derived from census units, which vary in geographic size based on population density. Units in urban areas are typically small with evenly distributed populations, while units in rural areas are larger with irregularly distributed populations. Using census units as a basis for population assessment can substantially limit the resolution of any spatial analysis of rural communities, and can reduce the accuracy of estimated impacts from socio-environmental problems [ 43 , 44 ].
To overcome this limitation, we implemented a workflow established by Swanwick et al. to create a 30-m resolution population density estimate for the study area [ 45 ]. This approach dasymetrically distributed block-level population estimates across all non-transportation impervious surfaces for each census block in the study area. We used the same approach to estimate population density for federally- and state-recognized tribal reservations and tribal-designated statistical areas (TDSA). Population data were obtained from the US Census Bureau’s 2021 American Community Survey, and impervious surface area data from the most recently available 2019 National Land Cover Database [ 46 ]. Simulated noise contours produced from Noisemap were rasterized to the same 30-m resolution as the population density map and intersected to yield an estimate of the number of people exposed to noise levels at or above thresholds established by domestic policy and international guidelines and associated with a substantial risk of impact on human health.
The World Health Organization (WHO) strongly recommends reducing aircraft noise levels below 45 dB L den , as aircraft noise above this level is associated with adverse health effects [ 9 ]. As such, we considered the 45 dB L dn contour to represent the spatial extent of adverse cumulative noise exposure, and the population residing within this area was therefore exposed to quantities of noise known to be harmful to human health. Additional thresholds used to estimate the at-risk population included aircraft noise levels associated with annoyance (45 dB L den ) [ 9 ], adverse effects on sleep (40 dB L night ) [ 9 ], a risk of hearing impairment over time (70 dBA L eq24 ) [ 3 , 39 ], and land use incompatibility according to regulations set by the Navy, Federal Aviation Administration (FAA), and US Department of Housing and Urban Development (65 dB L dn ) [ 27 , 47 , 48 ]. The number of individuals predicted to be impacted by these health risks vary according to the relationships described in the following section.
Population health impacts
Population health impacts, evaluated according to the number of individuals estimated to experience an adverse health outcome due to noise exposure, were calculated using established exposure-response relationships for annoyance, sleep disturbance, and compromised childhood learning (Fig. 3 ). These health outcomes were selected because they serve as critical indicators of community health [ 2 , 3 , 4 ], they are ubiquitous in noise law (e.g. environmental assessment [ 30 ], land-use [ 27 , 47 , 48 ]), and they have published exposure-response relationships that are commonly implemented in domestic and international policy and standards to assess health outcomes from noise [ 9 , 11 , 16 , 49 ]. In particular, WHO guidelines identify these outcomes as having sufficiently robust exposure-response relationships to support quantitative health assessment [ 9 ]. These outcomes are also the first responses in a stress-mediated chain of physiological effects that can lead to more severe health consequences. Noise exerts effects either directly though objective sound exposure (hearing impairment or sleep disturbance) or indirectly through the subjective emotional and cognitive perception of sound (annoyance) [ 1 , 4 , 50 ]. Both of these pathways elicit neurobiological stress responses that in turn promote cardiovascular risk factors (blood pressure, glucose levels) that can manifest in disease (hypertension, ischemic heart disease) [ 1 , 4 , 50 , 51 ] or induce psychological effects that jeopardize mental health (anxiety, depression) [ 4 , 50 , 52 ].

Functions relating L dn to high annoyance ( A ) and L night to high sleep disturbance ( B ) are illustrated with shaded 95% confidence intervals, where available.
These downstream health outcomes, namely cardiometabolic and psychological effects, were excluded from consideration in the present study because they currently lack generalized exposure-response relationships for public health assessment and are not widely used in domestic and international noise policy and guidelines. While relationships have been quantified for cardiometabolic and psychological effects [ 52 , 53 , 54 ], inconclusive empirical support and methodological differences between studies has precluded the development of robust generalized exposure-response relationships [ 53 ] and led to the exclusion of these health outcome assessments from WHO guidelines [ 9 , 55 , 56 ]. The chosen outcomes of annoyance, sleep disturbance, and childhood learning serve as proven indicators of community health that can be used to inform policy and prioritize future primary assessments of additional health outcomes from members of the population directly.
While most international noise policies and guidelines rely on L den as the primary cumulative noise metric [ 9 , 11 , 49 ], a majority of US states (including Washington) do not apply a penalty to the evening time period, and instead rely on L dn . As such, operational flight profile data from the simulation models were only available in day-night periods, and the following health analyses use L dn in lieu of L den . This is expected to result in slightly more conservative estimates than would be expected if L den were available, given that aircraft flight operations were not uncommon during evening hours.
To predict prevalence of high annoyance and high sleep disturbance throughout the population, associated exposure-response functions were used to obtain an estimated percentage of the population impacted from the noise exposure level at the 30 m 2 spatial grain (raster). Levels exceeding the defined range of a function were capped at the maximum predicted response value, while levels below were assigned a value of zero. The estimated population of each raster was multiplied by this percentage and summed across all units within the study area to estimate the total population subject to each health outcome.
Exposure-response curves quantifying the relationship between aircraft noise exposure and human annoyance can differ dramatically by region, community, and type of aircraft and activity. Similarly, curves used in public health policy vary widely between nations. For example, the dose-response curve endorsed by the Federal Interagency Committee on Noise (FICON) [ 40 ] remains the current US standard for estimating community response to noise exposure, and is employed by the FAA and Navy. However, the recent comprehensive Neighborhood Environmental Survey (NES) conducted by the FAA found that this standard does not reflect the current US public perception of aviation noise and provided an updated and nationally representative exposure-response curve [ 12 ]. Exposure-response curves developed and recommended by the ISO and WHO represent intermediate responses for a given noise exposure level [ 9 , 11 ].
Although these relationships are commonly applied in the implementation of health risk assessment and noise policy related to commercial and civil aircraft noise, there is evidence that they may underestimate impacts of noise from military aircraft due to the dramatic differences in the frequency and intensity of military aircraft events [ 12 , 19 , 20 , 22 , 57 ]. For these reasons, we include a unique exposure-response relationship developed by Yokoshima et al., based on a synthesis of individual studies on aircraft noise from US military and Japan Self-Defense Forces [ 19 ]. Collectively, these five exposure-response curves were used to assess the range of predicted impacts by relating aircraft noise L dn to the probability of a population being highly annoyed (Fig. 3A ).
- Sleep disturbance
Substantial evidence supports the considerable and consistent effects of aircraft noise on sleep disturbance [ 9 , 58 ]. These exposure-response relationships are based on survey and experimental assessments that identify aircraft noise as the cause of awakenings from sleep, the process of falling asleep, and/or sleep disturbance. Nighttime noise exposure near military airfields has been found to substantially reduce sleep quality [ 20 , 59 ]. However, because these studies are highly limited in number, exposure-response curves relating sleep disturbance to military aircraft noise exposure are not available. As such, we employed two published exposure-response curves that relate nighttime aircraft noise L night to the probability of being highly sleep disturbed (Fig. 3B ), namely, the guideline curve presented by the WHO and an updated version of this curve by Smith et al. that includes more recent survey data [ 9 , 58 ]. As previously discussed, these curves are expected to result in conservative estimates of impacted populations.
Childhood learning
We investigated the noise exposure levels at geographic centers of public, private, and postsecondary schools within the study area, obtained from the National Center for Education Statistics [ 60 ]. Systematic reviews conducted by the WHO and National Academies of Sciences, Engineering, and Medicine found evidence for a negative effect of aircraft noise exposure on reading and oral comprehension, standardized assessment performance, and long-term and short-term memory in children at school [ 5 , 61 ]. Specifically, WHO guidelines identify an increased risk of impaired reading and oral comprehension at 55 dB L den , equating to a 1 month delay in reading age, and an additional 1–2 month delay for each 5 dB increase beyond 55 dB L den [ 9 ]. As simulations produced estimates of L dn for the average annual day, assuming 365 days of exposure, we derived this noise level specific risk for each school according to its level of equivalent continuous exposure over a school year duration of 180 days.
Hearing impairment
Environmental noise pollution associated with military airfields and military operating areas can occur at levels that can result in both short- and long-term hearing impairment [ 62 , 63 , 64 ]. An exposure-response curve directly relating cumulative noise exposure to hearing impairment has not been developed at the population scale. Instead, acute noise exposures that could impact hearing were calculated and compared against action levels for occupational noise according to protocols established by the Occupational Safety and Health Administration and the National Institute for Occupational Safety and Health [ 65 , 66 ]. Because this analysis requires measurement of continuous sound levels over time as opposed to cumulative metrics, daily noise exposure doses using a 24-h reference duration (representing potential exposure experienced by residents) were calculated for monitoring locations only. Single-event noise levels were also compared against established thresholds for direct physiological impairment [ 24 , 67 ].
Military aircraft noise regime
Noise events from military aircraft operations often exhibited a characteristic contour, with a fast onset rising to a maximum peak, followed by a gradual decay (Fig. 4 ). The magnitude, onset rate, and duration of events varied by operation and monitoring location across the study region.

A single FCLP noise event L eq ( A ) and spectrogram ( B ); an FCLP training session ( C , D ). Data recorded at monitoring location 7 on August 10, 2021.
The loudest aircraft noise event measured at each monitoring location ranged from 85.4–119.8 dB L max and 94.3–122.7 dB L E (Supplementary Table S 2 ). At all monitoring locations on Whidbey Island, as well as off-island locations in Port Townsend (location 11) and the Skagit River (location 2), events were measured in excess of 100 dB L max . Noise events during active operations at the MOA location were recorded up to 90 dB L max , 95.4 dB L E . The single loudest event occurred during a touch-and-go operation near OLF Coupeville (location 15) measuring 119.8 dBA L max , 121.1 dBA L Fmax , 136.2 dBC L Cpeak , 122.7 dBA L E , at the time of approximately 23:57.
Spectral energy of aircraft noise occupied an expansive range of the frequency spectrum extending beyond the limits of human audibility. The amount of high frequency noise increased with proximity to aircraft, though substantial amounts of low-frequency energy were present in all noise events, regardless of distance. Energy-averaged Z-weighted levels of one-third octave band spectra from locations within approximately 3 km of an active FCLP session exhibited a broad peak around roughly 300 Hz of 65 to 85 dBZ, and up to 69 dBZ at infrasonic frequencies and 51 dBZ at 20 kHz.
During the four 2020–2021 monitoring periods, Ault Field conducted a wide range of operations, including Olympic MOA departure, arrival, and pattern operations, while the vast majority of operations at OLF Coupeville were FCLPs. Inter-field transit operations were common between both airfields. Ault Field conducted an average of approximately 1134 operations, including 145 FCLPs, per weeklong monitoring period, while OLF Coupeville conducted an average of 760 operations, including 690 FCLPs [ 33 ]. A single FCLP counts as two operations, one for takeoff and one for landing. The average weekly number of combat training operations conducted within the Olympic MOA was 66.
Flight operations were concentrated from Monday through Thursday (91.4%), with less activity on Friday (7.1%) and minimal activity on weekends (1.4%). On Friday, Saturday, and Sunday, operations were only conducted from Ault Field. Roughly 70% of operations occurred during daytime hours, 20% during the evening, and 10% at night. Operations were recorded at all hours except 2:00 and 4:00 AM. FCLP sessions at OLF Coupeville took place during the hours of 11:30 to 23:30, ranging in duration from 30 min to 3 h (lasting approximately 1 h on average), with multiple sessions typically occurring on a single day. Sessions have continued past midnight during other recorded monitoring periods [ 35 ]. The vast majority of operations within the Olympic MOA occurred during weekdays, with roughly 97% occurring during the day, and 3% at night.
L den increased dramatically on days with substantial flight activity. Compared to weekends (little operation at Ault Field, none at OLF Coupeville), weekdays at monitoring locations within and immediately surrounding Whidbey Island exhibited energy-averaged increases ranging from approximately 8–28 dB L den , except for those at Lopez Island (location 3) and Port Townsend (location 11) where differences were negligible. Similarly, L night increased during weekdays, with differences ranging from approximately 3–29 dB. Average hourly L eq increased by up to roughly 35 dB during flight operations, compared to hours when no operations were occurring. As an increase of 10 dB is typically perceived by the human ear as a doubling in loudness, this equates to a roughly 11-fold increase in loudness during hours of operation.
Simulation model validation
The Navy determined that Noisemap modeling “operates as intended and provides an accurate prediction of noise exposure levels from aircraft operations for use in impact assessments and long-term land use planning” [ 37 ]. For each location within the 2020–2021 monitoring period (excluding the Olympic MOA), we compared the estimated L dn from our simulation against results from the Navy’s monitoring study, namely a) the modeled DNL, simulated by Noisemap per-period and then energy-averaged across periods, and b) the real-time measured DNL, calculated from discrete event SEL metrics computed directly from acoustic monitoring data. We found that our simulated results were highly correlated with both the modeled and measured DNL, with Pearson correlation coefficients of 0.99 ( P < 0.001) and 0.97 ( P < 0.001), respectively (Supplementary Fig. S 1 ). The mean difference between our simulated L dn and the modeled DNL was 0.72 dB (min 0, max 3), while the mean difference with the measured DNL was 4.25 dB (min 0.9, max 8.2), falling within the accepted range expected by the Navy’s monitoring programs [ 33 ]. Simulation of airspace activity within the Olympic MOA yielded a cumulative noise exposure of approximately 35 dB L dnmr throughout the area, approximately 4.8 dB less than the measured energy-average of 39.8 dB DNL during periods of operations across the entire 365-day period.
The total area of noise exposure associated with adverse health effects was 1278 km 2 (427.5 km 2 not including water) (Fig. 5 ), with an estimated exposed population of 74,316 people (Fig. 6 ). Exposure was most severe along flight tracks for airbase arrival, departure, and closed-pattern routines, with L dn reaching beyond 90 dB near landing strips at both Ault Field and OLF Coupeville. Interfacility transit operations also substantially contributed to the spatial extent of noise exposure, exhibiting L dn contours of up to 65 dB.

L dn , day-night average sound level, from 45 dB ( A ); L night , night average sound level, from 40 dB ( B ); L eq24 , 24-h equivalent continuous sound level, from 70 dB ( C ). Additional contours below risk thresholds are shown as dotted lines for context.

Population size, in thousands, is illustrated per 5 dB L dn of military aircraft noise exposure (lower bound inclusive).
Simulated operations within the Olympic MOA resulted in a cumulative noise exposure of approximately 35 dB L dnmr throughout the area, with measured individual monthly L dn ranging from approximately 34–47 dB L dn . Because the annual average was below the 45 dB L dn threshold, we determined that no health impacts could be estimated for the MOA.
Estimated populations at risk of adverse health outcomes were substantial (Table 1 ). Island County was the most severely impacted region in terms of total number of exposed people (56,813), amounting to approximately two thirds of the total county population. This included all residents of the cities of Oak Harbor and Coupeville. The Swinomish Reservation was the most severely impacted region in terms of the percentage of community exposure, at roughly 85% of the local reservation population. A total of 74,316 people were exposed to day-night average levels of at least 45 dB L den , posing a risk of annoyance [ 9 ], while 41,089 were exposed to nighttime average levels of at least 40 dB L night , posing a risk of adverse effects on sleep [ 9 ]. An estimated 8059 people, all residing within fairly close proximity to Ault Field or OLF Coupeville, were exposed to average noise levels exceeding 70 dBA L eq24 that can induce hearing impairment over time [ 3 , 39 ]. All monitoring locations on Whidbey Island during the same monitoring periods exceeded this level on at least one day, including those lying outside of 70 dBA L eq24 contours. A total of 12,449 people were exposed to 65 dB L dn or greater, noise levels incompatible with residential land use according to regulations set by the Navy, FAA, and US Department of Housing and Urban Development, and eligible for community noise mitigation funds [ 27 , 33 , 47 , 48 , 68 ].
The estimated population health impacts vary according to different published benchmarks (Table 2 ). According to WHO guidelines, 20,840 people were estimated to be highly annoyed. This estimate ranges from 5873 to 36,916 depending on the exposure-response function used (FICON or Yokoshima, respectively). A total of 5265 people were estimated to be exposed to levels at or beyond the defined range of all annoyance exposure-response functions except FICON (75 dB L dn ). Between 8315 to 9770 people were estimated to be highly sleep disturbed (WHO versus Smith). Importantly, 4967 people were estimated to be exposed to levels at or beyond the defined range of sleep disturbance exposure-response functions (65 dB L night ).
Several monitoring locations within roughly 3 km of OLF Coupeville surpassed the recommended exposure limit of the National Institute for Occupational Safety and Health (≥85 dB time-weighted average). Days with multiple FCLP sessions occasionally surpassed exposure thresholds for the FAA Hearing Conservation Program, which would require providing hearing protection and testing for employees [ 69 ]. Multiple noise events at a residence near OLF Coupeville (location 15) reached short-term intensities that may cause direct, acute mechanical damage to the inner ear [ 24 , 67 ].
Six schools were exposed to noise levels associated with increased risk of reduced reading and oral comprehension (≥55 dB L dn , Supplementary Table S 3 ) [ 9 ], with the quantitative risk of a 1–2 month delay in learning per 5 dB increase. The most severely impacted schools (Coupeville Middle School, Coupeville High School, and Crescent Harbor Elementary) had an estimated exposure of 60–63 dB L dn , suggesting the risk of a 2–3 month delay in learning for students. An additional 12 schools were exposed to noise levels within 5 dB of the 55 dB L dn threshold. Columbia College, a postsecondary school near Ault Field, experienced exposure of 70 L dn ; impacts were not able to be estimated, however, given that the average student is older than the ages for which this relationship is defined.
Particularly loud individual aircraft noise events occurred during school hours at schools in proximity of flight tracks. At the field monitoring location nearest Crescent Harbor Elementary (location 1, distance of approximately 1 km), events surpassed 103 dB L max and 113 dB L E . Considering a standard 15–25 dB reduction to approximate indoor levels, noise events of such magnitude are known to interfere with student and teacher conversation and comprehension [ 70 , 71 , 72 ].
Simulation of alternative noise regimes
Simulation of alternative noise regimes revealed a positive relationship between aircraft operations and the estimated population impacted by all health outcomes across a wide range of total operations (Fig. 7 ). This relationship is nonlinear, as it is dependent on both the spatial distribution of the population and the range of levels for which thresholds and exposure-response relationships are defined. A 50% increase in annual operations yielded a 6.8% increase in the total exposed population, while a 50% decrease in operations yielded a 37% decrease in the exposed population. A 50% increase in operations increased cumulative noise levels within the Olympic MOA to no more than 36.4 dB L dnmr .

The equivalent annual number of operations for the four monitoring periods and the total number of operations projected for 2021 from the Navy environmental impact statement are both shown as vertical dashed lines.
Pervasive noise pollution from military aviation in western Washington exposes communities to an array of risks and impacts to human health and well-being. A majority of countries, including the United States, lack regulations that limit environmental noise pollution. This supports the needs for approaches, such as the one presented here, that allow for quantifying population health risks and impacts relative to established exposure-response relationships and regulatory guidelines from other noise-focused policies (e.g., occupational noise, land-use compatibility for civilian airports). Through the estimation of potential health burdens and projected increases and decreases in aircraft operations, this approach can inform impacted communities, highlight points of interest and areas that should be prioritized for alleviation and noise mitigation strategies, and better inform aircraft operational design, urban planning, and the development of improved policies to protect the public from the adverse human burden of noise exposure.
Our results suggest that noise exposure due to military aircraft activities within the study region poses a substantial risk and impact to public health. A majority of the resident population of Island County (66%) were exposed to noise levels associated with adverse health effects. Using WHO guidelines, 21% were estimated to be highly annoyed and 9% to be highly sleep disturbed. The Swinomish Indian Tribal Community of the Swinomish Reservation was extremely vulnerable to health risks, with nearly 85% of residents being exposed. The greatest impacts were predicted for populations residing near airfields and flight tracks, though the effects permeate broadly across the landscape. Our predictive modeling of health outcomes focuses on annoyance and sleep disturbance as critical indicators of community health for which sufficient research exists to employ exposure-response relationships. Ultimately, these outcomes are the first responses in a chain of physiological effects that can result in more severe health impacts. Stress responses can be triggered as a downstream consequence of sleep disturbance or the emotional and cognitive perception of sound (annoyance), promoting cardiovascular and psychological risk factors [ 4 , 52 ]. Mounting evidence from recent laboratory and longitudinal studies point to these underlying physiological and neurobiological mechanisms as pathways through which noise increases the risk of, or leads to, the onset of disease [ 4 , 50 , 51 , 52 ]. This strongly suggests that noise exposure should be considered as an environmental risk factor for the development of cardiometabolic and psychological disease and disorder [ 50 ]. While our study did not include a primary assessment of health outcomes from members of the population directly, the scale and severity of the indicators presented here imply considerable and diverse impacts to public health that warrant further investigation.
The estimated extent of population impacts varies widely depending on the standard or exposure-response relationship that is employed. For example, use of the FAA’s newly revised NES exposure-response curve for high annoyance, as opposed to the current FICON standard, increased population health impacts by almost 4-fold. Health impacts can also vary across individuals, and exposure-response relationships are influenced by the life experience and culture of the populations from which they are derived [ 19 ]. This wide range in estimated impacts suggests that there is uncertainty associated with current methods for health assessment, and conventional thresholds governing permissible community exposure, such as the 65 dB L dn contour used by the Navy, FAA, and US Department of Housing and Urban Development for land-use compatibility, may fail to protect populations from the adverse effects of noise exposure they were designed to. Despite this, the exposure-response relationships used in this study are currently employed in health assessments at an international scale, meaning that estimated public health risks and associated costs to society will vary widely. We suggest that variation in population health impact estimates starkly illustrates the need to reduce uncertainties in our understanding of how noise exposure results in human health outcomes and identify levels of permissible exposure informed by the best available science.
Critical gaps remain in our ability to assess health outcomes from military aviation noise specifically, and environmental noise pollution in general. First, an important finding of this study was that a substantial portion of the population was exposed to noise levels at or beyond the defined range of exposure-response relationships. This indicates that these levels of exposure are unprecedented in community noise analyses. Although there are few circumstances outside of close proximity to military airfields where such exposure is likely to be routine, it remains that the expected community response and health impacts from aircraft noise exposure at such extreme levels is unknown. Second, our simulation also produced contours for noise levels below those commonly presented in conventional assessments, but still proven to elicit adverse health effects. For example, domestic assessments often limit contours to 65 dB L dn and above [ 33 ], while the Environmental Noise Directive requires that assessments report population estimates exposed to 55 dB L den and above [ 49 ], despite evidence that adverse human health effects can be experienced at 45 dB L dn [ 9 ]. When considering an entire population, even comparatively low levels of exposure can yield substantial societal effects. As such, we urge future health assessments to consider the entire range of noise exposure known to be harmful to human health.
Perhaps the most significant knowledge gap involves the difference in estimated impacts between the exposure-response curves for noise from military versus civil aircraft [ 19 , 25 ]. This difference is dramatic and warrants further study to understand the role of acoustic (both single-event and cumulative metrics) and non-acoustic indicators in future community health assessments of noise from military aviation. For example, military aircraft noise within the study region exhibited substantial low-frequency energy. The conventional use of A frequency weighting underestimates the contribution of this energy to noise measurements and has been criticized as inadequate to quantify such low-frequency noise events [ 73 , 74 ]. Low-frequency noise propagates farther than higher frequency noise, and therefore A-weighted contours may underestimate the true spatial extent of noise exposure. Additionally, low-frequency noise is not easily attenuated by physical barriers such as walls and windows and can resonate with building structures and the human body, creating secondary effects of rattling and vibration [ 73 , 75 , 76 ]. This minimizes the efficacy of sound insulation and can promote feelings of helplessness in residents [ 73 ]. While the specific health impacts of low-frequency noise exposure remain understudied, evidence suggests that it can elicit a substantially more rapid increase in perceived loudness, annoyance, and sleep disturbance, even at low sound pressure levels [ 3 , 73 , 75 , 76 ]. The WHO and ISO suggest that guidelines for permissible exposure to low-frequency noise should be lowered and rating procedures for the assessment of such noise should be modified [ 11 ]. However, there remains little consensus on what modifications are appropriate due to a dearth of research relating low-frequency noise exposure to health impacts. Future improvements to noise simulation tools such as Noisemap should include the ability to calculate C-weighted levels to better quantify exposure to low-frequency noise.
Military aircraft activity within the study region also exhibited a more sporadic noise regime than that associated with common commercial or civil aviation, which may contribute to more severe health impacts than are predicted by cumulative acoustic metrics such as L dn [ 22 ]. Individual events can have significant implications for health outcomes that cumulative metrics fail to account for. This suggests that communities outside of the 45 dB L dn contour may still be subject to noise exposure that is associated with adverse health effects. For example, although most residents of Port Townsend, Camano Island, Lopez Island, and Forks (a city within the Olympic MOA) reside outside the area that poses a relevant risk of annoyance according to the WHO, these communities have reported high numbers of noise complaints [ 29 ]. This may be exacerbated in areas within the Olympic MOA in particular, such as Forks, due to the intermittent nature of noise events and comparatively reduced presence of other environmental noise [ 18 ]. However, current research linking single-event indicators to long-term population health impacts remains tentative, and as such these metrics are not widely employed in assessment guidelines [ 9 ].
Simulations of alternative noise regimes suggest that population health impacts can be slightly reduced, but definitely not avoided, by decreasing the volume of aircraft operations. While increased operations are associated with more severe health impacts, the spatial extent of noise exposure (and the mere presence of health risks) is driven in particular by the flight pattern of active operations. Therefore, reducing population exposure and subsequent health impacts may best be achieved by strategically discontinuing or altering the flight paths of operations that result in the most egregious impacts, such as FCLP operations, as well as reducing the volume. Changing the timing of operations to avoid sensitive periods, such as school and nighttime hours, may also substantially reduce the risk of associated health impacts. Further opportunities may exist in the creation of subsidy programs for sound insulation or even the purchase of homes in high exposure areas, such as those for commercial airports in the US [ 27 , 71 ] or military airfields abroad [ 20 , 25 ]. However, it should be noted that although sound insulation has been shown to reduce indoor exposure to traffic and commercial aircraft noise [ 77 , 78 ], prior research suggests that it may be ineffective in reducing the high intensity and low-frequency noise associated with military aircraft [ 20 ].
Finally, the spatial extent of noise exposure presented in this study, and thus the magnitude of predicted health risks and impacts, is likely underestimated due to limitations of available data. The scaling of operations occurring within the four weeklong monitoring periods to the entire year amounted to 83% of the volume of total operations suggested by the Navy for all of 2021 [ 30 ]. Compared to our simulation, modeled yearly average L dn values presented in the Navy environmental impact statement are louder at most monitoring locations, some by up to 10.5 dB [ 37 ], and the area of the 65 dB L dn contour is approximately 1.23 times as large (not including water or the NASWI complex) [ 30 ]. This suggests that human health impacts from the true annual noise regime are likely even more severe than those shown here.
The approach presented here improves on existing methods of assessing the population health risk of noise by increasing transparency and reproducibility. Although acute and chronic noise pollution is an issue for many communities worldwide, noise and operations from NASWI have been closely scrutinized for many years. This has led to unique monitoring datasets and a rare legal action that critically examined, and ultimately rejected, the environmental impact statement process and procedures as implemented by the Department of Defense [ 79 ]. Other recent successful lawsuits also underscore the inadequacy of current environmental assessment practices and policies related to noise [ 80 ], and the burden on communities to organize and self-advocate for change [ 81 ]. Our approach offers several benefits and improvements for noise impact assessment. The first is that we rely on published exposure-response relationships to transparently and systematically estimate impacts for multiple health outcomes. These relationships can be expanded or updated as new information becomes available (e.g., exposure-response curves for cardiovascular or psychological impacts). A second improvement lies in the integration of dasymetric population density maps which provide a more accurate estimation of exposed populations, particularly across different types of non-urban areas such as those prevalent in the study region. This is important as noise pollution is not an exclusively urban issue, extending well outside city centers. Finally, this workflow can be used to project the expected magnitude and geography of population health risk resulting from proposed changes in activity, including both increases and decreases in flight operations related to new policy and mitigation strategies (e.g., land use changes, sound insulation programs). We believe that this approach can be employed by both noise producers and affected communities as a basis for common dialogs that extend beyond noise exposure to discuss human health impacts and potential solutions.
Military aviation operations data are typically not available to the public, and noise monitoring around airfields is rare. This study purposefully leveraged datasets that arose from unique policy instruments [ 33 ] and robust monitoring funded by federal agencies [ 21 ] and community organizations [ 35 , 36 ]. We believe this approach offers a roadmap that communities elsewhere can use to effectively plan and implement rigorous noise monitoring and systematically collect operational data. For example, the datasets that facilitated this assessment have common features, including the use of class 1 sound level meters to collect an array of SPL measurements and a robust means to identify individual events automatically or through simultaneous observation for comparison with operations data. The workflow presented makes more accessible the conversion of these raw acoustic data into meaningful metrics for communication. Using this example, community-led initiatives could advocate for government funding to support noise monitoring studies or conduct their own investigations with volunteers. The ongoing evolution of inexpensive monitoring equipment and advances in acoustic analysis increase this likelihood, with strong potential for application of AI-based automated detection of noise events from long-term passive monitoring [ 82 ]. Such datasets collected through community science could provide useful validation of noise modeling and exposure [ 83 , 84 ], although overcoming sporadicity must be considered [ 85 ]. This may offer a much-needed mechanism to organize and advocate for mitigation and could go a long way to alleviating the powerlessness that communities commonly experience related to noise pollution [ 86 ].
By using a modular analytical framework, this approach can be extended to diverse noise sources well beyond the purview of military aircraft, including any context where the spatial extent of noise exposure can be modeled. This offers a promising avenue to bridge monitoring gaps for other environmental noise sources that are poorly documented and monitored yet still affect communities worldwide. The framework can also be readily updated or customized with other health thresholds and exposure-response relationships to serve future assessments in other contexts. The insights obtained through this approach may help better inform efforts in mitigating community noise exposure and developing policy governing noise legislation and land use. We strongly encourage future public health assessments of environmental noise pollution to leverage such a workflow in an effort to obtain a comprehensive understanding of the magnitude of health implications associated with noise exposure at the population scale with the best available science.
Data availability
Code for the methods and workflow routines can be found at the open-source repository github.com/giojacuzzi/noise-pollution-pop-health-naswi [ 87 ]. Noisemap software is available from the US Department of Defense Community and Environmental Noise Primer resources at dodnoise.org/primer_resources. BaseOps version 7.368 was used as the graphical user interface for Noisemap simulation data entry and management in concert with a) Omega10 and Omega11 to calculate sound over distance for aircraft flight operations, ground maintenance, and run-up operations; b) NMap 7.3 and MRNMap to calculate noise exposure values on the ground; c) NMPlot 4.974 to convert calculated noise exposure values to noise contour plots. Data from the 2020–2021 Navy monitoring periods are available from the Naval Facilities Engineering Systems Command Aircraft Sound Monitoring database [ 34 ], including acoustic monitoring data, flight operations data, and noise modeling data. Acoustic monitoring data from the 2015 National Park Service Night Skies and Sounds Division report and 2016 and 2019 JGL Acoustics, Inc. reports are available upon reasonable request. Impervious surface data used in the dasymetric population density mapping are available from the National Land Cover Database [ 46 ]. School geographic locations are available from the National Center for Education Statistics [ 60 ].
Basner M, Babisch W, Davis A, Brink M, Clark C, Janssen S, et al. Auditory and non-auditory effects of noise on health. Lancet. 2014;383:1325–32.
Article PubMed Google Scholar
Stansfeld SA, Matheson MP. Noise pollution: Non-auditory effects on health. Br Med Bull. 2003;68:243–57.
Berglund B, Lindvall T, Schwela DH. Guidelines for community noise. Geneva, Switzerland: World Health Organization; 1999.
Sørensen M, Pershagen G, Thacher JD, Lanki T, Wicki B, Röösli M, et al. Health position paper and redox perspectives - Disease burden by transportation noise. Redox Biol. 2024;69:102995.
Sharp BH, Connor TL, McLaughlin D, Clark C, Stansfeld SA, Hervey J. Assessing Aircraft Noise Conditions Affecting Student Learning, Volume 1: Final Report. Washington, D.C.: Transportation Research Board; 2014.
Swinburn TK, Hammer MS, Neitzel RL. Valuing quiet: An economic assessment of US environmental noise as a cardiovascular health hazard. Am J Preventive Med. 2015;49:345–53.
Article Google Scholar
Hammer MS, Swinburn TK, Neitzel RL. Environmental noise pollution in the United States: Developing an effective public health response. Environ Health Perspect. 2014;122:115–9.
Astley RJ. Can technology deliver acceptable levels of aircraft noise? Inter Noise Noise Con Congr Conf Proc. 2014;249:2622–33.
Google Scholar
World Health Organization. Environmental noise guidelines for the European Region. Geneva, Switzerland: World Health Organization; 2018.
European Environment Agency. Environmental noise in Europe—2020. Luxembourg, Luxembourg: European Environment Agency; 2020.
International Organization for Standardization. Acoustics – Description, measurement and assessment of environmental noise – Part 1: Basic quantities and assessment procedures. ISO 1996-1 Third edition. Geneva, Switzerland: International Organization for Standardization; 2016.
US Department of Transportation, Federal Aviation Administration. Analysis of the Neighborhood Environmental Survey. Washington, DC: US Department of Transportation; 2021.
D'Alessandro F, Schiavoni S. A review and comparative analysis of European priority indices for noise action plans. Sci Total Environ. 2015;518:290–301.
Hammer MS, Fan Y, Hammer SS, Swinburn TK, Weber M, Weinhold D, et al. Applying a novel environmental health framework theory (I-ACT) to noise pollution policies in the United States, United Kingdom, and the Netherlands. J Environ Plan Manag. 2018;61:2111–32.
Perna M, Padois T, Trudeau C, Bild E, Laplace J, Dupont T, et al. Comparison of road noise policies across Australia, Europe, and North America. Int J Environ Res Public Health. 2021;19:173.
Article PubMed PubMed Central Google Scholar
Fidell S. A review of US aircraft noise regulatory policy. Acoust Today. 2015;11:25–34.
Kuehne LM, Erbe C, Ashe E, Bogaard LT, Salerno Collins M, Williams R. Above and below: Military aircraft noise in air and under water at Whidbey Island. Wash J Mar Sci Eng. 2020;8:923.
Kuehne LM, Olden JD. Military flights threaten the wilderness soundscapes of the olympic peninsula, Washington. Northwest Sci. 2020;94:188–202.
Yokoshima S, Morinaga M, Tsujimura S, Shimoyama K, Morihara T. Representative exposure-annoyance relationships due to transportation noises in Japan. Int J Environ Res Public Health. 2021;18:10935.
Matsui T. A Report on the Aircraft Noise as a Public Health Problem in Okinawa. Okinawa, Japan: Department of Culture and Environmental Affairs Okinawa Prefectural Government; 1999.
Pipkin A. Ebey’s Landing National Historical Reserve: Acoustical monitoring report. Natural resource report. NPS/ELBA/NRR—2016/1299. Fort Collins, CO: National Park Service; 2016.
Gelderblom FB, Gjestland TT, Granøien ILN, Taraldsen G. The impact of civil versus military aircraft noise on noise annoyance. Inter Noise Noise Con Congr Conf Proc. 2014;249:786–95.
Waitz IA, Lukachko SP, Lee JJ. Military aviation and the environment: Historical trends and comparison to civil aviation. J Aircr. 2005;42:329–39.
Ising H, Rebentisch E, Poustka F, Curio I. Annoyance and health risk caused by military low-altitude flight noise. Int Arch Occup Environ Health. 1990;62:357–63.
Article CAS PubMed Google Scholar
Morinaga M, Kawai K, Makino K. Aircraft noise annoyance around military airfields in Japan. Inter Noise Noise Con Congr Conf Proc. 2016;253:854–63.
US Department of Defense. DoD Instruction 4715.13 DoD operational noise program. Washington, DC: US Department of Defense; 2020.
Code of Federal Regulations. 14 CFR part 150–Airport noise compatibility planning. Washington, DC: Federal Aviation Administration.
US Department of Transportation. National transportation noise map documentation. Washington, DC: US Department of Transportation; 2020.
Quiet Skies Over San Juan County. Jet noise density maps. 2022. Available from: https://www.quietskies.info/basic-01 .
US Department of the Navy. Final environmental impact statement for EA-18G growler airfield operations at Naval Air Station Whidbey Island Complex. Washington, DC: US Department of the Navy; 2018.
Fox J, Morris L. A summary of the association between noise and health. Olympia, WA: Washington State Department of Health; 2017.
US District Court Western District of Washington at Seattle. Case No. 2:19-cv-01059-RAJ-JRC Document 119. Seattle, WA: US District Court Western District of Washington at Seattle; 2022.
US Department of the Navy. Real-time aircraft sound monitoring final report. Washington, DC: US Department of the Navy; 2021.
Naval Facilities Engineering Systems Command. Aircraft sound monitoring. 2018. Available from: https://www.navfac.navy.mil/Directorates/Public-Works/Products-and-Services/Aircraft-Sound-Monitoring/ .
Lilly J. Military jet noise measurements OLF Coupeville Whidbey Island, WA. Issaquah, WA: JGL Acoustics, Inc.; 2020.
Lilly J. Whidbey Island military jet noise measurements. Issaquah, WA: JGL Acoustics, Inc.; 2016.
Downing M, Gillis J, Manning B, Mellon J, Calton M. Navy real-time aircraft sound monitoring study: Technical report. Asheville, NC: Blue Ridge Research and Consulting, LLC; 2022.
International Organization for Standardization. Acoustics – Unattended monitoring of aircraft sound in the vicinity of airports. ISO 20906, 1st ed. Geneva, Switzerland: International Organization for Standardization; 2009.
US Environmental Protection Agency. Information on levels of environmental noise requisite to protect public health and welfare with an adequate margin of safety. Washington, DC: US Environmental Protection Agency; 1974.
Federal Interagency Committee on Noise. Federal agency review of selected airport noise analysis issues. Washington, DC: Federal Interagency Committee on Noise; 1992.
SAE International. ARP4721. Monitoring aircraft noise and operations in the vicinity of airports: System description, acquisition, and operation. Warrendale, PA: SAE International; 2021.
US Air Force Civil Engineer Center. BaseOps 7.368 User’s Guide. 2023. Available from: http://dodnoise.org/resources/pdfs/BaseOps_User_Guide.pdf .
Jelinski DE, Wu J. The modifiable areal unit problem and implications for landscape ecology. Landsc Ecol. 1996;11:129–40.
Tiecke TG, Liu X, Zhang A, Gros A, Li N, Yetman G, et al. Mapping the world population one building at a time. arXiv. 2017;1712:05839.
Swanwick RH, Read QD, Guinn SM, Williamson MA, Hondula KL, Elmore AJ. Dasymetric population mapping based on US census data and 30-m gridded estimates of impervious surface. Sci Data. 2022;9:523.
Yang L, Jin S, Danielson P, Homer C, Gass L, Bender SM, et al. A new generation of the United States National Land Cover Database: Requirements, research priorities, design, and implementation strategies. ISPRS J Photogramm Remote Sens. 2018;146:108–23.
US Department of Defense. Air installations compatible use zones program. Washington, DC: US Department of Defense; 2022.
Code of Federal Regulations. 24 CFR B–Noise abatement and control. Washington, DC: US Department of Housing and Urban Development; 2013.
European Parliament and the Council of the European Union. Directive 2002/49/EC. Strasbourg, France: European Parliament and the Council of the European Union; 2002.
Münzel T, Sørensen M, Daiber A. Transportation noise pollution and cardiovascular disease. Nat Rev Cardiol. 2021;18:619–36.
Osborne MT, Radfar A, Hassan MZO, Abohashem S, Oberfeld B, Patrich T, et al. A neurobiological mechanism linking transportation noise to cardiovascular disease in humans. Eur Heart J. 2020;41:772–82.
Hahad O, Kuntic M, Al-Kindi S, Kuntic I, Gilan D, Petrowski K, et al. Noise and mental health: evidence, mechanisms, and consequences. J Exp Sci Environ Epidemiol. 2024;26;1–8.
Babisch W, Kamp I. Exposure-response relationship of the association between aircraft noise and the risk of hypertension. Noise Health. 2009;11:161.
Vienneau D, Schindler C, Perez L, Probst-Hensch N, Röösli M. The relationship between transportation noise exposure and ischemic heart disease: a meta-analysis. Environ Res. 2015;138:372–80.
Van Kempen E, Casas M, Pershagen G, Foraster M. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Cardiovascular and Metabolic Effects: A Summary. Int J Environ Res Public Health. 2018;15:379.
Clark C, Paunovic K. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Quality of Life. Wellbeing Ment Health Int J Environ Res Public Health. 2018;15:2400.
European Commission. Position paper on dose response relationships between transportation noise and annoyance. Luxembourg, Luxembourg: European Commission; 2002.
Smith MG, Cordoza M, Basner M. Environmental noise and effects on sleep: An update to the WHO systematic review and meta-analysis. Environ Health Perspect. 2022;130:076001.
Kim SJ, Chai SK, Lee KW, Park JB, Min KB, Kil HG, et al. Exposure–response relationship between aircraft noise and sleep quality: A community-based cross-sectional study. Osong Public Health Res Perspect. 2014;5:108–14.
National Center for Education Statistics. School locations & geoassignments. 2019. Available from: https://nces.ed.gov/programs/edge/geographic/schoollocations .
Clark C, Paunovic K. WHO environmental noise guidelines for the European region: A systematic review on environmental noise and cognition. Int J Environ Res Public Health. 2018;15:285.
Ising H, Joachims Z, Babisch W, Rebentisch E. Effects of military low-altitude flight noise part I: Temporary threshold shift in humans. Z fur Audiologie. 1999;38:118–27.
Kuronen P, Pääkkönen R, Savolainen S. Low-altitude overflights of fighters and the risk of hearing loss. Aviat Space Environ Med. 1999;70:650–5.
CAS PubMed Google Scholar
Hiramatsu K, Matsui T, Ito A, Miyakita T, Osad Y, Yamamoto T. The Okinawa study: An estimation of noise-induced hearing loss on the basis of the records of aircraft noise exposure around Kadena Air Base. J Sound Vib. 2004;277:617–25.
Occupational Safety and Health Administration. 1910.95 Appendix A - Noise Exposure Computation. Washington, DC: Occupational Safety and Health Administration; 2021.
US Department of Health and Human Services National Institute for Occupational Safety and Health. Occupational noise exposure; criteria for a recommended standard. Washington, DC: US Department of Health and Human Services National Institute for Occupational Safety and Health; 1998.
Babisch W. Noise and Health. Environ Health Perspect. 2005;113:A14–5.
US Department of Defense. Community noise mitigation. 2021. Available from: https://oldcc.gov/our-programs/community-noise-mitigation .
US Department of Transportation, Federal Aviation Administration. Flight standards service hearing conservation program. Order 3900.66A. Washington, DC: US Department of Transportation; 2021.
US Department of Defense. Improving aviation noise planning, analysis and public communication with supplemental metrics. Washington, DC: US Department of Defense; 2009.
Lind SJ, Pearsons K, Fidell S. Sound insulation requirements for mitigation of aircraft noise impact on Highline school district facilities volume I. BBN Systems and Technologies, BBN Report No. 8240. Cambridge, MA: BBN Systems and Technologies; 1998.
Sharp BH, Plotkin KJ. Selection of noise criteria for school classrooms. Arlington, VA: Wyle Research; 1984.
Berglund B, Hassmén P, Job RFS. Sources and effects of low‐frequency noise. J Acoust Soc Am. 1996; 99:2985–3002.
Committee on Technology for a Quieter America. Technology for a Quieter America. Washington, DC: National Academies Press; 2010.
Vos J, Houben MMJ. Annoyance caused by the low-frequency sound produced by aircraft during takeoff. J Acoust Soc Am. 2022;152:3706.
Persson K, Björkman M. Rylander R. Loudness, annoyance and dBA in evaluating low frequency sounds. J Low Frequency Noise, Vib Act Control. 1990;9:32–45.
Ehrlich GE, Gurovich Y. A Typical Case Study of School Sound Insulation. Arlington, VA: Sound and Vibration; 2004.
Xie J, Zhu L, Lee HM. Aircraft Noise Reduction Strategies and Analysis of the Effects. Int J Environ Res Public Health. 2023;20:1352.
Kelly JK. The sound of freedom at Naval Air Station Whidbey: Environmental impact review under the National Historic Preservation Act and National Environmental Policy Act. Villanova Environ Law J. 2020;31:3.
Mitsuzumi S. Okinawans file mass lawsuit over U.S. base noise pollution. The Asahi Shimbun. 2022. Available from: https://www.asahi.com/ajw/articles/14535305 .
Lorenzana R, Cherrier M, Seto E, Curle D, Albert J, Wong L, et al. Beacon Hill Seattle noise measurement project. OSF. 2019. Available from: http://osf.io/fn5z6 .
Morinaga M, Mori J, Yamamoto I. Aircraft model identification using convolutional neural network trained by those noises in a wide area around an airfield. Acoustical Sci Technol. 2023;44:131–6.
Noise Project. Homepage. 2023. Available from: https://noiseproject.org/ .
Challéat S, Farrugia N, Gasc A, Froidevaux J, Hatlauf J, Dziock F, et al. Silent Cities. 2023. Available from: https://osf.io/h285u/ .
Aceves-Bueno E, Adeleye AS, Feraud M, Huang Y, Tao M, Yang Y, et al. The accuracy of citizen science data: A quantitative review. Bull Ecol Soc Am. 2017;98:278–90.
Dreger S, Schüle SA, Hilz LK, Bolte G. Social inequalities in environmental noise exposure: A review of evidence in the WHO European region. Int J Environ Res Public Health. 2019;16:1011.
Jacuzzi G. giojacuzzi/noise-pollution-pop-health-naswi: 1.0. Zenodo. Available from: https://doi.org/10.5281/zenodo.10652377 (2024).
Download references
Acknowledgements
We are grateful to individuals and organizations that shared and facilitated access to noise monitoring data: Jerry Lilly of JGL Acoustics, Inc., and Ashley Pipkin of the National Park Service Night Skies and Natural Sounds Division. We appreciate the contributions and feedback of many community members and stakeholders that provided input on the project design and interim results via three community webinars. We also thank three anonymous reviewers for their helpful suggestions in improving the manuscript.
Funding for this study was provided by a Tier 2 research grant from the University of Washington’s Population Health Initiative.
Author information
Authors and affiliations.
School of Aquatic and Fishery Sciences, College of the Environment, University of Washington, Seattle, WA, 98195, USA
Giordano Jacuzzi & Julian D. Olden
Omfishient Consulting, Bremerton, WA, 98310, USA
Lauren M. Kuehne
Sound Defense Alliance, PO Box 373, Coupeville, WA, 98239, USA
Anne Harvey & Christine Hurley
Citizens of Ebey’s Reserve, PO Box 202, Coupeville, WA, 98239, USA
Robert Wilbur
School of Public Health, University of Washington, Seattle, WA, 98195, USA
Edmund Seto
You can also search for this author in PubMed Google Scholar
Contributions
GJ: Methodology, software, validation, formal analysis, data curation, writing (original draft), writing (review and editing), visualization. LMK: Conceptualization, methodology, validation, investigation, data curation, writing (review and editing), funding acquisition. AH: Conceptualization, writing (review and editing), funding acquisition. CH: Conceptualization, data curation, writing (review and editing), funding acquisition. RW: Conceptualization, data curation, writing (review and editing), funding acquisition. ES: Conceptualization, methodology, writing (review and editing), funding acquisition. JDO: Conceptualization, methodology, formal analysis, writing (review and editing), supervision, funding acquisition.
Corresponding author
Correspondence to Giordano Jacuzzi .
Ethics declarations
Competing interests.
The authors declare no competing interests.
Ethical approval
Ethical approval was not required for the purposes of this study as no research was conducted with personal human data. Data from the US Census Bureau and American Community Survey is anonymized.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary information, rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Cite this article.
Jacuzzi, G., Kuehne, L.M., Harvey, A. et al. Population health implications of exposure to pervasive military aircraft noise pollution. J Expo Sci Environ Epidemiol (2024). https://doi.org/10.1038/s41370-024-00670-1
Download citation
Received : 17 October 2023
Revised : 22 March 2024
Accepted : 27 March 2024
Published : 09 May 2024
DOI : https://doi.org/10.1038/s41370-024-00670-1
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Noise assessment
- Environmental noise
- Exposure-response
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies


About CDMRP

Since 1992, Congress has provided funding for the Congressionally Directed Medical Research Programs (CDMRPs) in the annual Defense Appropriations Act. Specific funding levels are provided for disease-specific programs, ranging from more common cancers to rare diseases to Gulf War Illness. The programs are administered by the U.S. Army Medical Research and Materiel Command (USAMRMC) at the Department of Defense (DoD).
Funding for the CDMRPs is not included in the President’s budget – it is added by the House and Senate Appropriations Committees during deliberations on the Defense Appropriations Act. Funding for each program within the CDMRP is determined through a rigorous legislative process involving grassroots advocacy, careful vetting by the appropriations committees and scrutiny from individual Members of Congress and the media.
While the CDMRPs have enjoyed significant bipartisan and bicameral support, there are those in Congress and the media who have criticized CDMRPs, or have suggested transferring the programs to the National Institutes of Health (NIH). Continued budgetary pressures and renewed scrutiny of DoD medical research place the CDMRPs at considerable risk of losing funding in fiscal year 2017 and beyond. As an example, the Senate Armed Services Committee’s version of the fiscal year 217 National Defense Authorization Act included provisions that would have severely restricted, if not eliminated altogether, funding for the CDMRPs. On June 7, 2016, by a vote of 66-32, the Senate approved the Durbin amendment to remove these provisions and protect funding for the CDMRPs – the first time in recent history that funding for CDMRPs came to a recorded vote in Congress.
FOR MORE INFORMATION :
- Medical Research Programs (CDMRP) – Home Page
- CDMRP – Research Programs Page
LATEST NEWS
June 26, 2023
House Appropriations Committee approves FY24 Defense Appropriations Act
On June 22, the House Committee on Appropriations approved its version of the fiscal year 2024 Defense Appropriations Act. Approved 34 to 24 along party lines, the bill would provide $826.45 billion for defense spending in the fiscal year starting October 1, staying within spending caps negotiated in the debt ceiling agreement.
The House Committee mark largely includes funding for the Congressionally Directed Medical Research Programs (CDMRPs) at existing fiscal year 2023 levels. The bill provides $10 million to create a new arthritis research program. Arthritis is currently an eligible condition in the Peer Reviewed Medical Research Program (PRMRP).
The House version of the bill will likely be brought to the House floor for consideration in July. The House may choose to first consider the fiscal year 2024 National Defense Authorization Act when it reconvenes on July 11.
In a related development, on June 22, the Senate Committee on Appropriations approved allocations for its versions of the fiscal year 2024 appropriations bills, including $823.3 billion for defense spending.
_______________________
November 22, 2022
The Defense Health Research Consortium and dozens of its affiliated members today sent a letter to House and Senate leadership, calling on them to “work toward the enactment of the fiscal year 2023 Defense Appropriations Act, to ensure full funding levels for the Defense Health Research Programs, including the Congressionally Directed Medical Research Programs (CDMRP).”
November 16, 2022
Rep. Ken Calvert has survived his re-election and will serve as chair of HAC-D
End-of-Year Outlook: What’s Left on the Congressional Agenda
Congress returns to Washington next week with a full agenda before adjourning for the year. Here is a look at what issues they may consider:
FY 2023 Appropriations
One benefit of the close elections is the path to finishing fiscal year (FY) 2023 appropriations may have gotten easier as Republicans will not have the leverage to punt the spending package into the new Congress. The current CR expires on December 16 th and Democrats in the House and Senate intend to negotiate and enact an omnibus spending package by then, or by the end of the calendar year. An omnibus would likely include supplemental Ukraine funding, disaster relief, mental health authorizations, and other priorities.
The $31.4 trillion debt limit will need to be raised by before the end of 2023. Influential Republicans have described the debt limit as a tool they will use to extract major spending cuts, despite the risk of crashing the economy. Therefore, Democrats and moderate Republicans are discussing the possibility of including a debt limit increase, or abolishing the debt limit, during the lame duck. President Biden opposes the abolishment of the debt limit, claiming it would be “irresponsible.” It is unclear there will be enough votes attached to this proposal to the omnibus. However, it would protect the economy under President Biden while solving the issue for the next Congress by taking it out of their hands.
Congress Passes Another Continuing Resolution to Extend Fiscal Deadline Through December 18
December 11, 2020
The Senate passed a one-week continuing resolution (CR) late Friday afternoon via voice vote, sending it to President Trump for his signature just hours before the midnight deadline. The President signed the bill Friday evening to keep the government open for another week while lawmakers work to reach an agreement on a spending package before the new December 18 deadline.
Lawmakers and staff worked over the weekend to finalize and file an omnibus package by COB today, but sources tell us lawmakers are still uncertain whether it is possible. Rumors are circulating that House Appropriations Committee staff have drafted a three-month CR that they could rely on if a final spending package isn’t ready by early this week. However, appropriators in both chambers are outwardly optimistic, including Senate Majority Leader Mitch McConnell (R-KY), who told reporters he is hopeful that progress on these items will produce a final bill this week.
Senate Passes FY 21 NDAA Conference Report
The Senate this afternoon passed H.R. 6395, the $740.5 billion FY 21 NDAA conference report, by a vote of 84 to 13.
President Trump had threatened to veto the bill because it excluded language repealing a legal shield to tech companies and included bill language that calls for renaming military bases named after confederate soldiers. The House passed the bill earlier this week by a strong vote of 335-78.
Congress Passes Continuing Resolution, Extending Fiscal Deadline
September 30, 2020
Today, Congress passed the continuing resolution (CR) to extend the fiscal deadline through December 11. According to a person familiar with the planning, President Trump will sign the CR on Thursday, but there won’t be a lapse in appropriations because of his intent to sign the measure, which the Senate cleared Wednesday on an 84-10 vote, several days after the House voted 359 to 57 to approve the bipartisan bill.
House Democrats Unveil a Short-term Spending Bill
September 22, 2020
House Appropriations Committee Chair Nita Lowey (D-NY) introduced a short-term CR to extend Fiscal Year (FY) 2020 funding beyond the September 30 fiscal deadline until December 11.
The Democrats reportedly introduced the bill on their own without support of the White House or House or Senate Republicans.
The Latest on the CR Negotiations
September 15, 2020
We are hearing the House is planning on filing a continuing resolution on Friday, and plan to take it up on the floor next week. How long the CR will last is still unknown, but it seems that Speaker Pelosi is in favor of February or March. Senate Majority Leader McConnell and Treasury Secretary Mnuchin unsurprising prefer the CR expire in December.
House Approves Fiscal Year 2021 Defense Appropriations Act
July 31, 2020
The House has approved the Fiscal Year 2021 Defense Appropriations Act, as part of a larger minibus package. There were no amendments that would have adversely impacted the CDMRPs. Now on to the Senate, which may not act on this until after the election.
The House has sent its members home for August but will call them back with a 24 hour notice if there is a deal on the next COVID-19 relief package.
EXTERNAL LINKS
- Congressionally Directed Medical Research Programs (CDMRP) – Home Page
- CDMRP – Research Programs Page

US reclassification could drive fresh research funding into pot sector
By Mrinalika Roy
(Reuters) - The U.S. pot sector could see an influx of medical research funding from healthcare investors amid renewed interest from pharmaceutical firms, should a proposal to reclassify cannabis as a lower-risk substance be approved, industry experts said.
The current classification as a Schedule I substance has limited research into cannabis due to restricted access to cannabis products, regulatory hurdles and funding limitations.
Federal research grants are essentially off the table, while potential legal complexities put off many private foundations.
But that may change with the U.S. Justice Department's proposal to reclassify cannabis.
"For years, pharma and biotech companies have viewed cannabis as a market with enormous potential," said Michael Johnson, CEO of Metrc, which makes software to track the cannabis supply chain.
"With rescheduling, investment firms that previously had clauses precluding them from investing may reconsider their stance."
Currently, research with Schedule 1 substances requires a more rigorous registration process, oversight from several agencies and special storage arrangements.
Rescheduling would ease requirements such as the need to store cannabis in a steel safe with video coverage and alarms and lead to lower expenses, said Mark Bolton, head of global public policy at Jazz Pharma, which makes the only U.S. FDA-approved medicine derived from the marijuana plant.
Maridose LLC — one of eight companies on the Drug Enforcement Administration's approved list to manufacture and supply marijuana for research — said it has been receiving more enquiries from both non-profits and commercial entities, including state-licensed cannabis firms.
Reclassification will also free pot firms from the 280E tax provision, allowing listing on major U.S. exchanges.
"We expect to see healthcare venture capitalists move quickly to invest in cannabis-related research that can lead to new cannabis startups," Metrc's Johnson said.
There has been increased interest especially from small family offices and small hedge funds, AdvisorShares CEO Noah Hamman said. AdvisorShares offers several exchange traded funds, including Pure US Cannabis, the biggest U.S.-listed pot ETF.
Experts, however, said a financial overhaul of the sector is needed to attract bigger investors and banks.
"Rescheduling will spur more investment ... (but) will you now see JPMorgan and some of the traditional blue-chip investment firms willing to lend? That's probably going to take a little bit more time," Zack Kobrin, partner at law firm Saul Ewing, said.
(Reporting by Mrinalika Roy, Manas Mishra and Pratik Jain in Bengaluru; Editing by Arpan Varghese and Shounak Dasgupta)

Skip to Content

Current Students

Interested in more? Search Courses
- Search Input Submit Search
Faculty and Staff Grants From March 2024
University of denver, congratulations to the university of denver faculty and staff members who received grants and awards in march 2024 for the following projects..

Synthetic Protein Mimetics-Based Specific Targeting and Degradation of TDP-43 Aggregation Associated With ALS
- Sunil Kumar and Daniel Linseman , College of Natural Sciences & Mathematics
- Grant from U.S. Department of Defense
- Abstract: There are no effective treatments to cure or halt the progression of ALS disease, which is a common neurodegenerative disease characterized by the loss of motor neuron functions. One of the main causal agents associated with ALS pathology is the clumping of a neuronal protein called TDP-43 into aggregates. Therefore, the modulation of the aggregation of TDP-43 is considered to be a potential therapeutic intervention for ALS disease. We propose a novel two-pronged approach using synthetic protein mimetic molecules to modulate the TDP-43 aggregation. Overall, we believe that the completion of this study will empower the translation of drug-like ligands identified in our lab to potential lead therapeutics for the treatment of ALS.
Collaborative Research: Superinvaders: Testing a General Hypothesis of Forest Invasions by Woody Species Across the Americas
- Patrick Martin , College of Natural Sciences & Mathematics
- Grant from National Science Foundation
- Abstract: The main objective of this project is to better understand the functional constraints that drive adaptive trade-offs among woody species, using systematic observations and experiments across light gradients in temperate, subtropical and tropical forest. Our approach is transformative because it would test a new theory that integrates plant functional physiology and food web dynamics in a whole-plant carbon allocation framework.
Advocates for Recovery Colorado, Peer Recovery Support Services Expansion
- Meredith Silverstein , Graduate School of Social Work
- Grant from Advocates for Recovery Colorado (subaward City and County of Denver)
- Abstract: Advocates for Recovery Colorado (AFRC) is Colorado’s first and oldest recovery community organization. Since 2001, AFRC has provided no-cost peer recovery coaching and peer recovery support services to anyone regardless of stage of recovery or chosen recovery pathway. In alignment with Denver Public Health and Environment’s Treatment/People in Additional Areas Strategy Area, AFRC will achieve two key goals over the three-year funding period: expansion of services in Denver through the relocation of its recovery community center and expansion of services to people of color who are increasingly impacted by opioid misuse and overdose.
CueThinkEF+ - Phase 4 and 5 Partnership
- Stephen Hutt , Ritchie School of Engineering & Computer Science
- Grant from CueThink
- Abstract: The team will develop the EF Training feature during Phase 4, so that they will be ready for incorporation into a Phase 4 evaluation study that will allow for features to be rolled out and tested in an iterative manner.
Understanding Personal, Social Network and Neighborhood Environmental Contributors to Gun Access and Violence Among Young Adults Experiencing Homelessness
- Anthony Fulginiti , Graduate School of Social Work
- Grant from University of North Carolina (subaward Centers for Disease Control & Prevention)
- Abstract: Firearm-involved violence is an urgent public health issue in many major cities across the U.S., and youth experiencing homelessness (YEH) are especially vulnerable to violence, including firearm-involved violence. However, little research has focused on firearm risks among YEH. In fact, virtually nothing is known about individual, social network and neighborhood characteristics that may be associated with YEH's firearm risks. This information will provide a much-needed comprehensive understanding of firearm violence among YEH. This study will also inform interventions to reduce firearm violence among YEH and others who may be impacted by firearm violence among this vulnerable population.
History Colorado 2024 Amache Field School in Historic Archaeology and Museum Studies
- Bonnie Clark , College of Arts, Humanities & Social Sciences
- Grant from History Colorado
- Abstract: The Amache National Historic Site contains remarkably intact evidence of life in a WWII-era Japanese American incarceration camp, with building foundations, scattered surface artifacts and incarceree-created landscaping. In 2024, the University of Denver’s Department of Anthropology will continue its ongoing collaborative field school at the site and associated museum, followed by analysis and presentation of the resulting data. This project provides a rare opportunity for students and stakeholders to work together investigating the past and its meaning in the present at a national historic site.
Beyond the Ethnic Trap: Pathways From Power Sharing
- Timothy Sisk , Josef Korbel School of International Studies
- Grant from United States Institute of Peace (subaward AERDF - Advanced Education Research and Development Fund)
- Abstract: Escaping the Ethnic Trap explores the conditions under which inclusive governance and human rights can be fostered in contexts where prior conflict dynamics have created an ethnic trap in which identity-based politics undermines social cohesion and the inter-group interdependencies that give rise to sustainable peace.
Training System Assessment and Recommendations
- Charmaine Brittain , Graduate School of Social Work
- Grant from Colorado Department of Human Services
- Abstract: The Butler Institute for Families at the University of Denver Graduate School of Social Work (Butler) will partner with the Colorado Department of Human Services, Division of Child Support Services (CDHS-CS) to assess their training system and provide recommendations to strengthen it.
Colorado Universal Preschool RFP Development Process Evaluation
- Whitney Leboeuf, Colorado Evaluation Action Lab
- Grant from Colorado Department of Early Childhood
- Abstract: The Colorado Lab will develop a statement of work and support CDEC’s request for proposals (RFP) process to identify a vendor for a multi-year process evaluation of components of Colorado Universal Preschool. This work will result in a final RFP for CDEC, accompanied by recommended response evaluation criteria and vendor selection criteria.
NAACHO Harm Redux
- Grant from Mile High Council on Alcoholism and Drug Abuse
- Abstract: The Butler Institute for Families at the University of Denver, Graduate School of Social Work (Butler) will provide both evaluation and creative work in support of Mile High Behavioral Healthcare’s project to provide academic detailing for drag artists in Colorado. MHBHC’s academic detailing project will support drag artists to incorporate harm reduction messages into their work in the queer nightlife scene across the state and improve overdose prevention outcomes for LGBTQIA+ Coloradans.
Related Articles

Faculty and Staff Grants From January 2024
Faculty and Staff Grants from December 2023
Faculty and staff grants from november 2023.
IMAGES
COMMENTS
Currently Has Open Funding Opportunities. Defense Medical Research and Development Medical Simulation and Information Sciences Research Program (JPC-1) Military Infectious Diseases Research Program (JPC-2) Military Operational Medicine Research Program (JPC-5) Combat Casualty Care Research Program (JPC-6) Radiation Health Effects Research ...
DEPARTMENT OF DEFENSE - CONGRESSIONALLY DIRECTED MEDICAL RESEARCH PROGRAMS. Contact Us ... CDMRP Research Funding for 2024 IMPORTANT: Immediate Changes in System for Award Management (SAM) Registration Process for New and Existing Contractors; Last updated Friday, May 10, 2024.
Program Funding Opportunities. All pre-applications must be submitted electronically to the Electronic Biomedical Research Application Portal (eBRAP) https://ebrap.org. Full applications must be submitted electronically to the Grants.gov website https://grants.gov. To view past Program Funding Opportunities, please visit the Program Funding ...
Program Announcement. Application Instructions. Pre-Application (Letter of Intent): May 13, 2024 5:00 p.m. Eastern Time. Application: June 6, 2024 11:59 p.m. Eastern Time. Submit Pre-Application. Lifestyle and Behavioral Health Interventions Research Award (LBIRA) March 29, 2024.
Defense Health Program's RDT&E appropriation, as reflected in Figure 1. Biomedical research conducted by the Defense Advanced Research Projects Agency or other military research agencies is not included in this account. Figure 1. Total Defense Health Program (DHP) RDT&E Appropriation, FY2024 Source: Explanatory Statement accompanying P.L. 118-47,
The Consolidated Appropriations Act, 2023 provides medical research funding for the following programs managed by the Department of Defense, Congressionally Directed Medical Research Programs (CDMRP): Alcohol and Substance Use Disorders Research Program - $4.0 million;
Defense Health Program's RDT&E appropriation, as reflected in Figure 1. Biomedical research conducted by the Defense Advanced Research Projects Agency or other military research agencies is not included in this account. Figure 1. Total Defense Health Program RDT&E Appropriation, FY2022 Source: "Explanatory Statement accompanying H.R. 2471,"
The Peer Reviewed Medical Research Program (PRMRP), established in fiscal year 1999 (FY99), has supported research across the full range of science and medicine, with an underlying goal of enhancing the health, care, and well-being of military Service members, Veterans, retirees, and their family members. Program oversight is provided by a ...
Congressionally Directed Medical Research Programs (CDMRP). The U.S. Army Medical Research and Development Command (MRDC), in coordination with the Defense Health Agency, administers the program using a competitive grant process. CDMRP funding is to be used only for medical research on congressionally identified medical research topics (e.g ...
The Department of Defense's (DoD's) Congressionally Directed Medical Research Programs (CDMRP) has a well-established process for managing the review and selection of funding applications that it receives for its medical research programs. This chapter presents an overview of that process and provides a brief overview of CDMRP's organization and structure. The current functions of the program ...
For FY2021, $370 million was appropriated for the PRMRP. PRMRP funding supports grants for medical research on a number of conditions or treatment modalities that are of "clear scientific merit and direct relevance to military health.". Congress specifies an annual list of eligible conditions or treatments that typically includes a few ...
Combat Casualty Care Research Program (August Pre-app deadline) Chronic Pain Management Research Program (August Pre-app deadline) Toxic Exposures Research Program (September Pre-app deadlines) More programs to be posted soon. The most up to date information may be found on the DoD Funding Opportunities webpage.
Lewis-Burke Associates has provided campus with a report about the Department of Defense (DOD) Congressionally Directed Medical Research Programs (CDMRP) FY24 Peer Reviewed Medical Research Program (PRMRP) solicitations. For FY 2024, Congress has allocated $370 million for PRMRP in over forty topic areas. The PRMRP aims to support medical research projects of clear scientific merit that lead ...
Funding. The US Army Medical Research and Development Command (USAMRDC) Military Operational Medicine Research Program (MOMRP) manages research funding on behalf of the Department of the Army and the DoD Defense Health Program (DHP). This funding supports research at DoD laboratories and myriad extramural research organizations from small ...
committees on the Joint Warfighter Medical Research Program (JWMRP). This report lists the projects that receive funding, including the funding amount awarded to each project, a thorough description of each project's research, and the benefit this research will provide to the Department of Defense (DoD).
The Department of Defense Medical Research Office evolved from a long and successful partnership with the U.S. government. Numerous Mayo Clinic faculty and staff have been or are members of the U.S. military. The cornerstone of Mayo Clinic's rich heritage and commitment to military service can be traced back to the earliest days of Mayo Clinic ...
The Defense Health Research Consortium was founded by CRD Associates to bring a diverse community together to advocate for the CDMRP, a $1.5 billion medical research program designed to meet the unique health and medical challenges of the men and women in the U.S. Armed Services. Funding for the CDMRP is added every year by Congress to the ...
Registration is now open for the Congressionally Directed Medical Research Programs (CDMRP) workshop on Jan. 22! The Deputy Director and Program Managers from the U.S. Department of Defense will present an overview of CDMRP, cover specific programs upcoming in FY2024, and provide guidance on application submissions. Of note, research does not ...
Traumatic Brain Injury and Psychological Health ; Tuberous Sclerosis Complex; Vision; Additional Supported DOD Programs/Projects. Defense Medical Research and Development. Medical Simulation and Information Sciences Research Program (JPC-1) Military Infectious Diseases Research Program (JPC-2) Military Operational Medicine Research Program (JPC-5)
House Appropriations Committee Approves Fiscal Year 2023 Department of Defense Appropriations Bill with $20 M for Vision Research Program. 06/23/2022 - On June 22 the House Appropriations Committee approved its Fiscal Year (FY) 2023 Defense spending bill which includes $20 million in VRP funding, the fifth year that the program has been funded ...
Program Announcement for the Department of Defense . Defense Health Program . Congressionally Directed Medical Research Programs . Peer Reviewed Orthopaedic Research Program ... DOD FY24 Peer Review Orthopaedic Women's Health Research Award 25 . II.G.2. Grants.gov Contact Center Questions regarding Grants.gov registration and Workspace: Phone ...
The Defense Medical Research and Development Program (DMRDP) is directed by the Defense Health Program Enhancement initiative in the office of the Assistant Secretary of Defense for Health Affairs. ... Grants.gov is used for finding and applying for federal grants. The U.S. Department of Health and Human Services (HHS) serves as the managing ...
Providing more than $86 million for high-impact research on lupus. The Lupus Foundation of America led the fight to secure lupus research funding through the Department of Defense's (DoD) Congressionally Directed Medical Research Program (CDMRP). To date, our efforts have generated more than $86 million to fund high-impact, high-quality ...
In a letter to Defense Subcommittee Chairman Jon Tester (D-MT) and Ranking Member Susan Collins (R-ME), the Senator led a bipartisan group of his colleagues to urge the Appropriations leadership to support the strongest possible funding for the Traumatic Brain Injury and Psychological Health Research program within the Department of Defense ...
Grant Program Highlights. National Security Education Program The David L. Boren National Security Education Act of 1991 mandated that the Secretary of Defense create and sustain a program to award scholarships to U.S. undergraduate students, fellowships to U.S. graduate students, and grants to U.S. institutions of higher education.
Funding Statement. This work was supported by funding from the National Institute on Alcohol Abuse and Alcoholism (R01-AA030041) and the Department of Defense (HU0001-22-2-0066). Author Declarations. I confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been obtained. Yes
These health outcomes were selected because they serve as critical indicators of community health [2,3,4], they are ubiquitous in noise law (e.g. environmental assessment , land-use [27, 47, 48 ...
About CDMRP. Since 1992, Congress has provided funding for the Congressionally Directed Medical Research Programs (CDMRPs) in the annual Defense Appropriations Act. Specific funding levels are provided for disease-specific programs, ranging from more common cancers to rare diseases to Gulf War Illness.
By Mrinalika Roy. (Reuters) - The U.S. pot sector could see an influx of medical research funding from healthcare investors amid renewed interest from pharmaceutical firms, should a proposal to ...
Synthetic Protein Mimetics-Based Specific Targeting and Degradation of TDP-43 Aggregation Associated With ALS Sunil Kumar and Daniel Linseman, College of Natural Sciences & Mathematics Grant from U.S. Department of Defense Abstract: There are no effective treatments to cure or halt the progression of ALS disease, which is a common neurodegenerative disease characterized by the loss of motor ...