America’s Most Popular Drug Has a Puzzling Side Effect. We Finally Know Why.
The reason statins can make your muscles sore or weak was unclear—until scientists accidentally stumbled upon an answer.

Statins, one of the most extensively studied drugs on the planet, taken by tens of millions of Americans alone, have long had a perplexing side effect. Many patients—some 5 percent in clinical trials, and up to 30 percent in observational studies—experience sore and achy muscles, especially in the upper arms and legs. A much smaller proportion, less than 1 percent, develop muscle weakness or myopathy severe enough that they find it hard to “climb stairs, get up from a sofa, get up from the toilet,” says Robert Rosenson, a cardiologist at Mount Sinai. He’s had patients fall on the street because they couldn’t lift their leg over a curb.
But why should an anticholesterol drug weaken muscles in the arms and legs? Recently, two groups of scientists stumbled upon an answer. They didn’t set out to study statins. They weren’t studying cholesterol at all. They were hunting for genes behind a rare disease called limb girdle muscle dystrophy, in which muscles of the upper arms and legs—sound familiar?—become weak and waste away. After both teams tracked the disease through a handful of families in the U.S. and a Bedouin family in Israel , their suspicions separately landed on mutations in a gene encoding a particularly intriguing enzyme.
The enzyme is known as HMG-CoA reductase, and to doctors, it is not obscure. It is, in fact, the very enzyme that statins block in the process of halting cholesterol production. And so, the answers to two mysteries suddenly became clear at once: Dysfunction in this enzyme causes muscle weakness from both limb girdle muscular dystrophy and statins.
This connection between a rare disease and a common drug stunned the researchers. “It seemed too good to be true,” says Joel Morales-Rosado, a pathologist who worked on one of the studies as a postdoctoral researcher at the Mayo Clinic. “One of the first things you learn in medical school is association between statins and myopathy.” Now the answer as to why— along with a potential treatment for it—has emerged from the DNA of just a few patients living with a seemingly unrelated genetic disease.
The first patient the Mayo team studied had been showing signs of limb girdle muscular dystrophy since he was a child, and his symptoms worsened over time until he lost the ability to walk or breathe with ease. (The disease can also affect large muscles in the torso.) Now in his 30s, he wanted to know the genetic cause of his disease before having children and potentially passing it on to them. His two brothers had the disease as well. So the team looked for genes in which all three brothers had mutations in both copies, which is how they zeroed in on the gene for HMG-CoA reductase.
Six more patients from four other families confirmed the link. They too all had mutations in the same gene, and they too were all diagnosed with some degree of limb girdle muscular dystrophy. (Interestingly, for reasons we don’t entirely understand, they all have normal or low cholesterol.)
Unbeknownst to the Mayo team, a group of researchers halfway around the world was already studying a large Bedouin family with a history of limb girdle muscular dystrophy. This family also carried mutations in the gene encoding HMG-CoA reductase. Those afflicted began experiencing minor symptoms in their 30s, such as muscle cramps, that worsened over time. The oldest family members, in their late 40s or 50s, had lost all movement in their arms and legs. One bedridden woman had to be ventilated full-time through a hole in her windpipe. Another had died in their mid-50s, Ohad Birk, a geneticist and doctor at Ben-Gurion University of the Negev, in Israel, told me. When his team saw that this family had the mutations in HMG-CoA reductase, they too immediately recognized the potential link to statins.
This pair of studies in the U.S. and Israel “really strongly suggests” that statins cause muscle damage via the same HMG-CoA reductase pathway, says Andrew Mammen, a neurologist at the National Institutes of Health who was not involved in either study. The enzyme’s role had been suspected, he told me, but “it had never been proven, especially in humans.” (Questions still remain, however. The enzyme, for example, is found in tissues throughout the body, so why do these common side effects show up in muscles specifically?) Rosenson, at Mount Sinai, wondered if variations in this gene could explain why statins don’t affect everyone the same. Perhaps patients who suffer particularly severe muscle side effects already have less functional versions of the enzyme, which becomes problematic only when they start taking statins, which reduce its function even further. This research might end up concretely improving the life of at least some of the patients most severely affected by statins.
That’s because Birk’s team in Israel did not stop at simply identifying the mutation. For two decades, he and his colleagues have been studying genetic disorders in this Bedouin community in the Negev and developing genetic tests so parents can avoid passing them on to their children. (Cousin marriages are traditional there, and when two parents are related, they are more likely to carry and pass on the same mutation to a child.) With limb girdle muscular dystrophy, his team went one step further than usual: They found a drug to treat it. This drug, called mevalonolactone, allows muscle cells to function more normally even without the HMG-CoA reductase enzyme. Birk’s team first tested it in mice given doses of statins high enough to weaken their limbs; those also given mevalonolactone continued to crawl and even hang upside down on a wire just fine. They seemed to suffer no ill effects. When that experimental drug was given to the Bedouin woman bedridden with limb girdle muscular dystrophy, she also started regaining control of her arms and legs. She could eventually lift her arm, sit up by herself, raise her knees, and even feed her grandchild on her own. It was a dramatic improvement. Birk told me he has since heard about dozens of patients with limb girdle muscular dystrophy around the world who may benefit from this experimental drug.
Mammen and others think the drug could help a small subset of patients who take statins as well. However, the majority of patients—those with relatively minor pains or weaknesses that go away after they switch statins or have their dosage reduced—probably don’t need this new treatment. It probably even undermines the whole point of taking statins: Mevalonolactone eventually gets turned into cholesterol in the body, so “you’re basically supplying the building blocks for making more cholesterol,” Mammen said. But for some people, numbering in the thousands, severe muscle weakness does not go away even after they stop taking statins. These patients have developed antibodies to HMG-CoA reductase , which Mammen suspects continue to bind and disable the enzyme.
Mammen is eager for these patients to try mevalonolactone, and he’s been in touch with Birk, who unfortunately doesn’t have enough of the drug to share. In fact, he doesn’t even have enough to treat all of the other family members in Israel who are clamoring for it. “We’re not a factory. We’re a research lab,” Birk told me. Mevalonolactone is available as a research chemical, but that’s not pure and safe enough for human consumption. Birk’s graduate student Yuval Yogev had to manufacture the drug himself by genetically engineering bacteria to make mevalonolactone, which he then painstakingly purified. Making a drug to this standard is a huge amount of work, even for commercial labs. Birk is looking for a pharmaceutical company that could manufacture the drug at scale—for both patients with limb girdle muscular dystrophy and those with the most severe forms of statin-associated muscle damage.
Back in 1980, the very first person to receive an experimental dose of statins suffered muscle weakness so severe, she could not walk. (She had been given an extremely high dose.) Forty years later, muscle pain and weakness are still common reasons patients quit these very effective drugs. This recent breakthrough is finally pointing researchers toward a better understanding of statins’ toll on muscles, even if they still can’t fix it for everyone.
- Alzheimer's disease & dementia
- Arthritis & Rheumatism
- Attention deficit disorders
- Autism spectrum disorders
- Biomedical technology
- Diseases, Conditions, Syndromes
- Endocrinology & Metabolism
- Gastroenterology
- Gerontology & Geriatrics
- Health informatics
- Inflammatory disorders
- Medical economics
- Medical research
- Medications
- Neuroscience
- Obstetrics & gynaecology
- Oncology & Cancer
- Ophthalmology
- Overweight & Obesity
- Parkinson's & Movement disorders
- Psychology & Psychiatry
- Radiology & Imaging
- Sleep disorders
- Sports medicine & Kinesiology
- Vaccination
- Breast cancer
- Cardiovascular disease
- Chronic obstructive pulmonary disease
- Colon cancer
- Coronary artery disease
- Heart attack
- Heart disease
- High blood pressure
- Kidney disease
- Lung cancer
- Multiple sclerosis
- Myocardial infarction
- Ovarian cancer
- Post traumatic stress disorder
- Rheumatoid arthritis
- Schizophrenia
- Skin cancer
- Type 2 diabetes
- Full List »
share this!
October 18, 2023
This article has been reviewed according to Science X's editorial process and policies . Editors have highlighted the following attributes while ensuring the content's credibility:
fact-checked
peer-reviewed publication
trusted source

New study sheds light on long term effectiveness and safety of two widely used statins
by British Medical Journal

Explore further
Feedback to editors

Unobtrusive, implantable device could deepen our understanding of behavioral responses
22 minutes ago

Using MRI, engineers have found a way to detect light deep in the brain
30 minutes ago

Analysis reveals new insights into global surge of Strep A infections
32 minutes ago

Flicker stimulation shines in clinical trial for epilepsy
57 minutes ago

New research traces the spread of HIV in and from Indonesia
5 hours ago

Metabolism of autism reveals developmental origins

Under 4-minute milers' longevity shows that extreme exercise doesn't seem to curb lifespan
15 hours ago

Study shows how night shift work can raise risk of diabetes, obesity
18 hours ago

'Smart' contact lenses could someday enable wireless glaucoma detection

Low-cost MRI paired with AI produces high-quality results
Related stories.

Real-world data links rosuvastatin with signs of kidney damage
Jul 19, 2022

Real-world data links rosuvastatin to adverse effects on kidneys
Aug 18, 2022

Long-term outcomes of PCI, CABG compared for multivessel CAD
Oct 5, 2022

Best statins for reducing cardiovascular risk in people with diabetes found
Mar 24, 2022

Vitamin D supplements may reduce risk of serious cardiovascular events in older people
Jun 28, 2023

How to reduce your risk for coronary artery disease
Jan 25, 2023
Recommended for you

Keto diet boosts lifesaving antifungal drug in mice
22 hours ago

New drug reduces vascular leak and endothelial cell dysfunction in mice with sepsis
May 9, 2024

Scientists unravel how psychedelic drugs interact with serotonin receptors to potentially produce therapeutic benefits
May 8, 2024

New research reports on financial entanglements between FDA chiefs and the drug industry

About 90% of US adults are on the way to heart disease, study suggests

Intervention in Navajo Nation boosts uptake for heart failure drugs by 53%
Let us know if there is a problem with our content.
Use this form if you have come across a typo, inaccuracy or would like to send an edit request for the content on this page. For general inquiries, please use our contact form . For general feedback, use the public comments section below (please adhere to guidelines ).
Please select the most appropriate category to facilitate processing of your request
Thank you for taking time to provide your feedback to the editors.
Your feedback is important to us. However, we do not guarantee individual replies due to the high volume of messages.
E-mail the story
Your email address is used only to let the recipient know who sent the email. Neither your address nor the recipient's address will be used for any other purpose. The information you enter will appear in your e-mail message and is not retained by Medical Xpress in any form.
Newsletter sign up
Get weekly and/or daily updates delivered to your inbox. You can unsubscribe at any time and we'll never share your details to third parties.
More information Privacy policy
Donate and enjoy an ad-free experience
We keep our content available to everyone. Consider supporting Science X's mission by getting a premium account.
E-mail newsletter
Featured Topics
Featured series.
A series of random questions answered by Harvard experts.
Explore the Gazette
Read the latest.

Cancer risk, wine preference, and your genes

Excited about new diet drug? This procedure seems better choice.

How friends helped fuel the rise of a relentless enemy
Don’t need high cholesterol to benefit from statins.
Miles Martin
BWH Communications
Studies find drug protects against heart disease in high-risk groups
Two new studies found that statins, the most prescribed class of drugs to treat high cholesterol, are protective for high-risk groups who haven’t yet had a heart attack or stroke but could be at risk of one, according to Harvard-affiliated Brigham and Women’s Hospital.
The results provide additional context to a longstanding debate among the medical community about whether there are benefits to initiating statin use in people who don’t already have high cholesterol or cardiovascular disease. The studies appear in the JAMA Network Open and the Journal of the American Geriatrics Society.
“Statins are a first line class of drugs that can lower cholesterol and lower the risk of a second heart attack or stroke in people who have already had one — there’s no question about that,” said corresponding author Ariela Orkaby of the Brigham’s Division of Aging . “However, many clinicians still don’t agree on whether statins should be used as a preventative treatment for people who haven’t had a heart attack or stroke yet but are at high risk due to age or other factors.
“Our findings demonstrate statins have a protective effect even in people who haven’t had their first major cardiac event, which means there are still benefits to prescribing these medications for primary prevention of heart disease,” said Orkaby, who is also an investigator in the Veterans Affairs Geriatric Research Education and Clinical Center.
For most people, statins are well-tolerated and don’t have significant side-effects. However, some doctors over the last few years have called for these medications to stop being prescribed for certain people, including those with chronic kidney disease. Notably, cardiovascular disease is the leading cause of death for older adults with kidney disease.
“Our results suggest that for statins, frailty status doesn’t decrease benefit, and it may be the frailest older adults who benefit the most.” Ariela Orkaby, Brigham and Women’s Hospital
“There has been some chatter about statins causing muscle pains but, for the vast majority of people, these are very safe and effective medications,” said Orkaby. “The problem is that we’re still missing a lot of clinical evidence about their effectiveness in certain groups, which has made some doctors deprescribe statins out of caution.”
In their study of 14,828 people with chronic kidney disease, the researchers found that starting statins was associated with 9 percent reduced mortality and a 4 percent lower risk of heart attack or stroke. The team also looked at a much larger group of older adults without kidney disease, of whom 12 percent were frail. Among this group of 710,313 people, they found that statin therapy was associated with a 39 percent lower risk of mortality and 14 percent lower risk of a first heart attack or stroke. Both studies used data from the Veteran’s Affairs Healthcare System.
Notably, the researchers found that these reductions in mortality and disease risk were independent of frailty, which the researchers measured through a score that accounted for dozens of age-related health conditions.
“When we’re talking about the risk-benefit analysis of using a certain medication in older populations, we need to consider frailty because medications may not work as well or may cause more side effects in people who are frailer,” said Orkaby. “Our results suggest that for statins, frailty status doesn’t decrease benefit, and it may be the frailest older adults who benefit the most.”
While the two studies benefited from the large patient population and long-term follow-up afforded by working with VA data, the researchers caution that their conclusions drawn from past patient data should be validated in new clinical trials that prospectively address these questions.
“We’re still missing some of the evidence we need to fully understand the scope of what these medications do,” said Orkaby. “However, these studies tell us that until we have clinical data that suggests otherwise, statins are safe and effective for older people and those with chronic kidney disease.”
Disclosures: Ariela Orkaby accepted personal fees from Anthos Therapeutics during this research, unrelated to this work. Luc Djosse reports current research funding from Novartis, unrelated to this work.
This research was supported by grants from the National Institute on Aging (R03-AG060169) and Veterans Affairs (IK2-CX001800, I01 CX001025) .
Share this article
You might like.
Biologist separates reality of science from the claims of profiling firms

Study finds minimally invasive treatment more cost-effective over time, brings greater weight loss

Economists imagine an alternate universe where the opioid crisis peaked in ’06, and then explain why it didn’t
How old is too old to run?
No such thing, specialist says — but when your body is trying to tell you something, listen
How far has COVID set back students?
An economist, a policy expert, and a teacher explain why learning losses are worse than many parents realize
- See us on facebook
- See us on twitter
- See us on youtube
- See us on linkedin
- See us on instagram
Researchers solve mystery of how statins improve blood vessel health
Statins designed to lower cholesterol have long been noted to work in mysterious ways to improve other aspects of cardiovascular health. A Stanford Medicine-led study uncovers how they do it.
May 8, 2023 - By Nina Bai

Researchers at Stanford Medicine and their colleagues have discovered how statins improve cardiovascular health beyond lowering cholesterol. roger ashford/Shutterstock.com
Using new genetic tools to study statins in human cells and mice, Stanford Medicine researchers and collaborators have uncovered how the cholesterol-lowering drugs protect the cells that line blood vessels.
The findings provide new insight into statins’ curiously wide-ranging benefits, for conditions ranging from arteriosclerosis to diabetes, that have long been observed in the clinic.
“The study gives us an understanding, at a very deep mechanistic level, of why statins have such a positive effect outside of reducing LDL,” said professor of medicine Joseph Wu , MD, PhD, referring to low-density lipoprotein, or “bad” cholesterol. “Given how many people take statins, I think the implications are pretty profound.”
Statins are the most prescribed medications in the country, with more than 40 million Americans taking them. Developed in the 1980s from compounds found in mold and fungi, statins target an enzyme that regulates cholesterol production in the liver. But clinical trials have shown that they also seem to safeguard against cardiovascular disease beyond their ability to lower cholesterol.
Heart failure patients who take statins, for example, are less likely to suffer a second heart attack. They have also been shown to prevent the clogging of arteries, reduce inflammation and even lower cancer risk. Yet these underlying mechanisms are poorly understood.
“Statins were invented to lower cholesterol by targeting the liver. But we didn’t know the targets or the pathways in the cardiovascular system,” said Chun Liu , PhD, an instructor at the Stanford Cardiovascular Institute and co-lead author of the study published May 8 in Nature Cardiovascular Research . Mengcheng Shen , PhD, and Wilson Tan, PhD, postdoctoral scholars at the Stanford Cardiovascular Institute, are the other co-lead authors, and Wu is the senior author.

Hints from a dish
To take a closer look at statins’ effect on blood vessels, Liu and colleagues tested a common statin, simvastatin, on lab-grown human endothelial cells derived from induced pluripotent stem cells. Endothelial cells make up the lining of blood vessels, but in many diseases they transform into a different cell type, known as mesenchymal cells, which are poor substitutes.
“Mesenchymal cells are less functional and make tissues stiffer so they cannot relax or contract correctly,” Liu said.
The researchers suspected that statins could reduce this harmful transition. Indeed, endothelial cells treated with simvastatin in a dish formed more capillary-like tubes, a sign of their enhanced ability to grow into new blood vessels.
RNA sequencing of the treated cells offered few clues. The researchers saw some changes in gene expression, but they “didn’t find anything interesting,” Liu said.
It was not until they employed a newer technique called ATAC-seq that the role of statins became apparent. ATAC-seq reveals what happens at the epigenetic level, meaning the changes to gene expression that do not involve changes to the genetic sequence.
They found that the changes in gene expression stemmed from the way strings of DNA are packaged inside the cell nucleus. DNA exists in our cells not as loose strands but as a series of tight spools around proteins, together known as chromatin. Whether particular DNA sequences are exposed or hidden in these spools determines how much they are expressed.
“When we adopted the ATAC-seq technology, we were quite surprised to find a really robust epigenetic change of the chromatin,” Liu said.

ATAC-seq revealed that simvastatin-treated cells had closed chromatin structures that reduced the expression of genes that cause the endothelial-to-mesenchymal transition. Working backward, the researchers found that simvastatin prevents a protein known as YAP from entering the nucleus and opening chromatin.
The YAP protein is known to play important roles in development, such as regulating the size of our organs, but also has been implicated in the abnormal cell growth seen in cancer.
A look at diabetes
To see the drug in context, the researchers tested simvastatin on diabetic mice. Diabetes causes subtle changes to blood vessels that mimic the damage commonly seen in people who are prescribed statins — older patients who do not have a cardiovascular condition, Liu said.
They found that after eight weeks on simvastatin, the diabetic mice had significantly improved vascular function, with arteries that more easily relaxed and contracted.
“If we can understand the mechanism, we can fine-tune this drug to be more specific to rescuing vascular function,” Liu said.
The findings also provide a more detailed picture of the vascular disease process, which could help doctors identify and treat early signs of vascular damage.
“I’ve been taking statins for the past 10 years to keep my cholesterol down. I also knew it has good vascular effects. I just didn’t know how it does it,” said Wu, the Simon H. Stertzer, MD, Professor who is also the director of the Stanford Cardiovascular Institute. “This study explains how.”
Researchers from the University of North Texas and the Ohio State University College of Medicine contributed to this study.
The study was supported by funding from the National Institutes of Health (grants R01 HL130020, R01 HL150693, R01 HL163680, R01 HL145676, P01 HL141084, R01 HL141371, R01 HL126527, R01 HL15864, R01 HL161002, R01 HL155282 and 18CDA34110293), an American Heart Association SFRN grant, an AHA Career Development Award and the Tobacco-Related Disease Research Program.

About Stanford Medicine
Stanford Medicine is an integrated academic health system comprising the Stanford School of Medicine and adult and pediatric health care delivery systems. Together, they harness the full potential of biomedicine through collaborative research, education and clinical care for patients. For more information, please visit med.stanford.edu .
Hope amid crisis
Psychiatry’s new frontiers


Image credit: Shutterstock
New study shows muscle pain is not due to statins in over 90% of those taking the treatment
Statin therapies are not the cause of muscle pain in over 90% of those who experience symptoms, according to a new study led by researchers from Oxford Population Health. The results were published today in The Lancet and presented at the European Society of Cardiology Congress.
The study demonstrated that muscle pain or weakness is common in adults, regardless of whether they take a statin tablet or not. 14 out of 15 reported cases of muscle pain or weakness were not due to statin therapy, and those cases that were due to statins occurred mainly within the first year of treatment.
The researchers gathered together data from 23 large-scale randomised studies from the Cholesterol Treatment Trialists’ Collaboration, including information from almost 155,000 individuals. They used this information to assess the effect of statin treatments on the frequency of muscle-related symptoms across many different types of patient, and found that muscle symptoms such as muscle pain or weakness were common, even in those allocated a placebo (or dummy) tablet. In 19 trials of statin therapy versus placebo, similar numbers of people reported such symptoms (16,835; 27.1%) in the statin group and (16,446; 26.6%) in the placebo group.
They also found that statin treatments marginally increased the frequency of muscle-related symptoms. In those taking statins, about 14 out of 15 reports of muscle symptoms were not attributed to statins, falling to about 9 in 10 for patients taking a high intensity treatment. This means that statins are not the cause of muscle pain in over 90% of people who report symptoms.
Most of the reports of muscle symptoms in those taking statins occurred within the first year of treatment. After the first year of starting treatment, low/moderate intensity statin therapy caused no increase in the frequency of muscle symptoms.
Higher intensity statin treatments (those designed to produce greater reductions in low‑density lipoprotein (LDL) cholesterol) were more likely than low/moderate intensity statins to increase the risk of muscle symptoms with some persistent effect after the first year. (Overall low/moderate intensity regimens yielded a 3% increase in first reports, with higher intensity regimens resulting in an 8% increase in first reports.) There was no evidence of a relationship between the statin dose and muscle symptoms.
For every 1000 people taking a moderate intensity statin, the treatment would cause 11 (generally mild) episodes of muscle pain or weakness. This means that the slightly increased risk of muscle symptoms is greatly outweighed by the previously known benefits of statin therapy in preventing cardiovascular disease, including heart attacks and strokes. For example, for every 1000 people taking a moderate intensity statin, the treatment would typically prevent 50 major vascular events (such as heart attacks and strokes) in those with pre-existing vascular disease (secondary prevention), and 25 major vascular events if used for primary prevention.
Professor Colin Baigent , Director of the Medical Research Council Population Health Research Unit at the University of Oxford, and joint lead author of the study, said ‘Cardiovascular disease including heart attacks and strokes, is the world’s largest killer, responsible for around 18 million deaths each year. High levels of LDL (‘bad’) cholesterol are a major risk factor. Statins lower LDL-cholesterol levels and have been repeatedly proven to reduce the risk of cardiovascular disease. However, there have been concerns about muscle pain, and statins can, rarely, cause severe muscle problems.
‘Our research shows that, for most people taking a statin, any muscle-related symptoms they experience will not in fact be due to the statin itself – and so the potential benefits of statin therapy are likely to outweigh the muscle pain risks. Previous reports that statins are a major cause of muscle pain are likely to have been the result of methodological problems in the studies giving rise to those reports.
Dr Christina Reith , Senior Clinical Research Fellow at Oxford Population Health and joint lead author of the study, said: ‘Rates of cardiovascular disease are rising rapidly, particularly in low- and middle-income countries. Statin therapies are affordable and widely available, and are a key tool in helping to prevent avoidable disability and death. We hope that these results will help doctors and patients to make informed decisions about whether to start or remain on statin therapy and that information provided to doctors and patients will be reviewed in light of our study results.’
All of the trials included in the analysis were large-scale (involving at least 1000 participants) and of reasonably long duration (tracking patient outcomes for at least two years). The trials were also all double-blind, meaning that neither the trial participants nor those managing the participants or leading the study knew who was receiving which treatment, to avoid potential biases due to knowledge of treatment allocation.
In 19 of the trials, participants were randomly allocated to receive either statin treatment or a placebo, whilst in four trials the comparison was of higher doses of statins versus lower/moderate doses. Around 124,000 participants (average age 63 years) were involved in the 19 trials comparing statins to a placebo.
The researchers looked at all data about any adverse effects reported by individuals taking part in the clinical trials, as well as data on the timing of and reasons for stopping study treatment, use of other (non-trial) medications, other health conditions, and laboratory results that would help in the interpretation of particular adverse events.
Professor Sir Nilesh Samani, Medical Director at the British Heart Foundation, which co-funded the study said: ‘This accumulation of data from many clinical trials provides a clear picture that while statins are associated with a small increase in risk of muscle pains or weakness, they do not cause the majority of muscle pain symptoms commonly associated with them. It reinforces the evidence that statins are safe, which should provide reassurance to the many people taking, or considering taking, these lifesaving drugs that have been proven to protect against heart attacks and strokes.
‘However, it also shows how common muscle pain symptoms are. Almost one quarter of patients who participated in the trials reported such symptoms whether they were taking statins or placebo. It is vital that the genuine concerns of people who do experience muscle symptoms are not dismissed and that doctors have continued consultations with these patients to ensure their medication is tailored to work best for them.’
The study was conducted by the Cholesterol Treatment Trialists’ (CTT) Collaboration , a joint initiative coordinated between the National Health and Medical Research Council Clinical Trials Centre, University of Sydney, Australia and the Clinical Trial Service Unit & Epidemiological Studies Unit, Oxford Population Health, on behalf of academic researchers representing major statin trials worldwide. The work was funded by the British Heart Foundation, UK Medical Research Council, and the Australian National Health and Medical Research Council. The work of the CTT is overseen by an Independent Oversight Panel.
The full paper, ' Effect of statin therapy on muscle symptoms: an individual participant data meta-analysis of large-scale, randomised, double-blind trials ', can be read in The Lancet.
DISCOVER MORE
- Support Oxford's research
- Partner with Oxford on research
- Study at Oxford
- Research jobs at Oxford
You can view all news or browse by category
Appointments at Mayo Clinic
Statin side effects: weigh the benefits and risks.
Statins are effective at lowering cholesterol and protecting against a heart attack and stroke, although they may lead to side effects for some people.
Health care professionals often prescribe statins for people with high cholesterol. Statins help lower total cholesterol and reduce the risk of a heart attack or stroke.
Statins include atorvastatin (Lipitor), fluvastatin (Lescol XL), lovastatin (Altoprev), pitavastatin (Livalo), pravastatin, rosuvastatin (Crestor) and simvastatin (Zocor).
Having too much cholesterol in the blood increases the risk of heart attacks and strokes. Statins block an enzyme the liver needs to make cholesterol. This causes the liver to remove cholesterol from the blood.
While statins are highly effective and safe for most people, they have been linked to muscle pain, digestive problems and mental fuzziness in some people. Rarely, they may cause liver damage.
If you think you're experiencing side effects from taking statins, don't just stop taking the pills. Talk to your health care team to see if a change in how much medicine you take or even a different type of medicine might be helpful.
What are statin side effects?
Muscle pain and damage.
One of the most common complaints of people taking statins is muscle pain. You may feel this pain as a soreness, tiredness or weakness in your muscles. The pain can be a mild discomfort, or it can be serious enough to make it hard to do your daily activities.
However, researchers have found a "nocebo" effect when it comes to people thinking they have muscle pain from statins. A "nocebo" effect means people who have negative expectations about a medicine report experiencing the potential side effect at higher rates than the drug should cause.
The real risk of developing muscle pain as a result of taking statins is about 5% or less compared with taking a pill that doesn't contain medicine, called a placebo. However, studies have found that nearly 30% of people stopped taking the pills because of muscle aches even when they were taking a placebo.
A strong predictor of if you'll experience muscle aches when taking statins could be whether or not you read about the potential side effect.
Very rarely, statins can cause life-threatening muscle damage called rhabdomyolysis (rab-doe-my-OL-ih-sis). Rhabdomyolysis can cause extreme muscle pain, liver damage, kidney failure and death. The risk of very serious side effects is extremely low. Only a few cases of rhabdomyolysis occur per million people taking statins. Rhabdomyolysis can occur when you take statins in combination with certain drugs or if you take a high dose of statins.
Liver damage
Occasionally, statin use could cause an increase in the level of enzymes in the liver. These enzymes signal inflammation. If the increase is only mild, you can continue to take the drug. Rarely, if the increase is severe, you may need to try a different statin.
Although liver problems are rare, your health care team may order a liver enzyme test before or shortly after you begin to take a statin. You won't need any further liver enzyme tests unless you begin to have symptoms of trouble with your liver.
Contact your health care professional immediately if you have unusual fatigue or weakness, loss of appetite, pain in your upper stomach, dark-colored urine, or yellowing of your skin or eyes.
Increased blood sugar or type 2 diabetes
It's possible that your blood sugar level, known as blood glucose, may increase when you take a statin. This may lead to developing type 2 diabetes. The risk is small but important enough that the Food and Drug Administration (FDA) has issued a warning on statin labels regarding blood glucose levels and diabetes.
The increase generally occurs when blood sugar levels are already higher than normal. People with prediabetes or diabetes may see their blood sugar levels rise when they start taking a statin.
But statins also prevent heart attacks in people with diabetes. The benefit of taking statins likely outweighs the small risk to have the blood sugar level go up. Talk to your health care team if you have concerns.
Neurological side effects
The FDA warns on statin labels that some people have developed memory loss or confusion while taking statins. These side effects reverse once you stop taking the medicines. There is limited evidence to prove a cause-effect relationship and several studies have found that statins have no effect on memory. Talk to your care team if you experience memory loss or confusion while taking statins.
There also has been evidence that statins may help with brain function — in people with dementia, for example. This is still being studied. Don't stop taking your statin medicine before talking to your health care professional.
Who's at risk of developing statin side effects?
Not everyone who takes a statin will have side effects, but some people may be at a greater risk. Risk factors include:
- Taking multiple medicines to lower your cholesterol.
- Taking medicines that interact with statins.
- Being female.
- Having a smaller body frame.
- Being age 80 or older.
- Having kidney or liver disease.
- Drinking too much alcohol.
- For some statins, drinking too much grapefruit juice.
- Having certain conditions such as hypothyroidism or neuromuscular disorders including amyotrophic lateral sclerosis (ALS).
Food and drugs that interact with statins
Grapefruit juice has a chemical that can interfere with the enzymes that break down the statins in your digestive system. While you won't need to cut grapefruit entirely from your diet, ask your health care expert about how much grapefruit you can have.
Some medicines that may interact with statins and increase your risk of side effects include:
- Amiodarone (Pacerone), a medicine for irregular heart rhythms.
- Gemfibrozil (Lopid), another variety of cholesterol drug.
- HIV treatments called protease inhibitors such as saquinavir and ritonavir (Norvir).
- Some antibiotic and antifungal medicines, such as clarithromycin and itraconazole (Sporanox).
- Some immunosuppressant medicines, such as cyclosporine (Sandimmune).
There are many drugs that may interact with statins, so be sure your health care professional is aware of all the medicines you take before starting with statins.
How to relieve statin side effects
To relieve side effects believed to be caused by statins, your health care team may recommend several options. Discuss these steps with your care team before trying them:
- Take a brief break from statin therapy. Sometimes it's hard to tell whether the muscle aches or other problems you're having are statin side effects or just part of the aging process. Taking a break can help you decide whether your aches and pains are due to statins or something else.
- Switch to another statin drug. It's possible, although unlikely, that one particular statin may cause side effects for you while another statin won't. It's thought that simvastatin (Zocor) may be more likely to cause muscle pain as a side effect than other statins when it's taken at high doses.
- Change your dose. Lowering your dose may reduce some of your side effects, but it may also reduce some of the cholesterol-lowering benefits your medicine has. Another option is to take the medicine every other day, especially if you take a statin that stays in the blood for several days. Talk to your health care professional to determine if this is appropriate for you.
- Take it easy when exercising. If you aren't used to exercising, this might increase your risk of muscle injury. It's best to make changes in your exercise routine gradually. Exercise causes muscle pain too, so it is sometimes difficult to know if the pain comes from the statin or the exercise in someone who just started an exercise program.
- Consider other cholesterol-lowering medicines. Although statins are the most effective medicines for lowering your cholesterol, other types of drugs also are available. Sometimes, taking a combination of cholesterol drugs can provide the same result with lower doses of statins.
- Try coenzyme Q10 supplements. Coenzyme Q10 supplements may help prevent statin side effects in some people, though more studies are needed to determine any benefits of taking it. Talk to your health care professional first to make sure the supplement won't interact with any of your other medicines.
Weigh the risks and benefits
Although side effects believed to be caused by statins can be annoying, consider the benefits of taking a statin before you decide to stop taking your medicine. Remember that statins can lower your risk of a heart attack or stroke, and the risk of life-threatening side effects from statins is very low.
If you have read about the potential side effects of statins, you may be more likely to blame your symptoms on the medicine, whether or not they're truly caused by the drug.
Even if your side effects are frustrating, don't stop taking your statin medicine without talking to your health care professional first. Your care team may be able make a different treatment plan that can help you lower your cholesterol without uncomfortable side effects.
There is a problem with information submitted for this request. Review/update the information highlighted below and resubmit the form.
From Mayo Clinic to your inbox
Sign up for free and stay up to date on research advancements, health tips, current health topics, and expertise on managing health. Click here for an email preview.
Error Email field is required
Error Include a valid email address
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
Thank you for subscribing!
You'll soon start receiving the latest Mayo Clinic health information you requested in your inbox.
Sorry something went wrong with your subscription
Please, try again in a couple of minutes
- Controlling cholesterol with statins. Food and Drug Administration. https://www.fda.gov/consumers/consumer-updates/controlling-cholesterol-statins. Accessed March 7, 2023.
- Rosenson RS. Statins: Actions, side effects and administration. https://www.uptodate.com/contents/search. Accessed March 7, 2023.
- Rosenson RS, et al. Statin muscle-related adverse events. https://www.uptodate.com/contents/search. Accessed March 7, 2023.
- Ferri FF. Statin-induced muscle syndromes. In: Ferri's Clinical Advisor 2023. Elsevier; 2023. https://www.clinicalkey.com. Accessed March 7, 2023.
- Blood cholesterol. National Heart, Lung, and Blood Institute. https://www.nhlbi.nih.gov/health/blood-cholesterol. Accessed March 7, 2023.
- US Preventive Services Task Force, et al. Statin use for the primary prevention of cardiovascular disease in adults: US Preventive Services Task Force Recommendation Statement. JAMA. 2022; doi:10.1001/jama.2022.13044.
- South-Paul JE, et al., eds. Dyslipidemias. In: Current Diagnosis & Treatment: Family Medicine. 5th ed. McGraw Hill; 2020. https://accessmedicine.mhmedical.com. Accessed March 7, 2023.
- What is cholesterol? American Heart Association. https://www.heart.org/en/health-topics/cholesterol/about-cholesterol. Accessed March 7, 2023.
- AskMayoExpert. Statin intolerance. Mayo Clinic; 2022.
- Libby P, et al., eds. Lipoprotein disorders and cardiovascular disease. In: Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 12th ed. Elsevier; 2022. https://www.clinicalkey.com. Accessed March 7, 2023.
- van Hunsel F, et al. Media attention and the influence on the reporting odds ratio in disproportionality analysis: An example of patient reporting of statins. Pharmacoepidemiology and Drug Safety. 2010; doi:10.1002/pds.1865.
- Levenson JL. Psychological factors affecting other medical conditions: Management. https://www.uptodate.com/contents/search. Accessed May 16, 2023.
Products and Services
- Nutritional Supplements at Mayo Clinic Store
- A Book: Mayo Clinic Family Health Book, 5th Edition
- Newsletter: Mayo Clinic Health Letter — Digital Edition
- Arcus senilis: A sign of high cholesterol?
- Birth control pill FAQ
- Cholesterol level: Can it be too low?
- Cholesterol medications: Consider the options
- Cholesterol ratio or non-HDL cholesterol: Which is most important?
- Cholesterol test kits: Are they accurate?
- Cholesterol: Top foods to improve your numbers
- Cholesterol-lowering supplements may be helpful
- Coconut oil: Can it cure hypothyroidism?
- Congenital adrenal hyperplasia
- Prickly pear cactus
- Eggs and cholesterol
- Fasting diet: Can it improve my heart health?
- Hashimoto's disease
- HDL cholesterol: How to boost your 'good' cholesterol
- Herbal supplements and heart drugs
- High cholesterol
- High cholesterol in children
- High cholesterol treatment: Does cinnamon lower cholesterol?
- Hypothyroidism: Can calcium supplements interfere with treatment?
- Hypothyroidism diet
- Hypothyroidism and joint pain?
- Hypothyroidism: Should I take iodine supplements?
- Hypothyroidism symptoms: Can hypothyroidism cause eye problems?
- Hypothyroidism (underactive thyroid)
- Lowering Triglycerides
- Menus for heart-healthy eating
- Metabolic syndrome
- Niacin overdose: What are the symptoms?
- Niacin to improve cholesterol numbers
- Nuts and your heart: Eating nuts for heart health
- Is there a risk of rhabdomyolysis from statins?
- Soy: Does it reduce cholesterol?
- Soy: Does it worsen hypothyroidism?
- Statins: Do they cause ALS?
- Lifestyle changes to improve cholesterol
- Triglycerides: Why do they matter?
- VLDL cholesterol: Is it harmful?
- Mayo Clinic Minute: Out of shape kids and diabetes
- Mayo Clinic Minute: Weight loss surgery for kids
Mayo Clinic does not endorse companies or products. Advertising revenue supports our not-for-profit mission.
- Opportunities
Mayo Clinic Press
Check out these best-sellers and special offers on books and newsletters from Mayo Clinic Press .
- Mayo Clinic on Incontinence - Mayo Clinic Press Mayo Clinic on Incontinence
- The Essential Diabetes Book - Mayo Clinic Press The Essential Diabetes Book
- Mayo Clinic on Hearing and Balance - Mayo Clinic Press Mayo Clinic on Hearing and Balance
- FREE Mayo Clinic Diet Assessment - Mayo Clinic Press FREE Mayo Clinic Diet Assessment
- Mayo Clinic Health Letter - FREE book - Mayo Clinic Press Mayo Clinic Health Letter - FREE book
- Statin side effects Weigh the benefits and risks
Your gift holds great power – donate today!
Make your tax-deductible gift and be a part of the cutting-edge research and care that's changing medicine.

New study suggests benefit-to-harm balance of statins for healthy adults “generally favourable”
Findings should reassure patients and should not deter their use, say researchers
Statins are associated with a small increased risk of side effects in patients without a history of heart disease, but these effects are mild compared with the potential benefits of treatment in preventing major cardiovascular events, say researchers in The BMJ today.
They say their findings suggest that the benefit-to-harm balance of statins for adults without heart disease is generally favourable.
Statins are widely used to prevent heart disease, and severe side effects are rare, but many people are reluctant to take them because of the potential for milder effects such as muscle weakness and stiffness.
For people with existing heart disease, the benefits of statins far outweigh the risk of these effects, but when statins are used by people without a history of heart disease (known as primary prevention) the benefit-to-harm balance of treatment might be less favourable.
Yet recent guidelines have recommended wider use of statins for primary prevention.
So, a team of UK and US researchers set out to examine the associations between statins and adverse events in adults without a history of heart disease, and how they vary by type and dose of statins.
They analysed the results of 62 randomised controlled trials with 120,456 participants (average age 61; 40% women) followed up for an average of 3.9 years. The trials were designed differently, and were of varying quality, but the researchers were able to allow for that in their analysis.
Statins were associated with a slightly increased risk of self-reported muscle pain, liver and kidney problems, and certain eye conditions such as cataracts, but were not associated with clinically confirmed muscle disorders or diabetes.
These risks equated to 15 more instances of muscle symptoms, eight more liver events, 12 more kidney events, and 14 more eye conditions per 10,000 patients treated for a year.
However, these increased risks did not outweigh the reduction in the risk of major cardiovascular events. For example, statins were estimated to prevent 19 heart attacks, nine strokes, and eight deaths from cardiovascular disease per 10,000 patients treated for a year.
This suggests that the benefit-to-harm balance of statins for primary prevention of cardiovascular disease is favourable, say the researchers.
Analyses by type of statin showed that atorvastatin, lovastatin, and rosuvastatin were associated with some adverse events, but few significant differences were seen between the statins.
A possible modest dose-response relationship was identified for the effect of atorvastatin on liver dysfunction, but the dose-response relationships for the other types of statins and adverse effects were inconclusive.
This suggests that tailoring statin doses to deal with safety concerns when starting treatment is not currently needed, the researchers add.
This was a large study that was able to accurately assess the adverse effects of treatment with statins. But the researchers point to some limitations in trial design that may have led to events being underestimated or more severe long term events being missed.
However, they say the low risk of adverse events caused by statins reported in this review “should reassure patients and physicians that the potential harms of statins are small and should not deter their use for primary prevention of cardiovascular disease.”
They agree that routine monitoring of liver function during treatment is probably warranted in primary prevention, and say further studies are needed to help improve adherence to treatment and achieve more efficient monitoring.
[Ends] 14/07/21
Notes for editors Research: Associations between statins and adverse events in primary prevention of cardiovascular disease: systematic review with pairwise, network, and dose-response meta-analyses Journal: The BMJ
Funding: British Heart Foundation
Link to Academy of Medical Sciences press release labelling system: https://press.psprings. co.uk/AMSlabels.pdf
Peer reviewed? Yes Evidence type: Systematic review and meta-analysis Subjects: People
BMJ Expert Media Panel
If you are a journalist needing to speak to an expert, please click here.
BMJ IN THE NEWS
Latest coverage of BMJ in the national and international media
JOIN OUR MEDIA LIST
If you are a journalist who would like to receive our press releases, please provide your details.
CONTACT OUR MEDIA RELATIONS TEAM
Email the UK media relations team for more information.
New study suggests benefit-to-harm balance of statins for healthy adults 'generally favorable'
Findings should reassure patients and should not deter their use, say researchers.
Statins are associated with a small increased risk of side effects in patients without a history of heart disease, but these effects are mild compared with the potential benefits of treatment in preventing major cardiovascular events, say researchers in The BMJ today.
They say their findings suggest that the benefit-to-harm balance of statins for adults without heart disease is generally favourable.
Statins are widely used to prevent heart disease, and severe side effects are rare, but many people are reluctant to take them because of the potential for milder effects such as muscle weakness and stiffness.
For people with existing heart disease, the benefits of statins far outweigh the risk of these effects, but when statins are used by people without a history of heart disease (known as primary prevention) the benefit-to-harm balance of treatment might be less favourable.
Yet recent guidelines have recommended wider use of statins for primary prevention.
So, a team of UK and US researchers set out to examine the associations between statins and adverse events in adults without a history of heart disease, and how they vary by type and dose of statins.
They analysed the results of 62 randomised controlled trials with 120,456 participants (average age 61; 40% women) followed up for an average of 3.9 years. The trials were designed differently, and were of varying quality, but the researchers were able to allow for that in their analysis.
Statins were associated with a slightly increased risk of self-reported muscle pain, liver and kidney problems, and certain eye conditions such as cataracts, but were not associated with clinically confirmed muscle disorders or diabetes.
These risks equated to 15 more instances of muscle symptoms, eight more liver events, 12 more kidney events, and 14 more eye conditions per 10,000 patients treated for a year.
However, these increased risks did not outweigh the reduction in the risk of major cardiovascular events. For example, statins were estimated to prevent 19 heart attacks, nine strokes, and eight deaths from cardiovascular disease per 10,000 patients treated for a year.
This suggests that the benefit-to-harm balance of statins for primary prevention of cardiovascular disease is favourable, say the researchers.
Analyses by type of statin showed that atorvastatin, lovastatin, and rosuvastatin were associated with some adverse events, but few significant differences were seen between the statins.
A possible modest dose-response relationship was identified for the effect of atorvastatin on liver dysfunction, but the dose-response relationships for the other types of statins and adverse effects were inconclusive.
This suggests that tailoring statin doses to deal with safety concerns when starting treatment is not currently needed, the researchers add.
This was a large study that was able to accurately assess the adverse effects of treatment with statins. But the researchers point to some limitations in trial design that may have led to events being underestimated or more severe long term events being missed.
However, they say the low risk of adverse events caused by statins reported in this review "should reassure patients and physicians that the potential harms of statins are small and should not deter their use for primary prevention of cardiovascular disease."
They agree that routine monitoring of liver function during treatment is probably warranted in primary prevention, and say further studies are needed to help improve adherence to treatment and achieve more efficient monitoring.
- Cholesterol
- Heart Disease
- Multiple Sclerosis Research
- Diseases and Conditions
- Multiple Sclerosis
- Alzheimer's
- COX-2 inhibitor
- Deep brain stimulation
- Personalized medicine
- Heart failure
- Psychopharmacology
Story Source:
Materials provided by BMJ . Note: Content may be edited for style and length.
Journal Reference :
- Ting Cai, Lucy Abel, Oliver Langford, Genevieve Monaghan, Jeffrey K Aronson, Richard J Stevens, Sarah Lay-Flurrie, Constantinos Koshiaris, Richard J McManus, F D Richard Hobbs, James P Sheppard. Associations between statins and adverse events in primary prevention of cardiovascular disease: systematic review with pairwise, network, and dose-response meta-analyses . BMJ , 2021; n1537 DOI: 10.1136/bmj.n1537
Cite This Page :
Explore More
- New-To-Nature Enzyme Containing Boron Created
- New Target for Potential Leukemia Therapy
- 'Wraparound' Implants for Spinal Cord Injuries
- Climate May Influence Seismic Activity
- Atmosphere Surrounding Super-Earth?
- How Continents Stabilized
- Pressure to Be 'Perfect' Causing Burnout
- New Type of Memory State
- Mini-Robots to Clean Up Microplastics, Microbes
- Sound-Suppressing Silk Can Create Quiet Spaces
Trending Topics
Strange & offbeat.
- Skip to main content
- Keyboard shortcuts for audio player
Your Health
- Treatments & Tests
- Health Inc.
- Public Health
Statins vs. supplements: New study finds one is 'vastly superior' to cut cholesterol

Allison Aubrey

Millions of Americans are prescribed statins to reduce the risk of heart disease, but many prefer to take supplements like fish oil, garlic and flaxseed. Peter Dazeley/Getty Images hide caption
Millions of Americans are prescribed statins to reduce the risk of heart disease, but many prefer to take supplements like fish oil, garlic and flaxseed.
If you were prescribed medicine to lower your risk of a heart attack or stroke, would you take it?
Millions of Americans are prescribed statins such as Lipitor, Crestor or generic formulations to lower their cholesterol. But lots of people are hesitant to start the medication.
Some people fret over potential side effects such as leg cramps, which may be — or may not be — linked to the drug. As an alternative, dietary supplements, often marketed to promote heart health, including fish oil and other omega-3 supplements (omega-3s are essential fatty acids found in fish and flaxseed), are growing in popularity .
So, which is most effective? Researchers at the Cleveland Clinic set out to answer this question by comparing statins to supplements in a clinical trial. They tracked the outcomes of 190 adults, ages 40 to 75. Some participants were given a 5 mg daily dose of rosuvastatin, a statin that is sold under the brand name Crestor for 28 days. Others were given supplements, including fish oil, cinnamon, garlic, turmeric, plant sterols or red yeast rice for the same period.

Choose the best diet for you
The maker of Crestor, Astra Zeneca sponsored the study, but the researchers worked independently to design the study and run the statistical analysis.
"What we found was that rosuvastatin lowered LDL cholesterol by almost 38% and that was vastly superior to placebo and any of the six supplements studied in the trial," study author Luke Laffin, M.D. of the Cleveland Clinic's Heart, Vascular & Thoracic Institute told NPR. He says this level of reduction is enough to lower the risk of heart attacks and strokes. The findings are published in the Journal of the American College of Cardiology .
"Oftentimes these supplements are marketed as 'natural ways' to lower your cholesterol," says Laffin. But he says none of the dietary supplements demonstrated any significant decrease in LDL cholesterol compared with a placebo. LDL cholesterol is considered the 'bad cholesterol' because it can contribute to plaque build-up in the artery walls – which can narrow the arteries, and set the stage for heart attacks and strokes.
"Clearly, statins do what they're intended to do," the study's senior author Steve Nissen, a cardiologist and chief academic officer of the Heart, Vascular & Thoracic Institute at Cleveland Clinic told NPR. By comparison, he says this research shows that supplements are not effective. "They do not promote heart health. They do not improve levels of the bad cholesterol."
Nissen says supplements can be expensive compared to statin medications. Depending on insurance, he says people may pay less than $5 a month out-of-pocket for rosuvastatin.

Shots - Health News
Cholesterol provides a clue about heart risks from sleep apnea.
"Statins are the most effective heart attack and stroke prevention drugs that we have really ever seen," says Michael Honigberg , a cardiologist and researcher at Massachusetts General Hospital who is not affiliated with the new study. He says the new findings add to an already large body of evidence showing statins lower LDL cholesterol, and he's not surprised to see that the supplements were not as effective.
However, he says, not everyone with a family history of heart disease or slightly elevated cholesterol should be on a statin. The American College of Cardiology and American Heart Association developed some prescription guidelines. Typically, if a person's LDL cholesterol (bad cholesterol) is 190 or higher, they're often advised to start a statin. Health care professionals use a risk calculator to estimate a person's risk of having a heart attack or stroke over the next 10 years. If the risk is high enough, based on factors including age, blood pressure and smoking status, then a statin may be recommended.
Honigberg says for people who have slightly elevated cholesterol, but are not at high enough risk to be prescribed a statin, he recommends that they focus on diet and exercise, rather than buying supplements. "I tell my patients to save their money and instead spend that money on eating heart healthy, high quality food."
He points to studies that show heart-healthy diets, including Mediterranean diets which emphasize healthy fats, lots of fruits, vegetables and whole grains and the DASH diet , significantly reduce the risk of heart disease. "I think a formulation that we perhaps don't use enough is that food is medicine and is probably a more effective medicine than supplements," says Honigberg.
The National Center for Complementary and Integrative Health, part of the National Institutes of Health, has also concluded, based on prior research, that omega-3 supplements do not reduce the risk of heart disease , but eating fish – which contains omega-3 fatty acids – is linked to a reduced risk. This suggests that omega-3 fatty acids are most beneficial as part of a healthy diet.
And it's worth noting that the NIH review concludes that omega-3 supplements may help relieve symptoms of rheumatoid arthritis. Omega-3s are also added to baby formulas to promote brain development. The NIH review also concludes that omega-3 supplements can lower triglycerides, a type of fat found in the blood. But Honigberg says this may be recommended for a "small subset of patients" with very high triglyceride levels.
As for people whose risk of heart disease is high enough to warrant a statin prescription, Honigberg says he spends a fair amount of time talking through concerns with patients.
"We talk about the excellent safety profile and the very, very low risk of side effects," he says. He describes the risk of serious side effects as "vanishingly small."
Sometimes patients stop taking a statin because they believe it's causing a certain side effect. But Honigberg points to a double-blind research study that showed when patients were given a placebo in place of a statin, patients reported feeling most of the same side effects.
"So the punch line of the trial is people blame statins for side effects the statins aren't really causing," he says.
- supplements
- heart disease
Advertisement
Latest statin risk-benefit analysis: more harm than good, a study sought to quantify benefits and harms but in so doing may serve only to reopen old grievances, one critic insists..

- Created with Sketch.

(UPDATED) A new study seeking to allay concerns about statin side effects in primary prevention may have the unintended effect of reopening a debate that many physicians have long considered as settled, a prominent cardiologist warns.
The stated aim of the meta-analysis, published in the BMJ , is to assess the benefit-to-harm ratio of the popular cholesterol-lowering drugs, given pervasive concerns about adverse events in people who haven’t already had a cardiovascular event.
“As patients get a little bit older, the potential harms of [statins and other medications] increase, and for some it may be the case that the harms of treatment might start to outweigh the potential benefits,” senior author James Sheppard, PhD (University of Oxford, England), explained to TCTMD. “And therefore, there may be some patients who are less likely to want to take these sorts of medications.
“But the problem for doctors in clinical practice is that they don't really know who these patients might be,” Sheppard continued, “and there's not great empirical evidence at the moment to the extent to which who has different outcomes. Particularly for statins, it's become quite a controversial area where you see some study saying that statins have lots of side effects and other studies saying that statins have no side effects. It becomes quite confusing quite quickly.”
However, for Steven Nissen, MD (Cleveland Clinic, OH), who commented on the analysis for TCTMD, the study “does a serious disservice to evidence-based medicine” because the researchers don’t go far enough in their wording of the title and conclusions to promote statin use.
The study by Sheppard and colleagues, with lead author Ting Cai, MPH (University of Oxford), estimated that statins prevent 19 MIs, nine strokes, and eight CV deaths per 10,000 patients treated per year. Side effects like muscle symptoms and liver dysfunction were “really, really rare, and from what we could see, they certainly weren't on the same level as the amount of benefits that you get from taking a statin,” Sheppard said.
The authors conclude their paper saying: “Statins were associated with a small increased risk of self-reported muscle symptoms, liver dysfunction, renal insufficiency, and eye conditions in patients without a history of cardiovascular disease. These adverse effects were mild compared with the potential benefits of treatment with statins in preventing major cardiovascular events, suggesting that the benefit-to-harm balance of statins for primary prevention of cardiovascular disease is generally favorable.”
That’s too soft a stance, says Nissen.
“What I'm worried about is when you get this kind of strange study, it really has the effect of getting people who are somewhat cautious about statins to be more cautious,” he stressed. “I think we ought to be more aggressive about giving statins because we know that LDL cholesterol is in fact strongly associated with morbidity and mortality. In general, if you read the manuscript closely, they are saying that the benefits do outweigh the harms, but they are really overemphasizing the harms. These harms are not important.”
In response, Sheppard argued that the issue is not as straightforward as Nissen suggests.
“Unfortunately, many patients (rightly or wrongly) have preconceived ideas about statin treatment and the potential for harm, which stop them from accepting treatment when it is offered,” he said. “To dismiss these ideas and say that the harms are not important I think is unhelpful. In our paper, we acknowledge that these side effects are real, but also mild and very rare. I believe these data are helpful for clinicians speaking to patients who are anxious about starting statin treatment, allowing them to reassure individuals that the potential for side effects is very small, and outweighed by the potential for benefit.”
On behalf of the BMJ editors, Associate Editor Joseph Ross, MD (Yale School of Medicine, New Haven, CT), told TCTMD in an email they “made the decision to publish this study because there remains outstanding uncertainty about the risk of adverse events attributable to statins when used for the primary prevention of cardiovascular disease.
“In contrast, there have been ample studies examining the benefits,” he continued. “Our hope is that because the authors have provided the evidence for risk alongside the evidence for benefits, doing their best to meta-analyze the literature using multiple methodological approaches, patients and their primary care physicians can make more informed choices about whether to use statins for primary prevention.”
Meta-analysis Findings
For the meta-analysis, Sheppard and colleagues included 62 statin trials comprised of more than 120,000 patients without a history of cardiovascular disease who were followed for a mean of 3.9 years.
Statins were associated with greater risks of the following side effects:
- Self-reported muscle symptoms (21 trials): OR 1.06; 95% CI 1.01-1.13
- Liver dysfunction (21 trials): OR 1.33; 95% CI 1.12-1.58
- Renal insufficiency (eight trials): OR 1.14; 95% CI 1.01-1.28
- Eye conditions (six trials): OR 1.23; 95% CI 1.04-1.47
Neither clinically confirmed muscle disorders nor diabetes were shown to be related to statin use.
On the other hand, statins significantly reduced the risks of MI (OR 0.72; 95% CI 0.66-0.78), stroke (OR 0.80; 95% CI 0.72-0.89), and CV death (OR 0.83; 95% CI 0.76-0.91) in 22, 17, and 22 trials, respectively.
“The population we looked at here were people who were at low risk of having a cardiovascular event, so the chances of benefitting from a statin were lower,” Sheppard said. “In this population, you might think actually if there were a risk you might be more cautious about starting a statin, but what we show in the results is that actually the harms associated with statins are so small that is still beneficial to take a statin even if you are at low risk of cardiovascular disease.”
What this analysis wasn’t able to show, however, is which patients are most likely to experience side effects and why, he added, saying this is where future research should focus.
Nissen also took issue with the term “liver dysfunction” used in the study, defined as a rise in serum concentration of aspartate transaminase or alanine transaminase to more than three times the upper limit of normal and other diagnosed liver disorders. “What actually happens with statins is there's a modest increase in liver enzymes that never leads to liver dysfunction,” he said. “So it's not liver dysfunction. It's isolated enzyme increases.”
Ultimately, to say statins are “generally favorable” is “an awfully weak statement of support,” Nissen said. “It's just bizarre that they would conclude that there's not clearly a benefit over a harm.”
Correction: When this story was first published, in 2021, the data in paragraph 6 were inadvertently reported as absolute reductions in risk, rather than absolute risk differences. The data have now been corrected.

Yael L. Maxwell is Senior Medical Journalist for TCTMD and Section Editor of TCTMD's Fellows Forum . She served as the inaugural…
Disclosures
Cai T, Abel L, Langford O, et al. Associations between statins and adverse events in primary prevention of cardiovascular disease: systematic review with pairwise, network, and dose-response meta-analyses. BMJ . 2021;374:n1537.
- This study was funded by a British Heart Foundation PhD Scholarship held by Cai.
- Sheppard is funded by a Wellcome Trust/Royal Society Sir Henry Dale Fellowship, and he also reports receiving funding from a National Institute for Health Research Oxford Biomedical Research Centre Senior Fellowship.
- Nissen reports no relevant conflicts of interest.
Never Miss a Beat
Stay up-to-date with breaking news, conference slides, and topical videos covering the spectrum of CVD. Join our newsletter!
New at TCTMD? Register today!
Forgot Password
Forgot Your Password?
Enter the email you used to register to reset your password.
Search TCTMD
Sign up for our newsletter.
Sign up to receive the most important cardiovascular news, research, and major meeting presentations.
Submit an Event
Become a premium member or log in to view exclusive content.
This content is available for meeting attendees and/or Platinum Members
REGISTER for free or LOG IN to view this content

Benefits of statins may have been overstated – new study

Researcher, Medicine and Health, RCSI University of Medicine and Health Sciences
Disclosure statement
Paula Byrne does not work for, consult, own shares in or receive funding from any company or organization that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment.
RCSI University of Medicine and Health Sciences provides funding as a member of The Conversation UK.
View all partners
Cholesterol-lowering statins are one of the world’s most commonly used medicines. They were first approved for people with a high risk of cardiovascular disease in 1987. By 2020, global sales were estimated to have approached US$1 trillion (£764 billion).
However, there has been an ongoing debate about whether or not statins are over-prescribed. Does everyone who takes them really benefit from them? To find out, my colleagues and I found 21 relevant clinical trials and analysed the combined data (over 140,000 participants) in what is known as a meta-analysis.
We asked two questions: is it best to lower LDL cholesterol (sometimes known as “bad” cholesterol) as much as possible to reduce the risk of heart attack, stroke or premature death? And, how do the benefits of statins compare when it comes to reducing the risk of these events?
In answer to the first question, we found a surprisingly weak and inconsistent relationship between the degree of reduction in LDL cholesterol from taking statins and a person’s chance of having a heart attack or stroke, or dying during the trial period. In some trials, reductions in LDL cholesterol were associated with significant reductions in the risk of dying, but in others, reductions in LDL cholesterol did not reduce this risk.
This is an important finding because clinical guidelines have expanded the proportion of people eligible for statins as “ideal” LDL cholesterol levels were incrementally lowered. For example, one study estimated a 600% increase in eligibility for statins between 1987 and 2016.
The proportion of people in Europe eligible for statins

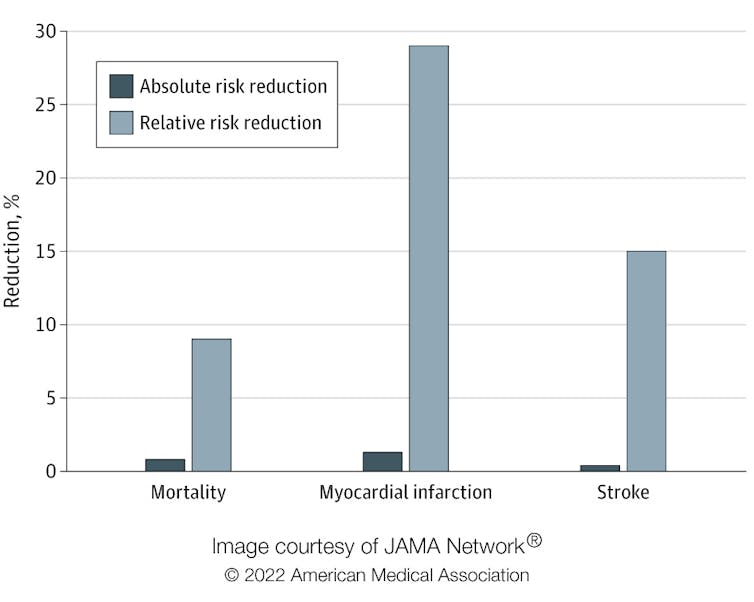
Regarding the second question, we looked at two types of risk reduction: relative risk reduction and absolute risk reduction. Imagine your chance of dying from a certain condition prematurely is 0.2%, and there’s a drug that reduces your chance of dying to 0.1%. In relative terms (relative risk reduction), your chance of dying has been halved, or reduced by 50%. But in absolute terms (absolute risk reduction), your chance of dying has only gone down by 0.1%.
Although there is a 50% relative risk reduction, is it a meaningful difference? Would it be worthwhile changing to this drug, particularly if there are side-effects associated with it? Absolute risk reduction presents a clearer picture and makes it easier for people to make informed decisions.
In our study, published in Jama Internal Medicine , we found that the absolute risk reduction from taking statins was modest compared with the relative risk reduction. The relative risk reduction for those taking statins compared with those who did not was 9% for deaths, 29% for heart attacks and 14% for strokes. Yet the absolute risk reduction of dying, having a heart attack or stroke was 0.8%, 1.3% and 0.4% respectively.
Absolute risk reduction compared with relative risk reduction
Individual differences
A further consideration is that trials report average outcomes across all included participants rather than for an individual. Clearly, people’s individual risk of disease varies depending on lifestyle and other factors. The baseline risk of cardiovascular disease can be estimated using an online calculator, such as QRisk , which takes a range of factors into account, such as weight, smoking, blood pressure, cholesterol and age.
The likelihood of a person developing cardiovascular disease in the next ten years is expressed as a percentage. For example, consider an overweight 65-year-old man who smokes, has high blood pressure and total cholesterol. He may be at high risk of cardiovascular disease, compared with a 45-year-old, non-smoking woman with slightly raised cholesterol and blood pressure and no other risk factors. If a doctor were to assess their risk of dying in the next ten years, the estimated risk for the man might be 38%, for example, whereas the woman’s risk might be only 1.4%.
Now consider the impact of taking statins for both. According to the study, statins would reduce the relative risk of dying by 9%. In absolute terms, the man would reduce his risk from 38% to 34.6%, and the woman from 1.4% to 1.3%.
Patients and their doctors need to consider whether they think these risk reductions are worthwhile in a trade-off between potential benefits and harms, including the inconvenience of taking a daily medicine, possibly for life. This is particularly salient for low-risk people for whom the benefits are marginal. However, people perceive risk differently based on their own experience and preferences, and what might look like a “good deal” to some may be seen as of little value to others.
Our study highlights that patients and doctors need to be supported to make decisions about treatments using evidence from all available studies and presented in a format that helps them understand potential benefits. Both patients and their doctors need to understand the true impact of medicines in order to make informed decisions. Relying on relative risk, which is numerically more impressive, instead of absolute, may lead both doctors and patients to overestimate the benefits of interventions.
For example, one study found that doctors rated a treatment as more effective and were more likely to prescribe it when the benefits were presented as relative rather than as absolute risk reductions. Another survey found that most respondents would agree to be screened for cancer if presented with relative risk reductions, whereas just over half would if presented with absolute risk reductions.
If you have been prescribed statins, don’t stop taking your medication without first consulting your doctor. Your risk profile might mean that they could benefit you. But if you’d like to reassess taking this drug, ask your doctor to explain your absolute risk reduction and then make a collaborative decision.
- Cardiovascular disease
- medical risk
Want to write?
Write an article and join a growing community of more than 183,300 academics and researchers from 4,953 institutions.
Register now
- Type 2 Diabetes
- Heart Disease
- Digestive Health
- Multiple Sclerosis
- Diet & Nutrition
- Supplements
- Health Insurance
- Public Health
- Patient Rights
- Caregivers & Loved Ones
- End of Life Concerns
- Health News
- Thyroid Test Analyzer
- Doctor Discussion Guides
- Hemoglobin A1c Test Analyzer
- Lipid Test Analyzer
- Complete Blood Count (CBC) Analyzer
- What to Buy
- Editorial Process
- Meet Our Medical Expert Board
This New Drug Lowers Cholesterol Without the Side Effects of Statins
Esperion Therapeutics, Inc
Key Takeaways
- Drugs called statins have been the go-to for helping people lower their cholesterol and reduce their risk of heart disease.
- Statins alone or with lifestyle changes are not always enough to help people get their cholesterol numbers down. Even when they work, the side effects of statins—particularly muscle pain—can be enough to make people stop taking the drugs.
- A new study has shown that another drug called Nexletol (bempedoic acid) can help people lower their cholesterol and prevent heart disease without causing the muscle pain that can come with taking statins.
While some people can lower their cholesterol through lifestyle changes alone, many people need to take medication to get their levels in check. But side effects of the most commonly prescribed medications to treat high cholesterol, called statins, can be enough of a problem that people stop taking the drugs, or won’t start taking them to begin with.
According to a new study, a non-statin medication can help people lower their cholesterol and prevent heart disease without causing muscle pain, which is a major side effect of statins. The drug could also be an add-on treatment for people already takings statins. Here’s what experts want you to know about the medication and whether it could be an option for you.
Bempedoic Acid: A Statin Alternative to Reduce Cholesterol
Statins reduce heart attacks and strokes, which is why they’re first-line therapy, but those side effects can be a problem for people.
The new study, published this month in the New England Journal of Medicine, shows a drug called bempedoic acid is a promising option for patients who can’t or won’t take statins.
Bempedoic acid , sold under the brand name Nexletol, is a first-of-its-kind drug called an adenosine triphosphate-citrate lyase (ACL) inhibitor. The drug works by preventing cholesterol synthesis in the liver.
Bempedoic acid is sold under the brand name Nexletol on its own and as a combination drug with ezetimibe called Nexlizet .
To find out if the drug could safely and effectively lower cholesterol, the researchers conducted a trial with almost 14,000 patients who could not or were not willing to take statins. All of the patients had a history of or were at high risk for getting heart disease. About 7,000 of the patients took Nexletol, and the rest took a placebo.
After about three years of follow-up, the researchers found that the group who took Nexletol experienced more of a cholesterol level decrease than the placebo group—about a 21% greater drop. They also had a lower risk for certain heart health-related events, like heart attacks.
What Are the Limitations of Nexletol?
Nexletol might be safe and effective and not cause muscle pain, but it’s not without side effects and risks.
Nexletol increases uric acid in the blood, which can cause gout and gallstones. The patients in the trial who took Nexletol had a higher incidence of gout than the placebo group. People who are prone to these health problems would need to talk to their providers about whether the statin alternative would be right for them.
What Is Gout?
Gout is a painful form of arthritis defined by inflammation and the accumulation of uric acid crystals in joints. It commonly affects the big toe.
Joshua Knowles, MD, PhD , associate professor of cardiovascular medicine at Stanford Health Care , told Verywell that while statins lower LDL cholesterol , or “bad” cholesterol, by an average of 50%, Nexletol lowers LDL by 25%, so it’s not as potent.
Ezetimibe or PCSK9 inhibitors are other options for patients who can’t take statins, but they can vary in effectiveness. Plus, injectable medications like PCSK9 inhibitors tend to be more expensive than oral medications.
Why Can’t Some People Take Statins?
Muscle aches are the best-known side effect of statin drugs and the most common reason people stop taking them.
While some studies suggest that between 5%–30% of people who take statins stop because they can’t handle the side effects, Knowles said that number is probably inflated—instead, many patients stop taking statins because they’re afraid of side effects.
According to Knowles, the actual number of patients who truly cannot take statins is probably closer to 2%–5%.
“Overcoming some of the limitations of statins was the major driver for this trial,” Michael Lincoff, MD , one of the study’s authors and a cardiologist with the Cleveland Clinic, told Verywell. In his experience, patients who perceive themselves to be statin-intolerant tolerate Nexletol pretty well.
Statins and bempedoic acid act on the same pathway the body uses to form cholesterol, but bempedoic acid is only active in the liver and does not affect the muscles. Researchers think that’s why the study participants who received bempedoic acid didn’t experience muscle pain.
Can You Take Statins and Nexletol Together?
Patients with an inherited predisposition to high cholesterol called familial hypercholesterolemia (also called “familial hypercholesteremia”) may have a hard time achieving a healthy LDL level if they’re only taking one medication.
“Only half of the patients with familial hypercholesteremia achieve goal LDL cholesterol with statins alone,” Knowles said. “Many patients with familial hypercholesteremia start with an LDL of 250 or 300. If you’ve already had a heart attack or stroke, you ideally need an LDL of 70 or lower.”
According to Knowles, providers usually want to reduce a patient’s LDL by over 50% to have a positive effect on their heart disease risk, but that’s beyond what can be achieved with statins alone.
Even with lifestyle modifications and maximum statin therapy, some patients still have high LDL. For these patients, Nexletol could be an effective add-on treatment.
“Some patients, even those that don’t have familial hypercholesteremia, don’t respond as well to statins,” Knowles said. “They might only have a 30% reduction in LDL with statins, so they need additional medication options.”
What’s Next for Nexletol?
The Food and Drug Administration (FDA) actually approved Nexletol back in 2020 for familial hypercholesterolemia and for patients with confirmed heart disease, but the latest study was the first to prove that the drug could be useful for preventing heart disease.
“Our trial proves that not only does bempedoic acid reduce LDL, it also reduces cardiovascular events,” Lincoff said. “That will hopefully enhance payer coverage for the drug and increase the motivation for practitioners to prescribe it.”
With new evidence in hand, Esperio, the company that manufactures Nexletol, will be able to seek permission to update drug labels to include the benefit of lowering heart disease risk.
While the recent trial showed promising evidence that Nexletol could have a role in high cholesterol treatment , statins still have the longest track record, so providers will probably keep using them as first-line treatment.
What This Means For You
Patients who can’t (or won’t) take statins or those who need another treatment in addition to statins and lifestyle changes to lower their cholesterol might benefit from Nexletol (bempedoic acid).
Nissen SE, Lincoff AM, Brennan D, et al. Bempedoic acid and cardiovascular outcomes in statin-intolerant patients . New England Journal of Medicine . Published online March 4, 2023. doi:10.1056/nejmoa2215024
National Library of Medicine: DailyMed. Nexletol—bempedoic acid tablet, film coated [drug label] .
National Library of Medicine: MedlinePlus. Ezetimibe .
Harvard Medical School. Are statins enough? When to consider PCSK9 inhibitors .
Cheeley MK, Saseen JJ, Agarwala A, et al. NLA scientific statement on statin intolerance: a new definition and key considerations for ASCVD risk reduction in the statin intolerant patient . J Clin Lipidol . 2022;16(4):361-375. doi:10.1016/j.jacl.2022.05.068
By Cyra-Lea Drummond, BSN, RN Drummond is a registered nurse and a writer specializing in heart health, cardiac care, pediatric health, and more.
Statin alternative significantly reduces heart disease deaths, new study finds
An alternative to statins may help reduce deaths from heart disease among people with high levels of LDL, or “bad” cholesterol, new research finds.
When taken as a daily pill, bempedoic acid lowered LDL cholesterol and showed a significant 39% reduction in heart disease deaths and heart attacks, researchers reported Saturday at the American Diabetes Association’s annual meeting. The findings were simultaneously published in JAMA.
“What we saw really surprised me,” said the study’s lead author, Dr. Steven Nissen, chief academic officer of the Heart, Vascular & Thoracic Institute at the Cleveland Clinic. “I hope this will be a wake-up call for patients and physicians.”
Right now, fewer than half the people who should be prescribed a cholesterol-lowering medication because of heart disease risk are getting it, according to Nissen. That needs to change, he said.
“Treating people who have risk factors before their first cardiovascular event would have large benefits,” not just in preventing complications but also in preventing deaths, he said.
What is a healthy level of cholesterol?
Bempedoic acid, which was approved in 2020 by the Food and Drug Administration , is not as effective as statins, which are considered the gold standard in treating high cholesterol. However, many people stop or refuse to take statins because of possible side effects such as muscle pain, headaches, sleep problems and digestive problems.
Recent research found that about 20% of people at high risk for heart disease refuse to take statins when prescribed by their doctor. Women in particular were less likely to accept a statin prescription, according to the study published in JAMA Network Open.
Although the new study looked at only the impact of bempedoic acid on people who had adverse reactions to statins, it found that lowering cholesterol resulted in a significant decrease in heart attacks and heart-disease related deaths.
What's most important is to get blood cholesterol to healthy levels, whether by taking a statin or bempedoic acid or other lipid-lowering medication, Nissen said in an interview.
More on heart health
- 'Good' cholesterol may not protect against heart disease as much as thought
- Covid infection raises cholesterol levels, even in people with no prior problem
- Too many people stop their lifesaving statins, research shows
LDL, or low density lipoprotein, is the type of cholesterol that contributes to the buildup of fatty deposits in the arteries and raises the risk of cardiovascular events, such as heart attack and stroke. According to the American Heart Association , the optimal total cholesterol level for an adult is about 150 mg/dL, with LDL levels at or below 100 mg/dL.
The 4,206 patients enrolled in the new study are part of a larger group described in a New England Journal of Medicine article in March. The NEJM study included both patients who had experienced a cardiovascular event, such as a stroke or heart attack, as well as those who only had risk factors.
In the new research, Nissen and his colleagues focused only on participants who had never been diagnosed with heart disease, but were at high risk because of factors such as high LDL, diabetes and hypertension.
The average age of the participants in the new study was 68, and 59% were women. Two-thirds had diabetes. At the outset, the average LDL level in the participants was 142.5 mg/dL.
Six months into the study, compared with patients taking a placebo, participants who received a daily dose of bempedoic acid experienced a 23.2% reduction in LDL cholesterol and a 22.7% decrease in inflammation caused by a protein in the blood associated with heart and stroke risk.
Other key findings of the study, which tracked most participants for a little more than three years, showed that:
- Risk of heart attacks among people who received the medication were cut by 39%.
- Risk of heart disease-related death had been reduced by 39%.
- The combined risk of a patient dying, having a heart attack or a stroke had been cut by 36%.
There was a small increased risk of complications in those who were treated with bempedoic acid versus placebo, including the development of gout and gallstones.
Statins as 'first-line therapy'
While bempedoic acid may not cause as many muscle-related symptoms, it is more expensive than generic statins, Dr. Druv S. Kazi, a cardiologist, noted in an editorial accompanying the JAMA study.
"Patients are likely to face substantially higher out-of-pocket costs for bempedoic acid than for a generic statin," Kazi wrote.
Sheldon Koenig, CEO and president of Esperion, which makes the medication sold as Nexletol and funded the study, said the drug is now covered by many insurance companies.
“For Medicare, the company has preferred status and the copay is generally only $45 per month,” Koenig said.
The new findings are “exciting and very promising,” said Dr. Marc Eisenberg, a cardiologist and an associate professor of medicine at Columbia University’s Vagalos College of Physicians and Surgeons. “But statins should still be offered and tried as a first-line therapy.” Eisenberg was not associated with the new study.
While the study is “well designed,” Eisenberg said, “we still need more studies.”
These “are very important findings,” said Dr. Robert Rosenson, director of metabolism and lipids for the Mount Sinai Health System and a professor of medicine at the Icahn School of Medicine at Mount Sinai.
The benefits seen in the new study are greater than you would expect simply based on the reductions seen in LDL level, said Rosenson, who was not associated with the research.
The new study reinforces the idea that “targeting LDL cholesterol reduces cardiovascular risk,” said Dr. Jeffrey Berger, director of the Center for the Prevention of Cardiovascular Disease at NYU Langone Health.
Patients with risk factors, such as high LDL and diabetes, but who haven’t yet been diagnosed with cardiovascular disease “are the largest group of patients we take care of,” Berger said. Berger was not part of the new study.
For people who can’t or won't take statins, bempedoic acid offers an alternative, Berger said.
“But I do think it’s important to recognize that there are important side effects with this drug. Like everything in medicine, there are risks and benefits,” Berger said.
CORRECTION (June 25, 2023, 6:56 p.m. ET): A previous version of this article misspelled Dr. Marc Eisenberg’s affiliation. It is Columbia University Vagelos College of Physicians and Surgeons, not Columbia University’s Vegelos College of Physicians and Surgeons.
Linda Carroll is a regular health contributor to NBC News. She is coauthor of "The Concussion Crisis: Anatomy of a Silent Epidemic" and "Out of the Clouds: The Unlikely Horseman and the Unwanted Colt Who Conquered the Sport of Kings."

- Follow UNSW on LinkedIn
- Follow UNSW on Instagram
- Follow UNSW on Facebook
- Follow UNSW on WeChat
- Follow UNSW on TikTok

Treatment-related pain may be ‘socially contagious’, study finds
Photo: Getty Images

Understanding the impact of social connections on pain management could improve treatment outcomes.
An individual’s experience of pain from medical treatment can be heightened by witnessing other people’s responses to the same treatment, with this negative experience subsequently spreading to others, scientists have discovered.
You may have heard of the placebo effect – a beneficial effect produced by a patient’s positive beliefs about a treatment. The ‘nocebo’ effect describes the opposite, where negative expectations about treatment can cause harmful side effects.
New research, published recently in Communications Psychology , found that the nocebo effect has the capacity to spread beyond the original “harmful” experience, and that this is heightened in cases when the physiological response of two individuals was more similar or “synchronised”; a phenomenon associated with increased social connection.
“We found that expectations formed about a treatment can go on to influence both our self-perceived experience of that treatment as well as our physiological response to it,” says Dr Kirsten Barnes, from the School of Psychology at UNSW Sydney, and lead author on the study.
These results are significant as treatments and therapy can often occur in communal settings. In group rehabilitation sessions, or on shared hospital wards, where patients may form a connection with one another, witnessing painful treatment experiences could be particularly harmful.
The team hopes that this latest study will address gaps in our understanding of the social aspects of pain management and could be used to guide treatment decisions.
Media enquiries
For enquiries about this story and to arrange interviews please contact Lilly Matson .
Tel: 0426 656 007 Email: [email protected]

A universal human experience
Pain is a near universal human experience that comes not only from physiological processes inside our bodies, but is also influenced by psychological and social factors. In Australia, one in five people suffer from chronic pain and 80 per cent of people experience acute pain after medical interventions like surgery.
One of the primary ways we learn about the negative effects of medical intervention, such as increased pain, is through observing others.
Dr Barnes wanted to demonstrate whether observing someone experiencing the nocebo effect could cause negative expectations about that treatment to spread to another person, who then goes on to express a second nocebo effect that would transfer to someone else.
“Because if that's the case, there’s the potential for the rapid propagation of these negative treatment experiences independent of any kind of active component of a treatment itself,” says Dr Barnes.
The Experiment
The study was completed while Dr Barnes was conducting postdoctoral research at the University of Sydney and was approved by the university Human Research Ethics Committee. The team recreated a situation in the lab that enabled them to measure whether a nocebo effect was being passed down through a chain of participants. Before the experiment, participants were instructed that a treatment applied to their arm would exacerbate their experience of pain, and this was reinforced with a short handout that they read during the set-up procedure. They were also told that once the treatment was calibrated, they wouldn’t be able to feel it. Instead, a blue or green square would appear on their computer screen when the treatment was either active or inactive and they had to discover, either through demonstrating or observing, which was associated with treatment activity.
The first participant – the demonstrator – was paired with another participant who observed their reactions to the treatment. This first demonstrator was fitted with a thermode, similar to a small heat plate, which pulsed a rapid burst of heat against their skin. When the blue square was presented, the intensity of this heat was surreptitiously increased so it was noticeably more painful.
Next it was the observer’s turn to become the demonstrator, while a new participant was introduced to the experiment in the observer’s chair. The process was then repeated three times, each time with a new observer.
Unknown to the participants, the treatment was actually a sham. While the intensity of the heat was surreptitiously changed for the first demonstrator, making it appear as if the treatment was effective, an identical intensity was applied for all other demonstrators irrespective of whether they saw the green or blue square.
Interestingly, as each observer moved to the demonstrator’s chair, many reported more pain when they saw the blue square, even though the intensity of the heat delivered to their arm was identical to when they saw the green square. These participants were experiencing a nocebo effect when they believed that the treatment was active.

Measuring a nocebo effect
While this social interaction was happening, the team was recording a host of changes in the participants.
“We know that certain muscles in the face are activated during pain. We recorded activity in these muscles from both the demonstrator and observer when the ‘treatment’ was being delivered, so we could see how both were responding when they experienced or witnessed more pain to treatment,” says Dr Barnes. “We also recorded the physiological response of both the demonstrator and observer, via their skin conductance – the sweat gland activity on their fingertips.”
The team asked the demonstrator to give a self-report measure of the pain they were experiencing when they saw the blue or green square. “After analysing the results, we found that witnessing treatment-related pain exacerbated the observer’s own pain to a sham-treatment, demonstrating that nocebo effects can be transmitted socially between people and passed successively along a chain.”
Interestingly, the participants showed genuine physiological changes in their skin conductance, and their pain-related facial expressions, when they thought that they were receiving treatment. “This means that the nocebo effect is not just psychological, but can cause real changes in your body that alter the experience of pain,” says Dr Barnes.
They also found that the more ‘synchronous’ or similar the physiological response of the demonstrator and observer were during the treatment session, the larger the nocebo effect of the observer when they subsequently experienced the ‘treatment’. “While more research is needed, this suggests that those closest to us may transmit their symptoms most readily, even in the case of the nocebo effect,” says Dr Barnes.
Previous research suggests that a good patient-practitioner relationship can lead to better health outcomes. “If you’re a patient in a group setting, such as participating in group therapy or experiencing an intervention for pain, it is generally believed that having social support is a good thing,” says Dr Barnes. “But this study suggests that forming those close relationships may paradoxically end up making pain worse if you witness someone having a bad experience of treatment.”
After analysing the results, we found that witnessing treatment-related pain exacerbated the observer’s own pain to a sham-treatment, demonstrating that nocebo effects can be transmitted socially between people and passed successively along a chain. Dr Kirsten Barnes
Research in a real-life context
This work contributes more broadly to an area of research that explores how the social transmission of negative health information may be impacting our health outcomes.
“Given that our social networks are ever expanding, with personal health experiences regularly shared on social media, it is important to understand the impact of this information, especially where it may be generating negative expectations about the effects of treatment.”
While this research has provided new insight into the influence of social connections on pain management, Dr Barnes highlights the need for further research.
In this study, the team tested healthy participants and the thermal stimuli that they experienced induced transient pain that they knew would end. This is not comparable to clinical settings where the time course of pain is often unpredictable and unknown. “Ideally, data is required from real treatment contexts to better understand the nocebo effect,” says Dr Barnes.
“Results of this study do not mean that there aren't genuine active effects of treatment, or that the pain you experience is all in your head. But if we can help to reduce these negative expectations, hopefully we can minimise the experience of the nocebo effect and improve patient experiences in the future.”
Share this story
- Share this page on Email
- Share this page on Facebook
- Share this page on Twitter
- Share this page on LinkedIn
- Share this page on WhatsApp
- Share this page on FacebookMessenger
- Share this page on WeChat
- Share this page on Copy
Related stories

Surgery won’t fix my chronic back pain, so what will?

Lost for words? Research shows art therapy brings benefits for mental health

May cause side effects: how social media could be affecting COVID vaccine hesitancy

We discovered a 'gentle touch' molecule is essential for light tactile sensation in humans - and perhaps in individual cells
- Share full article
Advertisement
The Morning
The side effects of covid vaccines.
Thousands of Americans have filed vaccine-injury claims with the federal government.

By David Leonhardt
Let me start with a disclaimer: The subject of today’s newsletter will make some readers uncomfortable. It makes me a little uncomfortable.
The Times has just published an article about Americans who believe they suffered serious side effects from a Covid vaccine. More than 13,000 of them have filed vaccine-injury claims with the federal government.
My colleague Apoorva Mandavilli tells some of their stories in the article , including those of several people who work in medicine and science:
Ilka Warshawsky, a 58-year-old pathologist, said she lost all hearing in her right ear shortly after receiving a Covid booster shot.
Dr. Gregory Poland, 68 — no less than the editor in chief of Vaccine, a scientific journal — said that a loud whooshing sound in his ears had accompanied every moment since his first Covid shot.
Shaun Barcavage, 54, a nurse practitioner in New York City, has experienced a ringing sound in his ears, a racing heart and pain in his eyes, mouth and genitals for more than three years. “I can’t get the government to help me,” Barcavage said. “I am told I’m not real.”
This subject is uncomfortable because it feeds into false stories about the Covid vaccines that many Americans have come to believe — namely, that the vaccines are ineffective or have side effects that exceed their benefits. Robert F. Kennedy Jr., the independent presidential candidate, has promoted these stories, as have some Republican politicians and conservative media figures. “The scale of misinformation,” Dr. Joshua Sharfstein of Johns Hopkins University told Apoorva, “is staggering.”
So let me be clear: The benefits of the Covid vaccines have far outweighed the downsides, according to a voluminous amount of data and scientific studies from around the world. In the U.S. alone, the vaccines have saved at least several hundred thousand lives and perhaps more than one million , studies estimate. Rates of death, hospitalization and serious illness have all been much higher among the unvaccinated than the vaccinated.
Here is data from the C.D.C., in a chart by my colleague Ashley Wu:
Average weekly Covid deaths per 100,000 in the U.S.
From the weeks of Oct. 1, 2022 to April 1, 2023

Unvaccinated
to 4 years old

80 years and older
6 months to 4 years old
Not only are the vaccines’ benefits enormous, but the true toll of the side effects may be lower than the perceived toll: Experts told Apoorva that some people who believe Covid vaccines have harmed them are probably wrong about the cause of their problems.
How so? Human beings suffer mysterious medical ailments all the time. If you happened to begin experiencing one in the weeks after receiving a vaccine, you might blame the shot, too, even if it were a coincidence. So far, federal officials have approved less than 2 percent of the Covid vaccine injury-compensation claims they have reviewed.
Still, some ailments almost certainly do stem from the vaccines. The C.D.C. says some people are allergic (as is the case with any vaccine). Both the C.D.C. and researchers in Israel — which has better medical tracking than the U.S. — have concluded that the vaccines contributed to heart inflammation, especially in young men and boys. Officials in Hong Kong — another place with good health care data — have concluded that the vaccines caused severe shingles in about seven vaccine recipients per million.
Honesty and trust
These side effects are worthy of attention for two main reasons.
First, people who are suffering deserve recognition — and the lack of it can be infuriating. Dr. Janet Woodcock, a former F.D.A. commissioner, told The Times that she regretted not doing more to respond to people who blame the vaccines for harming them while she was in office. “I believe their suffering should be acknowledged, that they have real problems, and they should be taken seriously,” Woodcock said.
The second reason is that public health depends on public trust, and public trust in turn depends on honesty. During the pandemic, as I’ve written in the past, government officials and academic experts sometimes made the mistake of deciding that Americans couldn’t handle the truth.
Instead, experts emphasized evidence that was convenient to their recommendations and buried inconvenient facts. They exaggerated the risk of outdoor Covid transmission , the virus’s danger to children and the benefits of mask mandates , among other things. The goal may have been admirable — fighting a deadly virus — but the strategy backfired. Many people ended up confused, wondering what the truth was.
The overall picture
Here’s my best attempt to summarize the full truth about the Covid vaccines:
They are overwhelmingly safe and effective. They have saved millions of lives and prevented untold misery around the world. They’re so valuable that elderly people and those with underlying health conditions should be vigilant about getting booster shots when they’re eligible. For most children, on the other hand, booster shots seem to have only modest benefits, which is why many countries don’t recommend them .
And, yes, a small fraction of people will experience significant side effects from the vaccines. Eventually, scientific research may be able to better understand and reduce those side effects — which is more reason to pay attention to them.
Overall, Covid vaccines are probably the most beneficial medical breakthrough in years, if not decades.
I encourage you to read Apoorva’s article .
THE LATEST NEWS
Trump on trial.
The jury in Donald Trump’s criminal trial heard audio — secretly recorded by Trump’s former lawyer Michael Cohen — that seemed to show Trump’s involvement in the hush-money payments to two women who allegedly had affairs with him.
In one recording, Cohen claimed that Trump hates “the fact that we did it,” referring to paying off Stormy Daniels. In another, Trump and Cohen discussed the deal with Karen McDougal.
The jury also saw texts from 2016 in which Daniels’s former lawyer acknowledged that the hush money might have helped Trump win the election. “What have we done?” he wrote.
Prosecutors asked the judge to hold Trump in contempt for again violating a gag order .
Jimmy Kimmel joked about texts that mention his show being entered into evidence. “Why was I not asked to testify?” he said.
More on Politics
In North Carolina, a swing state, President Biden announced more funding to replace toxic lead pipes . He also met with the families of police officers killed this week in Charlotte.
Biden, defending America’s history of immigration, called Japan and India — U.S. allies — xenophobic and said that China and Russia “don’t want immigrants.”
Senator Bob Menendez’s lawyers want a psychologist to testify at his corruption trial that traumatic experiences explain the cash he stockpiled .
Campus Protests
In a televised statement, Biden condemned violence and intimidation on college campuses. “There’s the right to protest, but not the right to cause chaos,” he said.
In recent weeks, more than 2,000 demonstrators have been arrested or detained on campuses across the U.S., according to a Times tally.
The House passed a bill that would crack down on antisemitic speech at colleges . About one-third of Democrats voted no, and some far-right Republicans criticized it as a threat to Christian teachings.
A teakettle, sleeping bags and guard shifts: This is what it was like inside a building at Columbia occupied by pro-Palestinian demonstrators .
Universities including Brown agreed to consider ending investments linked to Israel in response to protests. It’s a gamble that risks angering influential donors .
Israel-Hamas War
Hamas’s political leader said the group was studying Israel’s latest cease-fire proposal with a “positive spirit” and would soon resume in-person negotiations.
Some senior Israeli officials are weighing a postwar plan for Gaza in which Israel would share oversight of the enclave with an alliance of Arab nations.
The war strategies of Benjamin Netanyahu and Hamas’s leader, Yahya Sinwar, leave little room for compromise , The Wall Street Journal reports.
More International News
In Taiwan, Times reporters joined the faithful on pilgrimages honoring Mazu , sometimes known as the Goddess of the Sea.
The U.S. accused Russia of using chemical weapons against Ukrainian troops, in violation of a global ban .
At least 29 people died after several days of heavy rain in southern Brazil.
Business and Economy
Oil companies, betting that the world is not yet ready to move past fossil fuels, have expanded drilling into deeper waters . (See photos of life aboard a facility 80 miles out to sea .)
The restaurant chain Dave & Buster’s, which features arcade games like Skee-Ball, announced that it will soon allow customers to gamble on the games .
Sony Pictures and the private equity company Apollo Global Management formally expressed interest in acquiring Paramount for around $26 billion.
Other Big Stories
A judge declared a mistrial in a lawsuit from three Iraqi men who said they were tortured at Abu Ghraib prison two decades ago.
The Kentucky Derby will take place tomorrow. The breakdown of 12 horses after the event last year has led to existential questions about the sport .
New York City police infringed on First Amendment rights when they blocked journalists from witnessing their raid on Columbia University , Mara Gay writes.
Gerrymandering turned Michigan into a bastion of minority rule — until democracy activists fought back and won , Ari Berman writes.
Here are columns by David Brooks on how the protests help Trump , Michelle Cottle on Biden’s wise words about the protests and Michelle Goldberg on Kari Lake’s abortion stance .
MORNING READS
Medals: For decades, the Olympics included art competitions. The winning entries are largely forgotten .
‘Queer food’: Scholars gathered to discuss the role gender and sexuality play in the food space. (Snacks were plentiful.)
Night sky: The Eta Aquarids meteor shower, a result of debris from Halley’s Comet, will be at its peak this weekend. Here’s how to watch .
Lives Lived: Peggy Mellon Hitchcock was born into privilege but enthusiastically supported the 1960s counterculture. She offered Timothy Leary and Richard Alpert her brother’s mansion after they lost their jobs at Harvard for experimenting with psychedelic drugs. Hitchcock died at 90 .
N.B.A.: The New York Knicks defeated the Philadelphia 76ers in a thrilling game on the road. The Knicks will face the Indiana Pacers in the second round of the playoffs.
N.H.L.: The Toronto Maple Leafs fended off elimination and forced a Game 7 against the Boston Bruins in a tense 2-1 win .
Kentucky Derby: Larry Demeritte, the trainer of long-shot West Saratoga, will become the first Black trainer with a Derby entrant since 1989.
ARTS AND IDEAS
A new story by Ben Sisario, The Times’s music industry reporter, explores the surprisingly complicated answer to what seems to be a simple question: What is a song?
When it comes to copyright — and the multimillion-dollar lawsuits that come from it — a song is often defined by only the notes written on a piece of sheet music, and not by the much fuller recording. “It is completely divorced from actual music-making practice,” said Joseph P. Fishman, a professor at Vanderbilt Law School.
More on culture
Times Book Review editors gathered their picks for the best books published since 2000 .
Hip-hop’s popularity is growing in China . Artists there must strike a balance between creative expression and appeasing censors, The A.P. reports.
TikTok and Universal Music Group reached a new licensing deal , ending a three-month stalemate that blocked songs from pop’s biggest stars from the platform.
THE MORNING RECOMMENDS …
Roast simple miso salmon as part of a traditional Japanese breakfast spread.
Snuggle into bed with a comfy duvet .
Buy a gift for an occult enthusiast .
Take our news quiz .
Here is today’s Spelling Bee . Yesterday’s pangram was motorway .
And here are today’s Mini Crossword , Wordle , Sudoku , Connections and Strands .
Thanks for spending part of your morning with The Times. See you tomorrow. — David
P.S. For World Press Freedom Day, A.G. Sulzberger, The Times’s publisher, and Joseph Kahn, the executive editor, wrote a letter calling attention to missing and detained journalists across the globe .
Sign up here to get this newsletter in your inbox . Reach our team at [email protected] .
David Leonhardt runs The Morning , The Times’s flagship daily newsletter. Since joining The Times in 1999, he has been an economics columnist, opinion columnist, head of the Washington bureau and founding editor of the Upshot section, among other roles. More about David Leonhardt
IMAGES
VIDEO
COMMENTS
June 27, 2023. Statins, one of the most extensively studied drugs on the planet, taken by tens of millions of Americans alone, have long had a perplexing side effect. Many patients—some 5 ...
Two widely used statins, rosuvastatin and atorvastatin, are equally effective at preventing heart attacks, strokes and death in people with coronary artery disease. But while rosuvastatin ...
Studies find drug protects against heart disease in high-risk groups. Two new studies found that statins, the most prescribed class of drugs to treat high cholesterol, are protective for high-risk groups who haven't yet had a heart attack or stroke but could be at risk of one, according to Harvard-affiliated Brigham and Women's Hospital.
The findings provide new insight into statins' curiously wide-ranging benefits, for conditions ranging from arteriosclerosis to diabetes, that have long been observed in the clinic. ... To take a closer look at statins' effect on blood vessels, Liu and colleagues tested a common statin, simvastatin, on lab-grown human endothelial cells ...
A meta-analysis of six statin trials that included 57,593 participants revealed a 13% increase in the relative risk of new-onset diabetes 3 — a more modest effect than that seen in the JUPITER ...
Statin therapies are not the cause of muscle pain in over 90% of those who experience symptoms, according to a new study led by researchers from Oxford Population Health. The results were published today in The Lancet and presented at the European Society of Cardiology Congress.
Very rarely, statins can cause life-threatening muscle damage called rhabdomyolysis (rab-doe-my-OL-ih-sis). Rhabdomyolysis can cause extreme muscle pain, liver damage, kidney failure and death. The risk of very serious side effects is extremely low. Only a few cases of rhabdomyolysis occur per million people taking statins.
They say their findings suggest that the benefit-to-harm balance of statins for adults without heart disease is generally favourable. Statins are widely used to prevent heart disease, and severe side effects are rare, but many people are reluctant to take them because of the potential for milder effects such as muscle weakness and stiffness.
Statins are associated with a small increased risk of side effects in patients without a history of heart disease, but these effects are mild compared with the potential benefits of treatment in ...
A new study shows statins are much more effective. ... based on prior research, ... "So the punch line of the trial is people blame statins for side effects the statins aren't really causing," he ...
Statins (HMG-CoA reductase inhibitors) are the most widely used and effective lipid-lowering drugs in clinical practice. With intensive clinical and basic research on statins, it has been found in recent years that statins have anti-hypertensive effects in addition to lipid-lowering effects. 3,4 Studies have found that statins also significantly lower blood pressure in hypertensive patients ...
Statins are often discontinued because of side effects, 1,2 even though some blinded trials have not shown an excess of symptoms with statins as compared with placebo. 3,4 Patients who had ...
Introduction. Statins [3-hydroxy-3-methylglutaryl coenzyme A reductase (HMG-CoA) inhibitors] are recommended as the treatment of first choice for management of hypercholesterolaemia and combined hyperlipidaemia by European guidelines for cardiovascular disease (CVD) prevention and lipid management. 1, 2 The efficacy of these agents in decreasing low-density lipoprotein cholesterol (LDL-C), a ...
As described in the evidence table above, Guthrie 2023 reported two-way results where age was varied between 40 and 80 years and 10-year risk was varied between 2% and 40%. 68 This found that high intensity statins were cost effective for every age/risk combination except: Men aged 74 to 80 years with 2% risk.
"Statins can be very helpful for long-term risk reduction and with very minimal side effects and great benefits. It's one of those key medications that have changed the face of medicine ...
For the meta-analysis, Sheppard and colleagues included 62 statin trials comprised of more than 120,000 patients without a history of cardiovascular disease who were followed for a mean of 3.9 years. Statins were associated with greater risks of the following side effects: Self-reported muscle symptoms (21 trials): OR 1.06; 95% CI 1.01-1.13
According to the study, statins would reduce the relative risk of dying by 9%. In absolute terms, the man would reduce his risk from 38% to 34.6%, and the woman from 1.4% to 1.3%. Patients and ...
However, any adverse impact of these side-effects on major vascular events has already been taken into account in the estimates of the absolute benefits. Statin therapy may cause symptomatic adverse events (eg, muscle pain or weakness) in up to about 50-100 patients (ie, 0·5-1·0% absolute harm) per 10 000 treated for 5 years.
Bempedoic acid, an ATP citrate lyase inhibitor, reduces low-density lipoprotein (LDL) cholesterol levels and is associated with a low incidence of muscle-related adverse events; its effects on card...
Introduction. HMG-CoA reductase inhibitors (statins) have been the best selling prescription drug class in the US and include atorvastatin, the best-selling prescription drug in the world - indeed in history. 1-3 These drugs are perceived to have a favorable safety profile 4-6 and have well documented benefits to cardiovascular disease in many groups, including persons who are younger and ...
Even when they work, the side effects of statins—particularly muscle pain—can be enough to make people stop taking the drugs. A new study has shown that another drug called Nexletol (bempedoic acid) can help people lower their cholesterol and prevent heart disease without causing the muscle pain that can come with taking statins.
Statins are an important tool to prevent major cardiovascular problems, but many patients stop taking them because of side effects, including muscle pain. However, for more than 90% of patients on ...
Cancer is an international interdisciplinary journal publishing articles on the latest clinical cancer research findings, spanning the breadth of oncology disciplines. Abstract Background Preclinical evidence suggests improved breast cancer survival associated with statin use, but findings from observational studies are conflicting and remain ...
By Linda Carroll. An alternative to statins may help reduce deaths from heart disease among people with high levels of LDL, or "bad" cholesterol, new research finds. When taken as a daily pill ...
The E.M.A. also counts tinnitus as a side effect of the Johnson & Johnson vaccine, although the American health agencies do not. There are more than 17,000 reports of tinnitus following Covid ...
Results. Myalgia is the most common side effect of statin use, with documented rates from 1-10%. Rhabdomyolysis is the most serious adverse effect from statin use, though it occurs quite rarely (less than 0.1%). The most common risk factors for statin-related myopathy include hypothyroidism, polypharmacy and alcohol abuse.
More than 270 million Americans received about 677 million doses of the Covid vaccines, and even rare side effects — occurring, say, in just 0.001 percent of patients — might mean thousands of ...
The 'nocebo' effect describes the opposite, where negative expectations about treatment can cause harmful side effects. New research, published recently in Communications Psychology, found that the nocebo effect has the capacity to spread beyond the original "harmful" experience, and that this is heightened in cases when the ...
Shaun Barcavage, 54, a nurse practitioner in New York City, has experienced a ringing sound in his ears, a racing heart and pain in his eyes, mouth and genitals for more than three years.