
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- HHS Author Manuscripts

Observational Studies: Cohort and Case-Control Studies
Jae w. song.
1 Research Fellow, Section of Plastic Surgery, Department of Surgery The University of Michigan Health System; Ann Arbor, MI
Kevin C. Chung
2 Professor of Surgery, Section of Plastic Surgery, Department of Surgery The University of Michigan Health System; Ann Arbor, MI
Observational studies are an important category of study designs. To address some investigative questions in plastic surgery, randomized controlled trials are not always indicated or ethical to conduct. Instead, observational studies may be the next best method to address these types of questions. Well-designed observational studies have been shown to provide results similar to randomized controlled trials, challenging the belief that observational studies are second-rate. Cohort studies and case-control studies are two primary types of observational studies that aid in evaluating associations between diseases and exposures. In this review article, we describe these study designs, methodological issues, and provide examples from the plastic surgery literature.
Because of the innovative nature of the specialty, plastic surgeons are frequently confronted with a spectrum of clinical questions by patients who inquire about “best practices.” It is thus essential that plastic surgeons know how to critically appraise the literature to understand and practice evidence-based medicine (EBM) and also contribute to the effort by carrying out high-quality investigations. 1 Well-designed randomized controlled trials (RCTs) have held the pre-eminent position in the hierarchy of EBM as level I evidence ( Table 1 ). However, RCT methodology, which was first developed for drug trials, can be difficult to conduct for surgical investigations. 3 Instead, well-designed observational studies, recognized as level II or III evidence, can play an important role in deriving evidence for plastic surgery. Results from observational studies are often criticized for being vulnerable to influences by unpredictable confounding factors. However, recent work has challenged this notion, showing comparable results between observational studies and RCTs. 4 , 5 Observational studies can also complement RCTs in hypothesis generation, establishing questions for future RCTs, and defining clinical conditions.
Levels of Evidence Based Medicine
From REF 1 .
Observational studies fall under the category of analytic study designs and are further sub-classified as observational or experimental study designs ( Figure 1 ). The goal of analytic studies is to identify and evaluate causes or risk factors of diseases or health-related events. The differentiating characteristic between observational and experimental study designs is that in the latter, the presence or absence of undergoing an intervention defines the groups. By contrast, in an observational study, the investigator does not intervene and rather simply “observes” and assesses the strength of the relationship between an exposure and disease variable. 6 Three types of observational studies include cohort studies, case-control studies, and cross-sectional studies ( Figure 1 ). Case-control and cohort studies offer specific advantages by measuring disease occurrence and its association with an exposure by offering a temporal dimension (i.e. prospective or retrospective study design). Cross-sectional studies, also known as prevalence studies, examine the data on disease and exposure at one particular time point ( Figure 2 ). 6 Because the temporal relationship between disease occurrence and exposure cannot be established, cross-sectional studies cannot assess the cause and effect relationship. In this review, we will primarily discuss cohort and case-control study designs and related methodologic issues.

Analytic Study Designs. Adapted with permission from Joseph Eisenberg, Ph.D.

Temporal Design of Observational Studies: Cross-sectional studies are known as prevalence studies and do not have an inherent temporal dimension. These studies evaluate subjects at one point in time, the present time. By contrast, cohort studies can be either retrospective (latin derived prefix, “retro” meaning “back, behind”) or prospective (greek derived prefix, “pro” meaning “before, in front of”). Retrospective studies “look back” in time contrasting with prospective studies, which “look ahead” to examine causal associations. Case-control study designs are also retrospective and assess the history of the subject for the presence or absence of an exposure.
COHORT STUDY
The term “cohort” is derived from the Latin word cohors . Roman legions were composed of ten cohorts. During battle each cohort, or military unit, consisting of a specific number of warriors and commanding centurions, were traceable. The word “cohort” has been adopted into epidemiology to define a set of people followed over a period of time. W.H. Frost, an epidemiologist from the early 1900s, was the first to use the word “cohort” in his 1935 publication assessing age-specific mortality rates and tuberculosis. 7 The modern epidemiological definition of the word now means a “group of people with defined characteristics who are followed up to determine incidence of, or mortality from, some specific disease, all causes of death, or some other outcome.” 7
Study Design
A well-designed cohort study can provide powerful results. In a cohort study, an outcome or disease-free study population is first identified by the exposure or event of interest and followed in time until the disease or outcome of interest occurs ( Figure 3A ). Because exposure is identified before the outcome, cohort studies have a temporal framework to assess causality and thus have the potential to provide the strongest scientific evidence. 8 Advantages and disadvantages of a cohort study are listed in Table 2 . 2 , 9 Cohort studies are particularly advantageous for examining rare exposures because subjects are selected by their exposure status. Additionally, the investigator can examine multiple outcomes simultaneously. Disadvantages include the need for a large sample size and the potentially long follow-up duration of the study design resulting in a costly endeavor.

Cohort and Case-Control Study Designs
Advantages and Disadvantages of the Cohort Study
Cohort studies can be prospective or retrospective ( Figure 2 ). Prospective studies are carried out from the present time into the future. Because prospective studies are designed with specific data collection methods, it has the advantage of being tailored to collect specific exposure data and may be more complete. The disadvantage of a prospective cohort study may be the long follow-up period while waiting for events or diseases to occur. Thus, this study design is inefficient for investigating diseases with long latency periods and is vulnerable to a high loss to follow-up rate. Although prospective cohort studies are invaluable as exemplified by the landmark Framingham Heart Study, started in 1948 and still ongoing, 10 in the plastic surgery literature this study design is generally seen to be inefficient and impractical. Instead, retrospective cohort studies are better indicated given the timeliness and inexpensive nature of the study design.
Retrospective cohort studies, also known as historical cohort studies, are carried out at the present time and look to the past to examine medical events or outcomes. In other words, a cohort of subjects selected based on exposure status is chosen at the present time, and outcome data (i.e. disease status, event status), which was measured in the past, are reconstructed for analysis. The primary disadvantage of this study design is the limited control the investigator has over data collection. The existing data may be incomplete, inaccurate, or inconsistently measured between subjects. 2 However, because of the immediate availability of the data, this study design is comparatively less costly and shorter than prospective cohort studies. For example, Spear and colleagues examined the effect of obesity and complication rates after undergoing the pedicled TRAM flap reconstruction by retrospectively reviewing 224 pedicled TRAM flaps in 200 patients over a 10-year period. 11 In this example, subjects who underwent the pedicled TRAM flap reconstruction were selected and categorized into cohorts by their exposure status: normal/underweight, overweight, or obese. The outcomes of interest were various flap and donor site complications. The findings revealed that obese patients had a significantly higher incidence of donor site complications, multiple flap complications, and partial flap necrosis than normal or overweight patients. An advantage of the retrospective study design analysis is the immediate access to the data. A disadvantage is the limited control over the data collection because data was gathered retrospectively over 10-years; for example, a limitation reported by the authors is that mastectomy flap necrosis was not uniformly recorded for all subjects. 11
An important distinction lies between cohort studies and case-series. The distinguishing feature between these two types of studies is the presence of a control, or unexposed, group. Contrasting with epidemiological cohort studies, case-series are descriptive studies following one small group of subjects. In essence, they are extensions of case reports. Usually the cases are obtained from the authors' experiences, generally involve a small number of patients, and more importantly, lack a control group. 12 There is often confusion in designating studies as “cohort studies” when only one group of subjects is examined. Yet, unless a second comparative group serving as a control is present, these studies are defined as case-series. The next step in strengthening an observation from a case-series is selecting appropriate control groups to conduct a cohort or case-control study, the latter which is discussed in the following section about case-control studies. 9
Methodological Issues
Selection of subjects in cohort studies.
The hallmark of a cohort study is defining the selected group of subjects by exposure status at the start of the investigation. A critical characteristic of subject selection is to have both the exposed and unexposed groups be selected from the same source population ( Figure 4 ). 9 Subjects who are not at risk for developing the outcome should be excluded from the study. The source population is determined by practical considerations, such as sampling. Subjects may be effectively sampled from the hospital, be members of a community, or from a doctor's individual practice. A subset of these subjects will be eligible for the study.

Levels of Subject Selection. Adapted from Ref 9 .
Attrition Bias (Loss to follow-up)
Because prospective cohort studies may require long follow-up periods, it is important to minimize loss to follow-up. Loss to follow-up is a situation in which the investigator loses contact with the subject, resulting in missing data. If too many subjects are loss to follow-up, the internal validity of the study is reduced. A general rule of thumb requires that the loss to follow-up rate not exceed 20% of the sample. 6 Any systematic differences related to the outcome or exposure of risk factors between those who drop out and those who stay in the study must be examined, if possible, by comparing individuals who remain in the study and those who were loss to follow-up or dropped out. It is therefore important to select subjects who can be followed for the entire duration of the cohort study. Methods to minimize loss to follow-up are listed in Table 3 .
Methods to Minimize Loss to Follow-Up
Adapted from REF 2 .
CASE-CONTROL STUDIES
Case-control studies were historically borne out of interest in disease etiology. The conceptual basis of the case-control study is similar to taking a history and physical; the diseased patient is questioned and examined, and elements from this history taking are knitted together to reveal characteristics or factors that predisposed the patient to the disease. In fact, the practice of interviewing patients about behaviors and conditions preceding illness dates back to the Hippocratic writings of the 4 th century B.C. 7
Reasons of practicality and feasibility inherent in the study design typically dictate whether a cohort study or case-control study is appropriate. This study design was first recognized in Janet Lane-Claypon's study of breast cancer in 1926, revealing the finding that low fertility rate raises the risk of breast cancer. 13 , 14 In the ensuing decades, case-control study methodology crystallized with the landmark publication linking smoking and lung cancer in the 1950s. 15 Since that time, retrospective case-control studies have become more prominent in the biomedical literature with more rigorous methodological advances in design, execution, and analysis.
Case-control studies identify subjects by outcome status at the outset of the investigation. Outcomes of interest may be whether the subject has undergone a specific type of surgery, experienced a complication, or is diagnosed with a disease ( Figure 3B ). Once outcome status is identified and subjects are categorized as cases, controls (subjects without the outcome but from the same source population) are selected. Data about exposure to a risk factor or several risk factors are then collected retrospectively, typically by interview, abstraction from records, or survey. Case-control studies are well suited to investigate rare outcomes or outcomes with a long latency period because subjects are selected from the outset by their outcome status. Thus in comparison to cohort studies, case-control studies are quick, relatively inexpensive to implement, require comparatively fewer subjects, and allow for multiple exposures or risk factors to be assessed for one outcome ( Table 4 ). 2 , 9
Advantages and Disadvantages of the Case-Control Study
An example of a case-control investigation is by Zhang and colleagues who examined the association of environmental and genetic factors associated with rare congenital microtia, 16 which has an estimated prevalence of 0.83 to 17.4 in 10,000. 17 They selected 121 congenital microtia cases based on clinical phenotype, and 152 unaffected controls, matched by age and sex in the same hospital and same period. Controls were of Hans Chinese origin from Jiangsu, China, the same area from where the cases were selected. This allowed both the controls and cases to have the same genetic background, important to note given the investigated association between genetic factors and congenital microtia. To examine environmental factors, a questionnaire was administered to the mothers of both cases and controls. The authors concluded that adverse maternal health was among the main risk factors for congenital microtia, specifically maternal disease during pregnancy (OR 5.89, 95% CI 2.36-14.72), maternal toxicity exposure during pregnancy (OR 4.76, 95% CI 1.66-13.68), and resident area, such as living near industries associated with air pollution (OR 7.00, 95% CI 2.09-23.47). 16 A case-control study design is most efficient for this investigation, given the rarity of the disease outcome. Because congenital microtia is thought to have multifactorial causes, an additional advantage of the case-control study design in this example is the ability to examine multiple exposures and risk factors.
Selection of Cases
Sampling in a case-control study design begins with selecting the cases. In a case-control study, it is imperative that the investigator has explicitly defined inclusion and exclusion criteria prior to the selection of cases. For example, if the outcome is having a disease, specific diagnostic criteria, disease subtype, stage of disease, or degree of severity should be defined. Such criteria ensure that all the cases are homogenous. Second, cases may be selected from a variety of sources, including hospital patients, clinic patients, or community subjects. Many communities maintain registries of patients with certain diseases and can serve as a valuable source of cases. However, despite the methodologic convenience of this method, validity issues may arise. For example, if cases are selected from one hospital, identified risk factors may be unique to that single hospital. This methodological choice may weaken the generalizability of the study findings. Another example is choosing cases from the hospital versus the community; most likely cases from the hospital sample will represent a more severe form of the disease than those in the community. 2 Finally, it is also important to select cases that are representative of cases in the target population to strengthen the study's external validity ( Figure 4 ). Potential reasons why cases from the original target population eventually filter through and are available as cases (study participants) for a case-control study are illustrated in Figure 5 .

Levels of Case Selection. Adapted from Ref 2 .
Selection of Controls
Selecting the appropriate group of controls can be one of the most demanding aspects of a case-control study. An important principle is that the distribution of exposure should be the same among cases and controls; in other words, both cases and controls should stem from the same source population. The investigator may also consider the control group to be an at-risk population, with the potential to develop the outcome. Because the validity of the study depends upon the comparability of these two groups, cases and controls should otherwise meet the same inclusion criteria in the study.
A case-control study design that exemplifies this methodological feature is by Chung and colleagues, who examined maternal cigarette smoking during pregnancy and the risk of newborns developing cleft lip/palate. 18 A salient feature of this study is the use of the 1996 U.S. Natality database, a population database, from which both cases and controls were selected. This database provides a large sample size to assess newborn development of cleft lip/palate (outcome), which has a reported incidence of 1 in 1000 live births, 19 and also enabled the investigators to choose controls (i.e., healthy newborns) that were generalizable to the general population to strengthen the study's external validity. A significant relationship with maternal cigarette smoking and cleft lip/palate in the newborn was reported in this study (adjusted OR 1.34, 95% CI 1.36-1.76). 18
Matching is a method used in an attempt to ensure comparability between cases and controls and reduces variability and systematic differences due to background variables that are not of interest to the investigator. 8 Each case is typically individually paired with a control subject with respect to the background variables. The exposure to the risk factor of interest is then compared between the cases and the controls. This matching strategy is called individual matching. Age, sex, and race are often used to match cases and controls because they are typically strong confounders of disease. 20 Confounders are variables associated with the risk factor and may potentially be a cause of the outcome. 8 Table 5 lists several advantages and disadvantages with a matching design.
Advantages and Disadvantages for Using a Matching Strategy
Multiple Controls
Investigations examining rare outcomes may have a limited number of cases to select from, whereas the source population from which controls can be selected is much larger. In such scenarios, the study may be able to provide more information if multiple controls per case are selected. This method increases the “statistical power” of the investigation by increasing the sample size. The precision of the findings may improve by having up to about three or four controls per case. 21 - 23
Bias in Case-Control Studies
Evaluating exposure status can be the Achilles heel of case-control studies. Because information about exposure is typically collected by self-report, interview, or from recorded information, it is susceptible to recall bias, interviewer bias, or will rely on the completeness or accuracy of recorded information, respectively. These biases decrease the internal validity of the investigation and should be carefully addressed and reduced in the study design. Recall bias occurs when a differential response between cases and controls occurs. The common scenario is when a subject with disease (case) will unconsciously recall and report an exposure with better clarity due to the disease experience. Interviewer bias occurs when the interviewer asks leading questions or has an inconsistent interview approach between cases and controls. A good study design will implement a standardized interview in a non-judgemental atmosphere with well-trained interviewers to reduce interviewer bias. 9
The STROBE Statement: The Strengthening the Reporting of Observational Studies in Epidemiology Statement
In 2004, the first meeting of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) group took place in Bristol, UK. 24 The aim of the group was to establish guidelines on reporting observational research to improve the transparency of the methods, thereby facilitating the critical appraisal of a study's findings. A well-designed but poorly reported study is disadvantaged in contributing to the literature because the results and generalizability of the findings may be difficult to assess. Thus a 22-item checklist was generated to enhance the reporting of observational studies across disciplines. 25 , 26 This checklist is also located at the following website: www.strobe-statement.org . This statement is applicable to cohort studies, case-control studies, and cross-sectional studies. In fact, 18 of the checklist items are common to all three types of observational studies, and 4 items are specific to each of the 3 specific study designs. In an effort to provide specific guidance to go along with this checklist, an “explanation and elaboration” article was published for users to better appreciate each item on the checklist. 27 Plastic surgery investigators should peruse this checklist prior to designing their study and when they are writing up the report for publication. In fact, some journals now require authors to follow the STROBE Statement. A list of participating journals can be found on this website: http://www.strobe-statement.org./index.php?id=strobe-endorsement .
Due to the limitations in carrying out RCTs in surgical investigations, observational studies are becoming more popular to investigate the relationship between exposures, such as risk factors or surgical interventions, and outcomes, such as disease states or complications. Recognizing that well-designed observational studies can provide valid results is important among the plastic surgery community, so that investigators can both critically appraise and appropriately design observational studies to address important clinical research questions. The investigator planning an observational study can certainly use the STROBE statement as a tool to outline key features of a study as well as coming back to it again at the end to enhance transparency in methodology reporting.
Acknowledgments
Supported in part by a Midcareer Investigator Award in Patient-Oriented Research (K24 AR053120) from the National Institute of Arthritis and Musculoskeletal and Skin Diseases (to Dr. Kevin C. Chung).
None of the authors has a financial interest in any of the products, devices, or drugs mentioned in this manuscript.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
- En español – ExME
- Em português – EME
Case-control and Cohort studies: A brief overview
Posted on 6th December 2017 by Saul Crandon

Introduction
Case-control and cohort studies are observational studies that lie near the middle of the hierarchy of evidence . These types of studies, along with randomised controlled trials, constitute analytical studies, whereas case reports and case series define descriptive studies (1). Although these studies are not ranked as highly as randomised controlled trials, they can provide strong evidence if designed appropriately.
Case-control studies
Case-control studies are retrospective. They clearly define two groups at the start: one with the outcome/disease and one without the outcome/disease. They look back to assess whether there is a statistically significant difference in the rates of exposure to a defined risk factor between the groups. See Figure 1 for a pictorial representation of a case-control study design. This can suggest associations between the risk factor and development of the disease in question, although no definitive causality can be drawn. The main outcome measure in case-control studies is odds ratio (OR) .
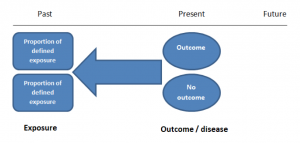
Figure 1. Case-control study design.
Cases should be selected based on objective inclusion and exclusion criteria from a reliable source such as a disease registry. An inherent issue with selecting cases is that a certain proportion of those with the disease would not have a formal diagnosis, may not present for medical care, may be misdiagnosed or may have died before getting a diagnosis. Regardless of how the cases are selected, they should be representative of the broader disease population that you are investigating to ensure generalisability.
Case-control studies should include two groups that are identical EXCEPT for their outcome / disease status.
As such, controls should also be selected carefully. It is possible to match controls to the cases selected on the basis of various factors (e.g. age, sex) to ensure these do not confound the study results. It may even increase statistical power and study precision by choosing up to three or four controls per case (2).
Case-controls can provide fast results and they are cheaper to perform than most other studies. The fact that the analysis is retrospective, allows rare diseases or diseases with long latency periods to be investigated. Furthermore, you can assess multiple exposures to get a better understanding of possible risk factors for the defined outcome / disease.
Nevertheless, as case-controls are retrospective, they are more prone to bias. One of the main examples is recall bias. Often case-control studies require the participants to self-report their exposure to a certain factor. Recall bias is the systematic difference in how the two groups may recall past events e.g. in a study investigating stillbirth, a mother who experienced this may recall the possible contributing factors a lot more vividly than a mother who had a healthy birth.
A summary of the pros and cons of case-control studies are provided in Table 1.
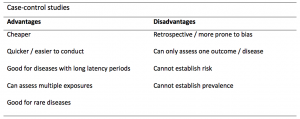
Table 1. Advantages and disadvantages of case-control studies.
Cohort studies
Cohort studies can be retrospective or prospective. Retrospective cohort studies are NOT the same as case-control studies.
In retrospective cohort studies, the exposure and outcomes have already happened. They are usually conducted on data that already exists (from prospective studies) and the exposures are defined before looking at the existing outcome data to see whether exposure to a risk factor is associated with a statistically significant difference in the outcome development rate.
Prospective cohort studies are more common. People are recruited into cohort studies regardless of their exposure or outcome status. This is one of their important strengths. People are often recruited because of their geographical area or occupation, for example, and researchers can then measure and analyse a range of exposures and outcomes.
The study then follows these participants for a defined period to assess the proportion that develop the outcome/disease of interest. See Figure 2 for a pictorial representation of a cohort study design. Therefore, cohort studies are good for assessing prognosis, risk factors and harm. The outcome measure in cohort studies is usually a risk ratio / relative risk (RR).
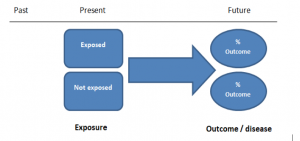
Figure 2. Cohort study design.
Cohort studies should include two groups that are identical EXCEPT for their exposure status.
As a result, both exposed and unexposed groups should be recruited from the same source population. Another important consideration is attrition. If a significant number of participants are not followed up (lost, death, dropped out) then this may impact the validity of the study. Not only does it decrease the study’s power, but there may be attrition bias – a significant difference between the groups of those that did not complete the study.
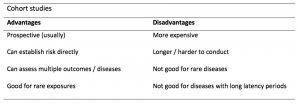
Cohort studies can assess a range of outcomes allowing an exposure to be rigorously assessed for its impact in developing disease. Additionally, they are good for rare exposures, e.g. contact with a chemical radiation blast.
Whilst cohort studies are useful, they can be expensive and time-consuming, especially if a long follow-up period is chosen or the disease itself is rare or has a long latency.
A summary of the pros and cons of cohort studies are provided in Table 2.
The Strengthening of Reporting of Observational Studies in Epidemiology Statement (STROBE)
STROBE provides a checklist of important steps for conducting these types of studies, as well as acting as best-practice reporting guidelines (3). Both case-control and cohort studies are observational, with varying advantages and disadvantages. However, the most important factor to the quality of evidence these studies provide, is their methodological quality.
- Song, J. and Chung, K. Observational Studies: Cohort and Case-Control Studies . Plastic and Reconstructive Surgery.  2010 Dec;126(6):2234-2242.
- Ury HK. Efficiency of case-control studies with multiple controls per case: Continuous or dichotomous data . Biometrics . 1975 Sep;31(3):643–649.
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies.  Lancet 2007 Oct;370(9596):1453-14577. PMID: 18064739.

Saul Crandon
Leave a reply cancel reply.
Your email address will not be published. Required fields are marked *
Save my name, email, and website in this browser for the next time I comment.
No Comments on Case-control and Cohort studies: A brief overview

Very well presented, excellent clarifications. Has put me right back into class, literally!

Very clear and informative! Thank you.

very informative article.

Thank you for the easy to understand blog in cohort studies. I want to follow a group of people with and without a disease to see what health outcomes occurs to them in future such as hospitalisations, diagnoses, procedures etc, as I have many health outcomes to consider, my questions is how to make sure these outcomes has not occurred before the “exposure disease”. As, in cohort studies we are looking at incidence (new) cases, so if an outcome have occurred before the exposure, I can leave them out of the analysis. But because I am not looking at a single outcome which can be checked easily and if happened before exposure can be left out. I have EHR data, so all the exposure and outcome have occurred. my aim is to check the rates of different health outcomes between the exposed)dementia) and unexposed(non-dementia) individuals.

Very helpful information

Thanks for making this subject student friendly and easier to understand. A great help.

Thanks a lot. It really helped me to understand the topic. I am taking epidemiology class this winter, and your paper really saved me.
Happy new year.

Wow its amazing n simple way of briefing ,which i was enjoyed to learn this.its very easy n quick to pick ideas .. Thanks n stay connected

Saul you absolute melt! Really good work man

am a student of public health. This information is simple and well presented to the point. Thank you so much.

very helpful information provided here

really thanks for wonderful information because i doing my bachelor degree research by survival model

Quite informative thank you so much for the info please continue posting. An mph student with Africa university Zimbabwe.

Thank you this was so helpful amazing

Apreciated the information provided above.

So clear and perfect. The language is simple and superb.I am recommending this to all budding epidemiology students. Thanks a lot.

Great to hear, thank you AJ!

I have recently completed an investigational study where evidence of phlebitis was determined in a control cohort by data mining from electronic medical records. We then introduced an intervention in an attempt to reduce incidence of phlebitis in a second cohort. Again, results were determined by data mining. This was an expedited study, so there subjects were enrolled in a specific cohort based on date(s) of the drug infused. How do I define this study? Thanks so much.

thanks for the information and knowledge about observational studies. am a masters student in public health/epidemilogy of the faculty of medicines and pharmaceutical sciences , University of Dschang. this information is very explicit and straight to the point

Very much helpful
Subscribe to our newsletter
You will receive our monthly newsletter and free access to Trip Premium.
Related Articles

Cluster Randomized Trials: Concepts
This blog summarizes the concepts of cluster randomization, and the logistical and statistical considerations while designing a cluster randomized controlled trial.

Expertise-based Randomized Controlled Trials
This blog summarizes the concepts of Expertise-based randomized controlled trials with a focus on the advantages and challenges associated with this type of study.

An introduction to different types of study design
Conducting successful research requires choosing the appropriate study design. This article describes the most common types of designs conducted by researchers.
Log in using your username and password
- Search More Search for this keyword Advanced search
- Latest content
- Current issue
- BMJ Journals More You are viewing from: Google Indexer
You are here
- Volume 20, Issue 1
- Observational research methods. Research design II: cohort, cross sectional, and case-control studies
- Article Text
- Article info
- Citation Tools
- Rapid Responses
- Article metrics
- Department of Accident and Emergency Medicine, Taunton and Somerset Hospital, Taunton, Somerset, UK
- Correspondence to: Dr C J Mann; tonygood{at}doctors.org.uk
Cohort, cross sectional, and case-control studies are collectively referred to as observational studies. Often these studies are the only practicable method of studying various problems, for example, studies of aetiology, instances where a randomised controlled trial might be unethical, or if the condition to be studied is rare. Cohort studies are used to study incidence, causes, and prognosis. Because they measure events in chronological order they can be used to distinguish between cause and effect. Cross sectional studies are used to determine prevalence. They are relatively quick and easy but do not permit distinction between cause and effect. Case controlled studies compare groups retrospectively. They seek to identify possible predictors of outcome and are useful for studying rare diseases or outcomes. They are often used to generate hypotheses that can then be studied via prospective cohort or other studies.
- research methods
- cohort study
- case-control study
- cross sectional study
https://doi.org/10.1136/emj.20.1.54
Statistics from Altmetric.com
Request permissions.
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
Cohort, cross sectional, and case-control studies are often referred to as observational studies because the investigator simply observes. No interventions are carried out by the investigator. With the recent emphasis on evidence based medicine and the formation of the Cochrane Database of randomised controlled trials, such studies have been somewhat glibly maligned. However, they remain important because many questions can be efficiently answered by these methods and sometimes they are the only methods available.
The objective of most clinical studies is to determine one of the following—prevalence, incidence, cause, prognosis, or effect of treatment; it is therefore useful to remember which type of study is most commonly associated with each objective (table 1)
- View inline
While an appropriate choice of study design is vital, it is not sufficient. The hallmark of good research is the rigor with which it is conducted. A checklist of the key points in any study irrespective of the basic design is given in box 1.
Study purpose
The aim of the study should be clearly stated.
The sample should accurately reflect the population from which it is drawn.
The source of the sample should be stated.
The sampling method should be described and the sample size should be justified.
Entry criteria and exclusions should be stated and justified.
The number of patients lost to follow up should be stated and explanations given.
Control group
The control group should be easily identifiable.
The source of the controls should be explained—are they from the same population as the sample?
Are the controls matched or randomised—to minimise bias and confounding.
Quality of measurements and outcomes
Validity—are the measurements used regarded as valid by other investigators?
Reproducibility—can the results be repeated or is there a reason to suspect they may be a “one off”?
Blinded—were the investigators or subjects aware of their subject/control allocation?
Quality control—has the methodology been rigorously adhered to?
Completeness
Compliance—did all patients comply with the study?
Drop outs—how many failed to complete the study?
Missing data—how much are unavailable and why?
Distorting influences
Extraneous treatments—other interventions that may have affected some but not all of the subjects.
Confounding factors—Are there other variables that might influence the results?
Appropriate analysis—Have appropriate statistical tests been used?
All studies should be internally valid. That is, the conclusions can be logically drawn from the results produced by an appropriate methodology. For a study to be regarded as valid it must be shown that it has indeed demonstrated what it says it has. A study that is not internally valid should not be published because the findings cannot be accepted.
The question of external validity relates to the value of the results of the study to other populations—that is, the generalisability of the results. For example, a study showing that 80% of the Swedish population has blond hair, might be used to make a sensible prediction of the incidence of blond hair in other Scandinavian countries, but would be invalid if applied to most other populations.
Every published study should contain sufficient information to allow the reader to analyse the data with reference to these key points.
In this article each of the three important observational research methods will be discussed with emphasis on their strengths and weaknesses. In so doing it should become apparent why a given study used a particular research method and which method might best answer a particular clinical problem.
COHORT STUDIES
These are the best method for determining the incidence and natural history of a condition. The studies may be prospective or retrospective and sometimes two cohorts are compared.
Prospective cohort studies
A group of people is chosen who do not have the outcome of interest (for example, myocardial infarction). The investigator then measures a variety of variables that might be relevant to the development of the condition. Over a period of time the people in the sample are observed to see whether they develop the outcome of interest (that is, myocardial infarction).
In single cohort studies those people who do not develop the outcome of interest are used as internal controls.
Where two cohorts are used, one group has been exposed to or treated with the agent of interest and the other has not, thereby acting as an external control.
Retrospective cohort studies
These use data already collected for other purposes. The methodology is the same but the study is performed posthoc. The cohort is “followed up” retrospectively. The study period may be many years but the time to complete the study is only as long as it takes to collate and analyse the data.
Advantages and disadvantages
The use of cohorts is often mandatory as a randomised controlled trial may be unethical; for example, you cannot deliberately expose people to cigarette smoke or asbestos. Thus research on risk factors relies heavily on cohort studies.
As cohort studies measure potential causes before the outcome has occurred the study can demonstrate that these “causes” preceded the outcome, thereby avoiding the debate as to which is cause and which is effect.
A further advantage is that a single study can examine various outcome variables. For example, cohort studies of smokers can simultaneously look at deaths from lung, cardiovascular, and cerebrovascular disease. This contrasts with case-control studies as they assess only one outcome variable (that is, whatever outcome the cases have entered the study with).
Cohorts permit calculation of the effect of each variable on the probability of developing the outcome of interest (relative risk). However, where a certain outcome is rare then a prospective cohort study is inefficient. For example, studying 100 A&E attenders with minor injuries for the outcome of diabetes mellitus will probably produce only one patient with the outcome of interest. The efficiency of a prospective cohort study increases as the incidence of any particular outcome increases. Thus a study of patients with a diagnosis of deliberate self harm in the 12 months after initial presentation would be efficiently studied using a cohort design.
Another problem with prospective cohort studies is the loss of some subjects to follow up. This can significantly affect the outcome. Taking incidence analysis as an example (incidence = cases/per period of time), it can be seen that the loss of a few cases will seriously affect the numerator and hence the calculated incidence. The rarer the condition the more significant this effect.
Retrospective studies are much cheaper as the data have already been collected. One advantage of such a study design is the lack of bias because the outcome of current interest was not the original reason for the data to be collected. However, because the cohort was originally constructed for another purpose it is unlikely that all the relevant information will have been rigorously collected.
Retrospective cohorts also suffer the disadvantage that people with the outcome of interest are more likely to remember certain antecedents, or exaggerate or minimise what they now consider to be risk factors (recall bias).
Where two cohorts are compared one will have been exposed to the agent of interest and one will not. The major disadvantage is the inability to control for all other factors that might differ between the two groups. These factors are known as confounding variables.
A confounding variable is independently associated with both the variable of interest and the outcome of interest. For example, lung cancer (outcome) is less common in people with asthma (variable). However, it is unlikely that asthma in itself confers any protection against lung cancer. It is more probable that the incidence of lung cancer is lower in people with asthma because fewer asthmatics smoke cigarettes (confounding variable). There are a virtually infinite number of potential confounding variables that, however unlikely, could just explain the result. In the past this has been used to suggest that there is a genetic influence that makes people want to smoke and also predisposes them to cancer.
The only way to eliminate all possibility of a confounding variable is via a prospective randomised controlled study. In this type of study each type of exposure is assigned by chance and so confounding variables should be present in equal numbers in both groups.
Finally, problems can arise as a result of bias. Bias can occur in any research and reflects the potential that the sample studied is not representative of the population it was drawn from and/or the population at large. A classic example is using employed people, as employment is itself associated with generally better health than unemployed people. Similarly people who respond to questionnaires tend to be fitter and more motivated than those who do not. People attending A&E departments should not be presumed to be representative of the population at large.
How to run a cohort study
If the data are readily available then a retrospective design is the quickest method. If high quality, reliable data are not available a prospective study will be required.
The first step is the definition of the sample group. Each subject must have the potential to develop the outcome of interest (that is, circumcised men should not be included in a cohort designed to study paraphimosis). Furthermore, the sample population must be representative of the general population if the study is primarily looking at the incidence and natural history of the condition (descriptive).
If however the aim is to analyse the relation between predictor variables and outcomes (analytical) then the sample should contain as many patients likely to develop the outcome as possible, otherwise much time and expense will be spent collecting information of little value.
Cohort studies
Cohort studies describe incidence or natural history.
They analyse predictors (risk factors) thereby enabling calculation of relative risk.
Cohort studies measure events in temporal sequence thereby distinguishing causes from effects.
Retrospective cohorts where available are cheaper and quicker.
Confounding variables are the major problem in analysing cohort studies.
Subject selection and loss to follow up is a major potential cause of bias.
Each variable studied must be accurately measured. Variables that are relatively fixed, for example, height need only be recorded once. Where change is more probable, for example, drug misuse or weight, repeated measurements will be required.
To minimise the potential for missing a confounding variable all probable relevant variables should be measured. If this is not done the study conclusions can be readily criticised. All patients entered into the study should also be followed up for the duration of the study. Losses can significantly affect the validity of the results. To minimise this as much information about the patient (name, address, telephone, GP, etc) needs to be recorded as soon as the patient is entered into the study. Regular contact should be made; it is hardly surprising if the subjects have moved or lost interest and become lost to follow up if they are only contacted at 10 year intervals!
Beware, follow up is usually easier in people who have been exposed to the agent of interest and this may lead to bias.
There are many famous examples of Cohort studies including the Framingham heart study, 2 the UK study of doctors who smoke 3 and Professor Neville Butler‘s studies on British children born in 1958. 4 A recent example of a prospective cohort study by Davey Smith et al was published in the BMJ 5 and a retrospective cohort design was used to assess the use of A&E departments by people with diabetes. 6
CROSS SECTIONAL STUDIES
These are primarily used to determine prevalence. Prevalence equals the number of cases in a population at a given point in time. All the measurements on each person are made at one point in time. Prevalence is vitally important to the clinician because it influences considerably the likelihood of any particular diagnosis and the predictive value of any investigation. For example, knowing that ascending cholangitis in children is very rare enables the clinician to look for other causes of abdominal pain in this patient population.
Cross sectional studies are also used to infer causation.
At one point in time the subjects are assessed to determine whether they were exposed to the relevant agent and whether they have the outcome of interest. Some of the subjects will not have been exposed nor have the outcome of interest. This clearly distinguishes this type of study from the other observational studies (cohort and case controlled) where reference to either exposure and/or outcome is made.
The advantage of such studies is that subjects are neither deliberately exposed, treated, or not treated and hence there are seldom ethical difficulties. Only one group is used, data are collected only once and multiple outcomes can be studied; thus this type of study is relatively cheap.
Many cross sectional studies are done using questionnaires. Alternatively each of the subjects may be interviewed. Table 2 lists the advantages and disadvantages of each.
Any study with a low response rate can be criticised because it can miss significant differences in the responders and non-responders. At its most extreme all the non-responders could be dead! Strenuous efforts must be made to maximise the numbers who do respond. The use of volunteers is also problematic because they too are unlikely to be representative of the general population. A good way to produce a valid sample would be to randomly select people from the electoral role and invite them to complete a questionnaire. In this way the response rate is known and non-responders can be identified. However, the electoral role itself is not an entirely accurate reflection of the general population. A census is another example of a cross sectional study.
Market research organisations often use cross sectional studies (for example, opinion polls). This entails a system of quotas to ensure the sample is representative of the age, sex, and social class structure of the population being studied. However, to be commercially viable they are convenience samples—only people available can be questioned. This technique is insufficiently rigorous to be used for medical research.
How to run a cross sectional study
Formulate the research question(s) and choose the sample population. Then decide what variables of the study population are relevant to the research question. A method for contacting sample subjects must be devised and then implemented. In this way the data are collected and can then be analysed
The most important advantage of cross sectional studies is that in general they are quick and cheap. As there is no follow up, less resources are required to run the study.
Cross sectional studies are the best way to determine prevalence and are useful at identifying associations that can then be more rigorously studied using a cohort study or randomised controlled study.
The most important problem with this type of study is differentiating cause and effect from simple association. For example, a study finding an association between low CD4 counts and HIV infection does not demonstrate whether HIV infection lowers CD4 levels or low CD4 levels predispose to HIV infection. Moreover, male homosexuality is associated with both but causes neither. (Another example of a confounding variable).
Often there are a number of plausible explanations. For example, if a study shows a negative relation between height and age it could be concluded that people lose height as they get older, younger generations are getting taller, or that tall people have a reduced life expectancy when compared with short people. Cross sectional studies do not provide an explanation for their findings.
Rare conditions cannot efficiently be studied using cross sectional studies because even in large samples there may be no one with the disease. In this situation it is better to study a cross sectional sample of patients who already have the disease (a case series). In this way it was found in 1983 that of 1000 patients with AIDS, 727 were homosexual or bisexual men and 236 were intrvenous drug abusers. 6 The conclusion that individuals in these two groups had a higher relative risk was inescapable. The natural history of HIV infection was then studied using cohort studies and efficacy of treatments via case controlled studies and randomised clinical trials.
An example of a cross sectional study was the prevalence study of skull fractures in children admitted to hospital in Edinburgh from 1983 to 1989. 7 Note that although the study period was seven years it was not a longitudinal or cohort study because information about each subject was recorded at a single point in time.
A questionnaire based cross sectional study explored the relation between A&E attendance and alcohol consumption in elderly persons. 9
A recent example can be found in the BMJ , in which the prevalence of serious eye disease in a London population was evaluated. 10
Cross sectional studies
Cross sectional studies are the best way to determine prevalence
Are relatively quick
Can study multiple outcomes
Do not themselves differentiate between cause and effect or the sequence of events
CASE-CONTROL STUDIES
In contrast with cohort and cross sectional studies, case-control studies are usually retrospective. People with the outcome of interest are matched with a control group who do not. Retrospectively the researcher determines which individuals were exposed to the agent or treatment or the prevalence of a variable in each of the study groups. Where the outcome is rare, case-control studies may be the only feasible approach.
As some of the subjects have been deliberately chosen because they have the disease in question case-control studies are much more cost efficient than cohort and cross sectional studies—that is, a higher percentage of cases per study.
Case-control studies determine the relative importance of a predictor variable in relation to the presence or absence of the disease. Case-control studies are retrospective and cannot therefore be used to calculate the relative risk; this a prospective cohort study. Case-control studies can however be used to calculate odds ratios, which in turn, usually approximate to the relative risk.
How to run a case-control study
Decide on the research question to be answered. Formulate an hypothesis and then decide what will be measured and how. Specify the characteristics of the study group and decide how to construct a valid control group. Then compare the “exposure” of the two groups to each variable.
When conditions are uncommon, case-control studies generate a lot of information from relatively few subjects. When there is a long latent period between an exposure and the disease, case-control studies are the only feasible option. Consider the practicalities of a cohort study or cross sectional study in the assessment of new variant CJD and possible aetiologies. With less than 300 confirmed cases a cross sectional study would need about 200 000 subjects to include one symptomatic patient. Given a postulated latency of 10 to 30 years a cohort study would require both a vast sample size and take a generation to complete.
In case-control studies comparatively few subjects are required so more resources are available for studying each. In consequence a huge number of variables can be considered. This type of study is therefore useful for generating hypotheses that can then be tested using other types of study.
This flexibility of the variables studied comes at the expense of the restricted outcomes studied. The only outcome is the presence or absence of the disease or whatever criteria was chosen to select the cases.
The major problems with case-control studies are the familiar ones of confounding variables (see above) and bias. Bias may take two major forms.
Sampling bias
The patients with the disease may be a biased sample (for example, patients referred to a teaching hospital) or the controls may be biased (for example, volunteers, different ages, sex or socioeconomic group).
Observation and recall bias
As the study assesses predictor variables retrospectively there is great potential for a biased assessment of their presence and significance by the patient or the investigator, or both.
Overcoming sampling bias
Ideally the cases studied should be a random sample of all the patients with the disease. This is not only very difficult but in many instances is impossible because many cases may not have been diagnosed or have been misdiagnosed. For example, many cases of non-insulin dependent diabetes will not have sought medical attention and therefore be undiagnosed. Conversely many psychiatric diseases may be differently labelled in different countries and even by different doctors in the same country. As a result they will be misdiagnosed for the purposes of the study. However, in reality you are often left studying a sample of those patients who it is possible to recruit. Selecting the controls is often a more difficult problem.
To enable the controls to represent the same population as the cases, one of four techniques may be used.
A convenience sample—sampled in the same way as the cases, for example, attending the same outpatient department. While this is certainly convenient it may reduce the external validity of the study.
Matching—the controls may be a matched or unmatched random sample from the unaffected population. Again the problems of controlling for unknown influences is present but if the controls are too closely matched they may not be representative of the general population. “Over matching” may cause the true difference to be underestimated.
The advantage of matching is that it allows a smaller sample size for any given effect to be statistically significant.
Using two or more control groups. If the study demonstrates a significant difference between the patients with the outcome of interest and those without, even when the latter have been sampled in a number of different ways (for example, outpatients, in patients, GP patients) then the conclusion is more robust.
Using a population based sample for both cases and controls. It is possible to take a random sample of all the patients with a particular disease from specific registers. The control group can then be constructed by selecting age and sex matched people randomly selected from the same population as the area covered by the disease register.
Overcoming observation and recall bias
Overcoming retrospective recall bias can be achieved by using data recorded, for other purposes, before the outcome had occurred and therefore before the study had started. The success of this strategy is limited by the availability and reliability of the data collected. Another technique is blinding where neither the subject nor the observer know if they are a case or control subject. Nor are they aware of the study hypothesis. In practice this is often difficult or impossible and only partial blinding is practicable. It is usually possible to blind the subjects and observers to the study hypothesis by asking spurious questions. Observers can also be easily blinded to the case or control status of the patient where the relevant observation is not of the patient themselves but a laboratory test or radiograph.
Case-control studies
Case-control studies are simple to organise
Retrospectively compare two groups
Aim to identify predictors of an outcome
Permit assessment of the influence of predictors on outcome via calculation of an odds ratio
Useful for hypothesis generation
Can only look at one outcome
Bias is an major problem
Blinding cases to their case or control status is usually impracticable as they already know that they have a disease or illness. Similarly observers can hardly be blinded to the presence of physical signs, for example, cyanosis or dyspnoea.
As a result of the problems of matching, bias and confounding, case-control studies, are often flawed. They are however useful for generating hypotheses. These hypotheses can then be tested more rigorously by other methods—randomised controlled trials or cohort studies.
Case-control studies are very common. They are particularly useful for studying infrequent events, for example, cot death, survival from out of hospital cardiac arrest, and toxicological emergencies.
A recent example was the study of atrial fibrillation in middle aged men during exercise. 11
USING DATABASES FOR RESEARCH (SECONDARY DATA)
Pre-existing databases provide an excellent and convenient source of data. There are a host of such databases and the increasing archiving of information on computers means that this is an enlarging area for obtaining data. Table 3 lists some common examples of potentially useful databases.
Such databases enable vast numbers of people to be entered into a study prospectively or retrospectively. They can be used to construct a cohort, to produce a sample for a cross sectional study, or to identify people with certain conditions or outcomes and produce a sample for a case controlled study. A recent study used census data from 11 countries to look at the relation between social class and mortality in middle aged men. 12
These type of data are ordinarily collected by people other than the researcher and independently of any specific hypothesis. The opportunity for observer bias is thus diminished. The use of previously collected data is efficient and comparatively inexpensive and moreover the data are collected in a very standardised way, permitting comparisons over time and between different countries. However, because the data are collected for other purposes it may not be ideally suited to the testing of the current hypothesis, additionally it may be incomplete. This may result in sampling bias. For example, the electoral roll depends upon registration by each individual. Many homeless, mentally ill, and chronically sick people will not be registered. Similarly the notification of certain communicable diseases is a statutory responsibility for doctors in the UK: while it is probable that most cases of cholera are reported it is highly unlikely that most cases of food poisoning are.
Causes and associations
Because observational studies are not experiments (as are randomised controlled trials) it is difficult to control many external variables. In consequence when faced with a clear and significant association between some form of illness or cause of death and some environmental influence a judgement has to be made as to whether this is a causal link or simply an association. Table 4 outlines the points to be considered when making this judgement. 13
None of these judgements can provide indisputable evidence of cause and effect, but taken together they do permit the investigator to answer the fundamental questions “is there any other way to explain the available evidence?” and is there any other more likely than cause and effect?”
Qualitative studies can produce high quality information but all such studies can be influenced by known and unknown confounding variables. Appropriate use of observational studies permits investigation of prevalence, incidence, associations, causes, and outcomes. Where there is little evidence on a subject they are cost effective ways of producing and investigating hypotheses before larger and more expensive study designs are embarked upon. In addition they are often the only realistic choice of research methodology, particularly where a randomised controlled trial would be impractical or unethical.
Cohort studies look forwards in time by following up each subject
Subjects are selected before the outcome of interest is observed
They establish the sequence of events
Numerous outcomes can be studied
They are the best way to establish the incidence of a disease
They are a good way to determine causes of diseases
The principal summary statistic of cohort studies is the relative risk ratio
If prospective, they are expensive and often take a long time for sufficient outcome events to occur to produce meaningful results
Cross sectional studies look at each subject at one point in time only
Subjects are selected without regard to the outcome of interest
Less expensive
They are the best way to determine prevalence
The principal summary statistic of cross sectional studies is the odds ratio
Weaker evidence of causality than cohort studies
Inaccurate when studying rare conditions
Case-control studies look back at what has happened to each subject
Subjects are selected specifically on the basis of the outcome of interest
Efficient (small sample sizes)
Produce odds ratios that approximate to relative risks for each variable studied
Prone to sampling bias and retrospective analysis bias
Only one outcome is studied
GLOSSARY OF TERMS
The inclusion of subjects or methods such that the results obtained are not truly representative of the population from which it is drawn
The process by which the researcher and or the subject is ignorant of which intervention or exposure has occurred.
Cochrane database
An international collaborative project collating peer reviewed prospective randomised clinical trials.
Is a component of a population identified so that one or more characteristic can be studied as it ages through time.
Confounding variable
A variable that is associated with both the exposure and outcome of interest that is not the variable being studied.
A group of people without the condition of interest, or unexposed to or not treated with the agent of interest.
False positive
A test result that suggests that the subject has a specific disease or condition when in fact the subject does not.
Is a rate and therefore is always related either explicitly or by implication to a time period. With regard to disease it can be defined as the number of new cases that develop during a specified time interval.
A period of time between exposure to an agent and the development of symptoms, signs, or other evidence of changes associated with that exposure.
The process by which each case is matched with one or more controls, which have been deliberately chosen to be as similar as the test subjects in all regards other than the variable being studied.
Observational study
A study in which no intervention is made (in contrast with an experimental study). Such studies provide estimates and examine associations of events in their natural settings without recourse to experimental intervention.
The ratio of the probability of an event occurring to the probability of non-occurrence. In a clinical setting this would be equivalent to the odds of a condition occurring in the exposed group divided by the odds of it occurring in the non-exposed group.
Is not defined by a time interval and is therefore not a rate. It may be defined as the number of cases of a disease that exist in a defined population at a specified point in time.
Randomised controlled trial
Subjects are assigned by statistically randomised methods to two or more groups. In doing so it is assumed that all variables other than the proposed intervention are evenly distributed between the groups. In this way bias is minimised.
Relative risk
This is the ratio of the probability of developing the condition if exposed to a certain variable compared with the probability if not exposed.
Response rate
The proportion of subjects who respond to either a treatment or a questionnaire.
Risk factor
A variable associated with a specific disease or outcome.
Validity—internal
The rigour with which a study has been designed and executed—that is, can the conclusion be relied upon?
Validity—external
The usefulness of the findings of a study with respect to other populations.
A value or quality that can vary between subjects and/or over time
- Download figure
- Open in new tab
- Download powerpoint
Study design for cohort studies.
Study design for cross sectional studies
Study design for case-control studies.
- Fowkes F , Fulton P. Critical appraisal of published research: introductory guidelines. BMJ 1991 ; 302 : 1136 –40.
- ↵ Lerner DJ , Kannel WB. Patterns of coronary heart disease morbidity and mortality in the sexes: a 26 year follow-up of the Framingham population. Am Heart J 1986 ; 111 : 383 –90. OpenUrl CrossRef PubMed Web of Science
- ↵ Doll R , Peto H. Mortality in relation to smoking. 40 years observation on female British doctors. BMJ 1989 ; 208 : 967 –73. OpenUrl
- ↵ Alberman ED , Butler NR, Sheridan MD. Visual acuity of a national sample (1958 cohort) at 7 years. Dev Med Child Neurol 1971 ; 13 : 9 –14. OpenUrl PubMed Web of Science
- ↵ Davey Smith G , Hart C, Blane D, et al . Adverse socioeconomic conditions in childhood and cause specific mortality: prospective observational study. BMJ 1998 ; 316 : 1631 –5. OpenUrl Abstract / FREE Full Text
- ↵ Goyder EC , Goodacre SW, Botha JL, et al . How do individuals with diabetes use the accident and emergency department? J Accid Emerg Med 1997 ; 14 : 371 –4. OpenUrl Abstract / FREE Full Text
- ↵ Jaffe HW , Bregman DJ, Selik RM. Acquired immune deficiency in the US: the first 1000 cases. J Inf Dis 1983 ; 148 : 339 –45. OpenUrl Abstract / FREE Full Text
- Johnstone AJ , Zuberi SH, Scobie WH. Skull fractures in children: a population study. J Accid Emerg Med 1996 ; 13 : 386 –9. OpenUrl Abstract / FREE Full Text
- ↵ van der Pol V , Rodgers H, Aitken P, et al . Does alcohol contribute to accident and emergency department attendance in elderly people? J Accid Emerg Med 1996 ; 13 : 258 –60. OpenUrl Abstract / FREE Full Text
- ↵ Reidy A , Minassian DC, Vafadis G, et al . BMJ 1998 ; 316 : 1643 –7. OpenUrl Abstract / FREE Full Text
- ↵ Karjaleinen , Kujala U, Kaprio J, et al . BMJ 1998 ; 316 : 1784 –5. OpenUrl FREE Full Text
- ↵ Kunst A , Groenhof F, Mackenbach J. BMJ 1998 ; 316 : 1636 –42. OpenUrl Abstract / FREE Full Text
- ↵ Hill AB , Hill ID. Bradford Hills principles of medical statistics. 12th edn. London: Edward Arnold, 1991.
Read the full text or download the PDF:
Together we are beating cancer
About cancer
Cancer types
- Breast cancer
- Bowel cancer
- Lung cancer
- Prostate cancer
Cancers in general
- Clinical trials
- Causes of cancer
Coping with cancer
- Managing symptoms and side effects
- Mental health and cancer
- Money and travel
- Death and dying
- Cancer Chat forum
Health Professionals
- Cancer Statistics
- Cancer Screening
- Learning and Support
- NICE suspected cancer referral guidelines
Get involved
- Make a donation
By cancer type
- Leave a legacy gift
- Donate in Memory
Find an event
- Race for Life
- Charity runs
- Charity walks
- Search events
- Relay For Life
- Volunteer in our shops
- Help at an event
- Help us raise money
- Campaign for us
Do your own fundraising
- Fundraising ideas
- Get a fundraising pack
- Return fundraising money
- Fundraise by cancer type
- Set up a Cancer Research UK Giving Page
- Find a shop or superstore
- Become a partner
- Cancer Research UK for Children & Young People
- Our We Are campaign
Our research
- Brain tumours
- Skin cancer
- All cancer types
By cancer topic
- New treatments
- Cancer biology
- Cancer drugs
- All cancer subjects
- All locations
By Researcher
- Professor Duncan Baird
- Professor Fran Balkwill
- Professor Andrew Biankin
- See all researchers
- Our achievements timeline
- Our research strategy
- Involving animals in research
Funding for researchers
Research opportunities
- For discovery researchers
- For clinical researchers
- For population researchers
- In drug discovery & development
- In early detection & diagnosis
- For students & postdocs
Our funding schemes
- Career Development Fellowship
- Discovery Programme Awards
- Clinical Trial Award
- Biology to Prevention Award
- View all schemes and deadlines
Applying for funding
- Start your application online
- How to make a successful application
- Funding committees
- Successful applicant case studies
How we deliver research
- Our research infrastructure
- Events and conferences
- Our research partnerships
- Facts & figures about our funding
- Develop your research career
- Recently funded awards
- Manage your research grant
- Notify us of new publications
Find a shop
- Volunteer in a shop
- Donate goods to a shop
- Our superstores
Shop online
- Wedding favours
- Cancer Care
- Flower Shop
Our eBay store
- Shoes and boots
- Bags and purses
- We beat cancer
- We fundraise
- We develop policy
- Our global role
Our organisation
- Our strategy
- Our Trustees
- CEO and Executive Board
- How we spend your money
- Early careers
Cancer news
- Cancer News
- For Researchers
- For Supporters
- Press office
- Publications
- Update your contact preferences
ABOUT CANCER
GET INVOLVED
NEWS & RESOURCES
FUNDING & RESEARCH
You are here
- Types of clinical trials
Medical research studies involving people are called clinical trials.
There are two main types of trials or studies - interventional and observational.
Interventional trials aim to find out more about a particular intervention, or treatment. A computer puts people taking part into different treatment groups. This is so that the research team can compare the results.
Observational studies aim to find out what happens to people in different situations. The research team observe the people taking part, but they don’t influence what treatments people have. The people taking part aren’t put into treatment groups.
There are different types of trials within these two groups. This page has information about
Pilot studies and feasibility studies
Prevention trials, screening trials, treatment trials, multi-arm multi-stage (mams) trials, cohort studies.
Case control studies
Cross sectional studies
Pilot studies and feasibility studies are small versions of studies which are sometimes done before a large trial takes place.
Feasibility studies are designed to see if it is possible to do the main study. They aim to find out things such as whether patients and doctors are happy to take part, and how long it might take to collect and analyse the information. They don’t answer the main research question about how well a treatment works.
Pilot studies are small versions of the main study. Pilot studies help to test that all the main parts of the study work together. They may also help answer the research question. Sometimes the research team include the information collected during the pilot study in the results of the main study.
Prevention trials look at whether a particular treatment can help prevent cancer. The people taking part don't have cancer.
These trials can be for the general population or for people who have a higher than normal risk of developing a certain cancer. For example, this could include people with a strong family history of cancer.
Screening tests people for the early signs of cancer before they have any symptoms. As with prevention trials, screening trials can be for the general population. Or they can be for a group of people who have a higher than normal risk of developing a certain cancer.
Researchers may plan screening trials to see if new tests are reliable enough to detect particular types of cancer. Or they may try to find out if there is an overall benefit in picking up the cancer early.

For trials that compare two or more treatments, you are put into a treatment group at random. This is a randomised trial. They are the best way to get reliable information about how well a new treatment works. We have more information about randomisation .
A multi arm trial is a trial that has:
- several treatment groups as well as
Multi-arm multi-stage (MAMS) trials have the same control group all the way through. The other treatment groups can change as the trial goes on. As these trials are more complex there are a number of treatments that people might have.
The research team may decide to stop recruiting people to a particular group. This could be because they have enough people to start looking at the results. Or because early results show the treatment isn’t working as well as they’d hoped.
The researchers may add new treatment groups as new drugs become available to look at. This means they don’t have to design and launch a brand new trial each time they want to research a new treatment. So it helps get results quicker.
The Stampede trial for prostate cancer is an example of a MAMS trial.
Observational studies Cohort studies, case control studies and cross sectional studies are all types of observational studies.
A cohort is a group of people, so cohort studies look at groups of people. A cohort study follows the group over a period of time.
A research team may recruit people who do not have cancer and collect information about them for a number of years. The researchers see who in the group develops cancer and who doesn’t. They then look to see whether the people who developed cancer had anything in common.
Cohort studies are very useful ways of finding out more about risk factors. But they are expensive and time consuming. They can be used when it wouldn’t be possible to test a theory any other way.
Case control studies
Case control studies work the opposite way to cohort studies. The research team recruits a group of people who have a disease (cases) and a group of people who don't (controls). They then look back to see how many people in each group were exposed to a certain risk factor.
Researchers want to make the results as reliable as possible. So they try to make sure the people in each group have the same general factors such as age or gender.
Case control studies are useful and they are quicker and cheaper than cohort studies. But the results may be less reliable. The research team often rely on people thinking back and remembering whether they were exposed to a certain risk factor or not. But people may not remember accurately, and this can affect the results.
Another issue is the difference between association and cause. Just because there is an association between a factor and a disease, it doesn’t mean that the factor causes the disease.
For example, a case control study may show that people with a lower income are more likely to develop cancer. But it doesn’t mean that the level of income itself causes cancer. It may mean that they have a poor diet or are more likely to smoke.
Cross sectional studies
Cross sectional studies are carried out at one point in time, or over a short period of time. They find out who has been exposed to a risk factor and who has developed cancer, and see if there is a link.
Cross sectional studies are quicker and cheaper to do. But the results can be less useful. Sometimes researchers do a cross sectional study first to find a possible link. Then they go on to do a case control or cohort study to look at the issue in more detail.
Oxford Handbook of Clinical and Healthcare Research (1st edition) R Sumantra, S Fitzpatrick, R Golubic and others Oxford University Press, 2016
Related information
You may find it helpful to read our information about:
What trials are
- Phases of clinical trials
Finding a clinical trial
Last reviewed
Find a trial, about cancer.
- Spot cancer early
- Talking to your doctor
- What is cancer?
- Randomised trials
- How to find a clinical trial
- How to join a clinical trial
- What you should be told about a clinical trial
- How clinical trials are planned and organised
- Clinical trial results
- What to ask your doctor about clinical trials
- Clinical trial organisations
- Children's Cancers
- Sign up for relevant cancer information and support
- How do I check for cancer?
- Welcome to Cancer Chat
Rate this page:

Research Methods (Case Studies & Observation Studies) 0 Pages | Leaving School | 27/04/2024
- Case Studies & Observation Studies

——————————————————
Observation Studies

Categories of behaviour: If the researcher is undertaking a natural observation , he may need to divide the behaviour he sees into categories so that a quick record can be made. If the researcher wants to understand how the public respond to a woman collapsing in the street, for example, his categories might include 1.) Ignores and walks on. 2.) Hesitates and walks on. 3.) Checks to see if the woman is ok. 4.) Calls 999.
Inter-observer reliability: In order to test the reliability of an observer’s records, it might be sensible to have two observers who are working to exactly the same category and score sheet, so that they can compare their results at the end of the observation period. If these observations closely match each other then it can be assumed their observations have been accurate. If there is a significant difference it may be necessary to start the observation over again.
Advantages of natural observation Natural observations are high in ecological validity . A string of natural actions can be observed. In a laboratory situation people are often asked to complete unnatural tasks.
Disadvantages of natural observation In the absence ofcontrolled variables it is difficult to establish why someone behaved in a certain way. This type of study is reliant on the accuracy of the observation. There are ethical issues involved in an observation of this kind i.e. the people being observed may not know that this is the case. Should they be told? And if they are told, would their behaviour still be natural? Natural observations can be awkward to plan as well as time consuming.
- Research Methods
- Hypotheses and Experimental Designs
- Standardised Procedures & Instructions
- Ecological Validity & Sampling Methods
- Making Sense of Data & Anomalous Results
- Survey Methods & Ethical Considerations
- Remember it, Test it!
ADVERTISEMENTS
Observational vs. Experimental Study: A Comprehensive Guide
Explore the fundamental disparities between experimental and observational studies in this comprehensive guide by Santos Research Center, Corp. Uncover concepts such as control group, random sample, cohort studies, response variable, and explanatory variable that shape the foundation of these methodologies. Discover the significance of randomized controlled trials and case control studies, examining causal relationships and the role of dependent variables and independent variables in research designs.
This enlightening exploration also delves into the meticulous scientific study process, involving survey members, systematic reviews, and statistical analyses. Investigate the careful balance of control group and treatment group dynamics, highlighting how researchers meticulously assign variables and analyze statistical patterns to discern meaningful insights. From dissecting issues like lung cancer to understanding sleep patterns, this guide emphasizes the precision of controlled experiments and controlled trials, where variables are isolated and scrutinized, paving the way for a deeper comprehension of the world through empirical research.
Introduction to Observational and Experimental Studies
These two studies are the cornerstones of scientific inquiry, each offering a distinct approach to unraveling the mysteries of the natural world.
Observational studies allow us to observe, document, and gather data without direct intervention. They provide a means to explore real-world scenarios and trends, making them valuable when manipulating variables is not feasible or ethical. From surveys to meticulous observations, these studies shed light on existing conditions and relationships.
Experimental studies , in contrast, put researchers in the driver's seat. They involve the deliberate manipulation of variables to understand their impact on specific outcomes. By controlling the conditions, experimental studies establish causal relationships, answering questions of causality with precision. This approach is pivotal for hypothesis testing and informed decision-making.
At Santos Research Center, Corp., we recognize the importance of both observational and experimental studies. We employ these methodologies in our diverse research projects to ensure the highest quality of scientific investigation and to answer a wide range of research questions.
Observational Studies: A Closer Look
In our exploration of research methodologies, let's zoom in on observational research studies—an essential facet of scientific inquiry that we at Santos Research Center, Corp., expertly employ in our diverse research projects.
What is an Observational Study?
Observational research studies involve the passive observation of subjects without any intervention or manipulation by researchers. These studies are designed to scrutinize the relationships between variables and test subjects, uncover patterns, and draw conclusions grounded in real-world data.
Researchers refrain from interfering with the natural course of events in controlled experiment. Instead, they meticulously gather data by keenly observing and documenting information about the test subjects and their surroundings. This approach permits the examination of variables that cannot be ethically or feasibly manipulated, making it particularly valuable in certain research scenarios.
Types of Observational Studies
Now, let's delve into the various forms that observational studies can take, each with its distinct characteristics and applications.
Cohort Studies: A cohort study is a type of observational study that entails tracking one group of individuals over an extended period. Its primary goal is to identify potential causes or risk factors for specific outcomes or treatment group. Cohort studies provide valuable insights into the development of conditions or diseases and the factors that influence them.
Case-Control Studies: Case-control studies, on the other hand, involve the comparison of individuals with a particular condition or outcome to those without it (the control group). These studies aim to discern potential causal factors or associations that may have contributed to the development of the condition under investigation.
Cross-Sectional Studies: Cross-sectional studies take a snapshot of a diverse group of individuals at a single point in time. By collecting data from this snapshot, researchers gain insights into the prevalence of a specific condition or the relationships between variables at that precise moment. Cross-sectional studies are often used to assess the health status of the different groups within a population or explore the interplay between various factors.
Advantages and Limitations of Observational Studies
Observational studies, as we've explored, are a vital pillar of scientific research, offering unique insights into real-world phenomena. In this section, we will dissect the advantages and limitations that characterize these studies, shedding light on the intricacies that researchers grapple with when employing this methodology.
Advantages: One of the paramount advantages of observational studies lies in their utilization of real-world data. Unlike controlled experiments that operate in artificial settings, observational studies embrace the complexities of the natural world. This approach enables researchers to capture genuine behaviors, patterns, and occurrences as they unfold. As a result, the data collected reflects the intricacies of real-life scenarios, making it highly relevant and applicable to diverse settings and populations.
Moreover, in a randomized controlled trial, researchers looked to randomly assign participants to a group. Observational studies excel in their capacity to examine long-term trends. By observing one group of subjects over extended periods, research scientists gain the ability to track developments, trends, and shifts in behavior or outcomes. This longitudinal perspective is invaluable when studying phenomena that evolve gradually, such as chronic diseases, societal changes, or environmental shifts. It allows for the detection of subtle nuances that may be missed in shorter-term investigations.
Limitations: However, like any research methodology, observational studies are not without their limitations. One significant challenge of statistical study lies in the potential for biases. Since researchers do not intervene in the subjects' experiences, various biases can creep into the data collection process. These biases may arise from participant self-reporting, observer bias, or selection bias in random sample, among others. Careful design and rigorous data analysis are crucial for mitigating these biases.
Another limitation is the presence of confounding variables. In observational studies, it can be challenging to isolate the effect of a specific variable from the myriad of other factors at play. These confounding variables can obscure the true relationship between the variables of interest, making it difficult to establish causation definitively. Research scientists must employ statistical techniques to control for or adjust these confounding variables.
Additionally, observational studies face constraints in their ability to establish causation. While they can identify associations and correlations between variables, they cannot prove causality or causal relationship. Establishing causation typically requires controlled experiments where researchers can manipulate independent variables systematically. In observational studies, researchers can only infer potential causation based on the observed associations.
Experimental Studies: Delving Deeper
In the intricate landscape of scientific research, we now turn our gaze toward experimental studies—a dynamic and powerful method that Santos Research Center, Corp. skillfully employs in our pursuit of knowledge.
What is an Experimental Study?
While some studies observe and gather data passively, experimental studies take a more proactive approach. Here, researchers actively introduce an intervention or treatment to an experiment group study its effects on one or more variables. This methodology empowers researchers to manipulate independent variables deliberately and examine their direct impact on dependent variables.
Experimental research are distinguished by their exceptional ability to establish cause-and-effect relationships. This invaluable characteristic allows researchers to unlock the mysteries of how one variable influences another, offering profound insights into the scientific questions at hand. Within the controlled environment of an experimental study, researchers can systematically test hypotheses, shedding light on complex phenomena.
Key Features of Experimental Studies
Central to statistical analysis, the rigor and reliability of experimental studies are several key features that ensure the validity of their findings.
Randomized Controlled Trials: Randomization is a critical element in experimental studies, as it ensures that subjects are assigned to groups in a random assignment. This randomly assigned allocation minimizes the risk of unintentional biases and confounding variables, strengthening the credibility of the study's outcomes.
Control Groups: Control groups play a pivotal role in experimental studies by serving as a baseline for comparison. They enable researchers to assess the true impact of the intervention being studied. By comparing the outcomes of the intervention group to those of survey members of the control group, researchers can discern whether the intervention caused the observed changes.
Blinding: Both single-blind and double-blind techniques are employed in experimental studies to prevent biases from influencing the study or controlled trial's outcomes. Single-blind studies keep either the subjects or the researchers unaware of certain aspects of the study, while double-blind studies extend this blindness to both parties, enhancing the objectivity of the study.
These key features work in concert to uphold the integrity and trustworthiness of the results generated through experimental studies.
Advantages and Limitations of Experimental Studies
As with any research methodology, this one comes with its unique set of advantages and limitations.
Advantages: These studies offer the distinct advantage of establishing causal relationships between two or more variables together. The controlled environment allows researchers to exert authority over variables, ensuring that changes in the dependent variable can be attributed to the independent variable. This meticulous control results in high-quality, reliable data that can significantly contribute to scientific knowledge.
Limitations: However, experimental ones are not without their challenges. They may raise ethical concerns, particularly when the interventions involve potential risks to subjects. Additionally, their controlled nature can limit their real-world applicability, as the conditions in experiments may not accurately mirror those in the natural world. Moreover, executing an experimental study in randomized controlled, often demands substantial resources, with other variables including time, funding, and personnel.
Observational vs Experimental: A Side-by-Side Comparison
Having previously examined observational and experimental studies individually, we now embark on a side-by-side comparison to illuminate the key distinctions and commonalities between these foundational research approaches.
Key Differences and Notable Similarities
Methodologies
- Observational Studies : Characterized by passive observation, where researchers collect data without direct intervention, allowing the natural course of events to unfold.
- Experimental Studies : Involve active intervention, where researchers deliberately manipulate variables to discern their impact on specific outcomes, ensuring control over the experimental conditions.
- Observational Studies : Designed to identify patterns, correlations, and associations within existing data, shedding light on relationships within real-world settings.
- Experimental Studies : Geared toward establishing causality by determining the cause-and-effect relationships between variables, often in controlled laboratory environments.
- Observational Studies : Yield real-world data, reflecting the complexities and nuances of natural phenomena.
- Experimental Studies : Generate controlled data, allowing for precise analysis and the establishment of clear causal connections.
Observational studies excel at exploring associations and uncovering patterns within the intricacies of real-world settings, while experimental studies shine as the gold standard for discerning cause-and-effect relationships through meticulous control and manipulation in controlled environments. Understanding these differences and similarities empowers researchers to choose the most appropriate method for their specific research objectives.
When to Use Which: Practical Applications
The decision to employ either observational or experimental studies hinges on the research objectives at hand and the available resources. Observational studies prove invaluable when variable manipulation is impractical or ethically challenging, making them ideal for delving into long-term trends and uncovering intricate associations between certain variables (response variable or explanatory variable). On the other hand, experimental studies emerge as indispensable tools when the aim is to definitively establish causation and methodically control variables.
At Santos Research Center, Corp., our approach to both scientific study and methodology is characterized by meticulous consideration of the specific research goals. We recognize that the quality of outcomes hinges on selecting the most appropriate method of research study. Our unwavering commitment to employing both observational and experimental research studies further underscores our dedication to advancing scientific knowledge across diverse domains.
Conclusion: The Synergy of Experimental and Observational Studies in Research
In conclusion, both observational and experimental studies are integral to scientific research, offering complementary approaches with unique strengths and limitations. At Santos Research Center, Corp., we leverage these methodologies to contribute meaningfully to the scientific community.
Explore our projects and initiatives at Santos Research Center, Corp. by visiting our website or contacting us at (813) 249-9100, where our unwavering commitment to rigorous research practices and advancing scientific knowledge awaits.
Recent Posts
Learn everything about Respiratory Syncytial Virus (RSV), from symptoms and diagnosis to treatment and prevention. Stay informed and protect your health with...
Discover key insights on Alzheimer's disease, including symptoms, stages, and care tips. Learn how to manage the condition and find out how you can...
Discover expert insights on migraines, from symptoms and causes to management strategies, and learn about our specialized support at Santos Research Center.
Explore our in-depth guide on UTIs, covering everything from symptoms and causes to effective treatments, and learn how to manage and prevent urinary tract infections.
Your definitive guide to COVID symptoms. Dive deep into the signs of COVID-19, understand the new variants, and get answers to your most pressing questions.
Unravel the differences between observational and experimental studies. Dive into the intricacies of each method and discover their unique applications in research.
Discover the different types of clinical trials and their significance in advancing medical science. Dive deep into the world of clinical research with Santos Research Center.
Santos Research Center, Corp. is a research facility conducting paid clinical trials, in partnership with major pharmaceutical companies & CROs. We work with patients from across the Tampa Bay area.
Contact Details
Navigation menu.
If you're seeing this message, it means we're having trouble loading external resources on our website.
If you're behind a web filter, please make sure that the domains *.kastatic.org and *.kasandbox.org are unblocked.
To log in and use all the features of Khan Academy, please enable JavaScript in your browser.
Statistics and probability
Course: statistics and probability > unit 6.
- Types of statistical studies
- Worked example identifying experiment
- Worked example identifying observational study
- Worked example identifying sample study
Observational studies and experiments
- Appropriate statistical study example
- In an observational study, we measure or survey members of a sample without trying to affect them.
- In a controlled experiment, we assign people or things to groups and apply some treatment to one of the groups, while the other group does not receive the treatment.
Problem 1: Drinking tea before bedtime
- (Choice A) Observational study A Observational study
- (Choice B) Experiment B Experiment
Problem 2: Social media and happiness
- One group was directed to use social media sites as they usually do.
- One group was blocked from social media sites.
Want to join the conversation?
- Upvote Button navigates to signup page
- Downvote Button navigates to signup page
- Flag Button navigates to signup page

Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- My Account Login
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Open access
- Published: 29 April 2024
Cognitive profile in multiple sclerosis and post-COVID condition: a comparative study using a unified taxonomy
- Cristina Delgado-Alonso 1 ,
- Alfonso Delgado-Alvarez 1 ,
- María Díez-Cirarda 1 ,
- Silvia Oliver-Mas 1 ,
- Constanza Cuevas 1 ,
- Paloma Montero-Escribano 1 ,
- Ana Maria Ramos-Leví 2 ,
- María José Gil-Moreno 1 ,
- Juan Ignacio López-Carbonero 1 ,
- Bruce P. Hermann 3 ,
- Jorge Matias-Guiu 1 &
- Jordi A. Matias-Guiu ORCID: orcid.org/0000-0001-5520-2708 1
Scientific Reports volume 14 , Article number: 9806 ( 2024 ) Cite this article
Metrics details
- Central nervous system infections
- Multiple sclerosis
Post-COVID condition (PCC) and multiple sclerosis (MS) share some clinical and demographic features, including cognitive symptoms and fatigue. Some pathophysiological mechanisms well-known in MS, such as autoimmunity, neuroinflammation and myelin damage, have also been implicated in PCC. In this study, we aimed to compare the cognitive phenotypes of two large cohorts of patients with PCC and MS, and to evaluate the relationship between fatigue and cognitive performance. Cross-sectional study including 218 patients with PCC and 218 with MS matched by age, sex, and years of education. Patients were evaluated with a comprehensive neuropsychological protocol and were categorized according to the International Classification of Cognitive Disorders system. Fatigue and depression were also assessed. Cognitive profiles of PCC and MS largely overlapped, with a greater impairment in episodic memory in MS, but with small effect sizes. The most salient deficits in both disorders were in attention and processing speed. The severity of fatigue was greater in patients with PCC. Still, the correlations between fatigue severity and neuropsychological tests were more prominent in the case of MS. There were no differences in the severity of depression among groups. Our study found similar cognitive profiles in PCC and MS. Fatigue was more severe in PCC, but was more associated with cognitive performance in MS. Further comparative studies addressing the mechanisms related to cognitive dysfunction and fatigue may be of interest to advance the knowledge of these disorders and develop new therapies.
Introduction
Cognitive dysfunction and fatigue are commonly reported after the acute phase of SARS-CoV-2 infection and have been emphasized as the most frequent symptoms by the World Health Organization in the post-COVID condition or Long-COVID (PCC) 1 . Several studies have confirmed the presence of objective cognitive deficits in neuropsychological assessments 2 , 3 . PCC occurs mainly in middle and working age, and women are predominant 4 , 5 , 6 , 7 . Cognitive deficits are more prominent in attention and processing speed, episodic memory and executive function and have been linked to structural and functional brain changes in neuroimaging studies 8 , 9 , 10 , 11 , 12 , 13 . A longitudinal study showed greater reductions in cortical thickness and brain volumes in patients after COVID-19 than in healthy controls compared with neuroimaging acquired before the pandemic 14 . A recent study has also associated fatigue in PCC with structural imaging changes in the thalamus and basal ganglia 15 .
Similarly, most patients with Multiple Sclerosis (MS) also report fatigue and cognitive deficits. Cognitive deficits are especially focused on attention and processing speed impairment, followed by executive function and episodic memory. MS is a recognized autoimmune disorder, and cognitive deficits have been linked to cortical and subcortical structural and functional brain damage 16 , 17 .
Although the pathophysiology of PCC and the neurological symptoms of PCC is still unknown, several studies suggest mechanisms of neuroinflammation, autoimmune disorders, myelin dysregulation, and reactivation of another virus (such as Epstein-Barr infection) 18 , 19 . Although in a different clinical course and extent, these mechanisms are at least partially shared with MS. Besides, the role of Epstein-Barr virus or other viral infections in the development of MS and/or disease activity is supported by some studies 20 . Overall, this suggests an interest in evaluating the similarities and differences in the cognitive profiles of patients with PCC and MS. Comparative studies may also be useful to contextualize the cognitive deficits found in PCC, which have important socioeconomic consequences 21 . However, to our knowledge, there are no studies comparing cognitive dysfunction associated with PCC and MS. In addition, the relationship between fatigue and cognitive performance is still unclear. Previous studies in MS have found that cognitive tests assessing vigilance and alertness are more related to fatigue, which could be caused by shared mechanisms associated with brain atrophy and neurochemical dysfunction 22 . In PCC, fatigue has also correlated with some attentional tests 23 , 24 . Thus, this study aimed to compare the cognitive phenotypes of two large cohorts of patients with PCC and MS that were examined with the same neuropsychological protocol. We also aimed to evaluate the relationships between fatigue, and cognitive performance in the two cohorts. We also compared the frequency of depression, which is a relevant factor in both MS and PCC 25 , 26 , 27 .
Study design and participants
We conducted a cross-sectional investigation including patients with PCC and MS involved in previous research studies evaluating the cognitive characteristics of these disorders 28 , 29 . Patients were recruited from specific clinical programs dedicated to diagnosing and treating individuals with PCS and MS, where comprehensive neuropsychological assessment were integrated into the clinical protocol. The research protocol was approved by the Ethics Committee of our center (Comité de Ética de la Investigación con Medicamentos del Hospital Clínico San Carlos). Written informed consent was obtained from all participants.
Patients with PCC met the following criteria: (a) Diagnosis of COVID-19 confirmed by RT-PCR; (b) cognitive complaints or fatigue in close relationship with SARS-CoV-2 infection; (c) WHO criteria for Post-COVID-19 condition 1 . Exclusion criteria were as follows: (a) any cognitive complaint before COVID-19; (b) any medical, systemic, neurological or developmental comorbidity potentially linked to cognitive dysfunction; (c) history of alcohol or drug abuse; (d) neuropsychiatric disorders not attributable to PCC; (e) any sensory or motor disorder potentially biasing assessments.
Patients with MS met the following criteria: (a) diagnosis of MS according to the 2010 McDonald criteria 30 ; (2) age between 18 and 80 years. Exclusion criteria were as follows: (a) a relapse within the previous two months or active treatment with corticosteroids; (b) any other medical, systemic, neurological or developmental comorbidity potentially causing cognitive impairment; (c) history of alcohol or drug abuse; (d) neuropsychiatric disorders not attributable to MS; (e) sensory or motor disorder biasing assessments.
From an initial sample of 240 patients with PCC (mean age 48.42 ± 10.84 years, 77.9% of women, mean time since the acute infection of 17.48 ± 8.43 months), and 298 patients with MS (mean age 48.09 ± 9.84 years, 69.8% of women, mean duration of disease of 15.87 ± 7.85 years), a matched sample of 436 participants (218 per group) was obtained. The main clinical and demographic characteristics of each group and the vaccination status are presented in Table 1 . Time of SARS-CoV-2 infection (month and year) leading to PCC and time of assessments is shown in Supplementary Fig. 1 .
Neuropsychological and behavioral assessments
Patients were evaluated with a comprehensive neuropsychological protocol that is mainly based on the cognitive tests included in the Neuronorma battery. This was a set of neuropsychological tests co-normed in our country in older and young people 31 , 32 and has been validated in several diseases 33 . Previous works by our group implemented this battery to describe the cognitive profile in patients with MS and recently in PCC 28 , 29 . This battery was administered by trained neuropsychologists. The following tests were shared in the assessment of patients with PCC and MS and were included in the present study: forward and backward digit span, Corsi block-tapping test, Symbol Digit Modalities Test, Boston Naming Test (BNT), Judgment Line Orientation (JLO), Rey-Osterrieth Complex Figure (ROCF) (copy and recall at 3, 30 min, and recognition), Free and Cued Selective Reminding Test (FCSRT) (total free recall, total recall, delayed free recall, and delayed total recall), verbal fluencies (animals and words beginning with “ p ” and “m” in 1 min each one), Stroop Color-Word Interference Test.
Furthermore, patients were evaluated with the Modified Fatigue Impact Scale (MFIS) 34 . MFIS contains 21 items related to cognitive, physical, and psychosocial dimensions of fatigue, which are scored using a Likert-type scale. The assessment evaluates the impact of fatigue in the past 4 weeks. Additionally, depression was assessed with the Beck Depression Inventory-II 32 . Following previous literature, we used a cut-off of ≥ 38 to delineate fatigue and ≥ 19 to define moderate to severe depression 34 , 35 .
Statistical analysis
Statistical analysis was conducted using IBM(R) SPSS v26.0, JASP v0.16.1 and R software 36 . Figures were prepared using the ggplot2 package (v3.4.1). Using MedCalc 20.218, patients with MS and PCC were matched 1:1 according to sex, age (± 3 years), and years of education (± 3 years). The two independent samples t-test was used to compare the two groups. Effect sizes were estimated with Cohen’s d, and were classified as small (d = 0.2–0.49), moderate (d = 0.5–0.79), and large (d ≥ 0.8).
We calculated the percentage of impairment of each test according to the normative data correcting by age, years of education, and sex when needed. Normative data are based on a multicenter study conducted in Spain before the pandemic 31 , 32 . In addition, we used the criteria proposed by IC-CoDiMS and IC-CoDi-COVID groups to describe the cognitive phenotypes in patients with MS and PCC, respectively 37 , 38 . In this taxonomy, initially developed for epilepsy as IC-CoDE 39 , 40 , a domain is considered impaired when two tests within the same domain fall below the cutoff. For this study, we used -1 S.D as the cutoff to define impairment, according to the findings of the previous studies in both MS and PCC using these criteria 37 , 38 . Five cognitive domains are considered: attention/processing speed, executive function, language, visuospatial, and episodic memory. Then, according to the number of domains impaired, the patients are classified as: cognitively intact, single-domain impairment, bi-domain impairment, or multi-domain impairment (≥ 3 impaired domains). The tests specified in Table 2 were used to describe each cognitive domain. The chi-squared test was used to compare cognitive phenotypes between MS and PCC.
Pearson’s coefficient was used to estimate the correlations between fatigue and neuropsychological tests in PCC and MS. Coefficients < 0.40 were interpreted as a weak correlation, 0.40–0.69 as moderate, and > 0.69 as strong. Fisher r-to-z transformation was calculated to compare between correlation coefficients.
A p -value < 0.05 was considered statistically significant. Due to the number of cognitive tests in the neuropsychological protocol, we also specified those contrasts statistically significant after False-Discovery Rate (FDR) correction in the comparison of cognitive performance between PCC and MS.
Ethical approval
This study was approved by the Ethics and Research Committee from our centre and was performed according to the Declaration of Helsinki and its later amendments.
Comparison between PCC and MS
Patients with MS showed lower raw scores compared to PCC in Corsi forward and backwards, FCSRT (total free recall), ROCF memory at 3 and 30 min, and semantic verbal fluency. Conversely, PCC showed greater fatigue severity measured with MFIS. There were no statistically significant differences in the other neuropsychological tests and depressive symptoms. Effect size was moderate for fatigue, and low for the other significant neuropsychological tests. All results are shown in Table 3 .
Cognitive phenotypes
There were no statistically significant differences in the cognitive phenotypes (χ 2 3.014, p = 0.389). Specifically, 127 (58.25%) of PCC patients were regarded as cognitively intact, and 91 (41.74%) as cognitively impaired, 43 (19.72%) showed single-domain, 27 (12.38%) bi-domain, and 21 (9.63%) generalized impairment. Patients with MS were classified as cognitively intact in 112 cases (51.37%), and cognitively impaired in 106 (48.62%). Of those with impairment, 44 (20.18%) showed single-domain, 38 (17.43%) bi-domain, and 24 (11.00%) generalized impairment (Fig. 1 ).

Circle chart representing the cognitive phenotypes in PCC and MS.
Regarding the specific cognitive domains, 63 (28.89%) of PCC and 81 (37.15%) of MS showed impairment in attention/processing speed (χ 2 = 3.36, p = 0.067); 24 (11.00%) and 37 (16.97%) in episodic memory (χ 2 = 3.22, p = 0.073); 41 (18.8%) and 46 (21.10%) in executive function (χ 2 = 0.359, p = 0.549); 14 (6.42%) and 16 (7.33%) in visuospatial function (χ 2 = 0.143, p = 0.705); and 22 (10.09%) and 26 (11.92%) in language (χ 2 = 0.375, p = 0.541). The frequency of impairment of each individual test is shown in Supplementary Fig. 2 . Patients with MS showed higher frequency of impairment in Stroop trial 1 (χ 2 = 6.29, p = 0.012), semantic fluency (χ 2 = 9.86, p = 0.002), letter fluency (χ 2 = 9.42, p = 0.002), ROCF at 3 and 30 min (χ 2 = 6.12, p = 0.013 and χ 2 = 13.28, p < 0.001, respectively), and FCSRT total free recall (χ 2 = 7.20, p = 0.007). The other tests, including SDMT, showed no statistically significant differences ( p > 0.05).
Comparison of cognitive profiles within the groups with cognitive impairment
We also compared those patients meeting the criteria for cognitive impairment with PCC and MS. Patients with MS showed lower scores in ROCF memory at 3 min and 30 min and semantic fluency in age- and education-adjusted scaled scores (Supplementary Table 1 ). Patients with PCC showed greater severity of fatigue (59.95 ± 14.98 vs 54.47 ± 20.89, t = 2.13, p = 0.034). As depicted in Fig. 2 , the represented cognitive profile showed a more prominent impairment in those tests associated with attention and information processing speed.

Violin plots representing the adjusted scaled scores (mean 10, standard deviation 3) in each cognitive test in patients with PCC (green) and MS (red) classified as cognitively impaired. The dots represent the mean of each group. DSF digit span forward, DSB digit span backward, CF Corsi forward, CB Corsi backward, SDMT symbol digit modalities test, FCSRT (free and cued selective reminding test, fr1 free recall 1, tfr total free recall, tr total recall, dfr delayed free recall, dtr delayed total recall, ROCF3 Rey-Osterrieth complex figure (memory at 3 min), ROCF30 Rey-Osterrieth complex figure (memory at 30 min), ROCFr Rey-Osterrieth complex figure (memory recognition), ROCFc Rey-Osterrieth complex figure (copy accuracy), ROCFct Rey-Osterrieth complex figure (copy time), JLO judgment line orientation, BNT Boston naming test, SF semantic fluency (animals), LF letter fluency (words beginning with “ p ”).
Correlations between fatigue and neuropsychological tests
All correlations are shown in Fig. 3 . In PCC, MFIS (total score) showed weak correlations with SDMT, FCSRT (total free recall and total recall), Stroop (parts 1, 2, and 3) and semantic and letter fluency. In MS, MFIS (total score) showed moderate correlations with SDMT, FCSRT (free delayed recall and total delayed recall), Stroop test (parts 1 and 2); and weak correlations were found with almost all the other tests.

Heatmap showing correlations between MFIS (total score) and neuropsychological tests scores in PCC and MS. The size and direction of the correlation are shown in the right vertical label. DSF digit span forward, DSB digit span backward, CF Corsi forward, CB Corsi backward, SDMT symbol digit modalities test, FCSRT (free and cued selective reminding test), fr1 free recall 1, tfr total free recall, tr total recall, dfr delayed free recall, dtr delayed total recall, ROCF3 Rey-Osterrieth complex figure (memory at 3 min), ROCF30 Rey-Osterrieth complex figure (memory at 30 min), ROCFr Rey-Osterrieth complex figure (memory recognition), ROCFc Rey-Osterrieth complex figure (copy accuracy), ROCFct Rey-Osterrieth complex figure (copy time), JLO judgment line orientation, BNT Boston naming test, SF semantic fluency (animals), LF letter fluency (words beginning with “ p ”).
Patients with MS showed higher correlations than PCC in the following tests: digit span forward (z = 3.02, p = 0.002), digit span backward (r = 3.53, p < 0.001), Corsi forward (Z = 2.45, p = 0.014), SDMT (z = 2.82, p = 0.004), Boston Naming Test (z = 2.81, p = 0.005), FCSRT recall trial 1 (Z = 2.15, p = 0.015), FCSRT total free recall (Z = 2.38, p = 0.017), FCSRT total recall (z = 3.63, p < 0.001), FCSRT delayed free recall (Z = 4.94, p < 0.001), FCSRT delayed total recall (Z = 3.93, p < 0.001), ROCF (memory at 3 min) (Z = 2.26, p = 0.011), ROCF (memory at 30 min) (z = 2.1, p = 0.035), semantic fluency (Z = 2.03, p = 0.04), letter fluency (M-words) (z = 2.64, p = 0.008), letter fluency (R-words) (z = 3.02, p = 0.002), Judgment Line Orientation (Z = 3.26, p = 0.001). There were no statistically significant differences ( p > 0.05) in the comparison of correlation coefficients in Stroop (trials 1, 2, and 3), Corsi backward, ROCF (copy accuracy and time), ROCF (memory recognition), and letter fluency ( P -words).
In this study, we examined the existence of differences in cognitive characteristics between PCC and MS, and the relationship between cognitive function and fatigue. We used two large cohorts of patients that were evaluated with a common neuropsychological protocol. Our study found a significant overlap in cognitive profile between both diseases. Importantly, attention and processing speed were the most pronounced deficits in both disorders, which is consistent with previous studies 2 , 37 , 41 , 42 . Few differences were found in episodic memory tests, which were more impaired in the group of patients with MS than PCC. Similarly, semantic fluency was also more impaired, which could also be linked to the greater impairment of episodic memory 43 . However, effect sizes for these tests were small, confirming that MS and PCC present a very similar cognitive profile.
We applied a novel approach using an international classification of cognitive disorders that is being implemented across several disease groups 37 , 38 , 40 , 44 . This classification system is based on a five-domain cognitive model (attention/processing speed, executive function, episodic memory, visuospatial function, and language) and provides a working definition of impairment to identify cognitive phenotypes and improve cognitive diagnostics. This taxonomy has found reproducible findings across several independent cohorts examined with different neuropsychological batteries in epilepsy 40 , multiple sclerosis 37 and PCC 38 . It has also shown favorable cross-cultural properties in diverse settings 36 . Our study also supports the use of this taxonomy as a valid method for comparative research across disorders.
By comparing both disorders, the similarities in the cognitive characteristics and the severity of deficits contribute to contextualizing the cognitive dysfunction in PCC. In this regard, our findings suggest that cognitive deficits in PCC are almost as pronounced and prevalent as in MS, and fatigue is even more severe, supporting the mounting evidence that fatigue and cognitive dysfunction are associated with occupational issues and socioeconomic consequences 45 , 46 .
The severity and frequency of fatigue was greater in patients with PCC. Interestingly, correlations between MFIS total score (evaluating fatigue impact in the last 4 weeks) and neuropsychological tests were larger in the case of MS. However, the cognitive tests that showed stronger correlations with MFIS were similar in both disorders (e.g., Stroop). This may suggest common mechanisms and neural underpinnings in fatigue and cognitive dysfunction in both disorders, as has been recently described 9 . This opens the way to test new therapies for fatigue based on their association with functional brain changes, such as non-invasive brain stimulation, which have shown positive effects in two clinical trials 47 , 48 . However, at the same time, the lower correlation with neuropsychological tests and the greater severity of fatigue in PCC suggest the existence of other mechanisms (probably not dependent on the central nervous system and including systemic processes such as immune mechanisms, mitochondrial dysfunction or muscle abnormalities) involved in the pathophysiology of fatigue in PCC 24 , 49 , 50 . In contrast, fatigue in MS would be more dependent on central mechanisms.
Another interesting result is the lack of significant differences in the severity and frequency of depressive symptoms. Although neuropsychiatric symptoms have been especially emphasized in PCC, most studies did not include a control group 51 . The prevalence of depression is higher in MS than in the general population, and has been associated with several factors, including genetic and immunological factors, brain changes, and psychosocial factors 52 . Similarly, in PCC, proinflammatory factors and psychosocial factors have been hypothesized, but clear evidence about the pathophysiology of depression is still lacking.
Our study has some limitations. First, although the protocol includes several tests of the main cognitive domains, we acknowledge the possibility of differences between groups if other specific tests are used. In this regard, a more thorough analysis of attention and executive function subdomains may be of interest to further characterize the cognitive mechanisms impaired in each disorder. In this study, we selected only those tests shared by both cohorts to avoid potential differences in the frequency of impairment to the length of the battery or the number of neuropsychological tests and scores. Second, fatigue was only assessed with MFIS, which mainly evaluates the impact of fatigue in daily living. More comprehensive questionnaires may be of interest to evaluate potential differences in the clinical characteristics of fatigue across disorders. Additionally, it could also be of interest to evaluate the feeling of fatigue on the same day of the examination because MFIS considers the fatigue severity in the 4 weeks before the assessment. Third, our study is performed in a single center. However, demographic characteristics and degree of impairment in both PCC and MS are consistent with previous studies of the literature, suggesting that both cohorts are representative of these disorders. In this regard, the most important proportion were infected during the first waves (especially the first in March 2020) and before vaccines were available. Furthermore, we must acknowledge the possibility of selection bias, particularly concerning MS, where individuals with more pronounced motor and cognitive impairments may be less inclined to undergo extensive neuropsychological evaluations. Nevertheless, our study was conducted within a framework where comprehensive neuropsychological assessments are standard practice for both MS and PCS. Additionally, the demographic characteristics of our participants closely resemble those of other large-scale studies published in the field 53 , 54 .
In conclusion, our study finds similar cognitive profiles in PCC and MS, which are mainly characterized by attention and processing speed deficits. Fatigue was more severe in PCC, but the relationship between fatigue and cognitive function was greater in the case of MS. Further comparative studies addressing the mechanisms associated with cognitive dysfunction and fatigue may be of interest to advance the knowledge of these disorders and develop new therapies.
Data availability
The datasets generated and analyzed are available from the corresponding author on reasonable request.
Soriano, J. B., Murthy, S., Marshall, J. C., Relan, P. & Diaz, J. V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 22 , e102–e107 (2022).
Article CAS PubMed Google Scholar
Bertuccelli, M. et al. Cognitive impairment in people with previous COVID-19 infection: A scoping review. Cortex 154 , 212–230 (2022).
Article PubMed PubMed Central Google Scholar
Ceban, F. et al. Brain behavior and immunity fatigue and cognitive impairment in Post-COVID-19 syndrome: A systematic review and meta-analysis. Brain Behav. Immun. 101 , 93–135 (2022).
Article ADS CAS PubMed Google Scholar
Crook, H., Raza, S., Nowell, J., Young, M. & Edison, P. Long covid—mechanisms, risk factors, and management. BMJ 374 , 1–18 (2021).
Google Scholar
Peter, R. S. et al. Post-acute sequelae of covid-19 six to 12 months after infection: Population based study. BMJ 379 , e071050 (2022).
Article PubMed Google Scholar
Bai, F. et al. Female gender is associated with long COVID syndrome: A prospective cohort study. Clin. Microbiol. Infect. 28 , 611 (2022).
Article Google Scholar
Bahmer, T. et al. Severity, predictors and clinical correlates of Post-COVID syndrome (PCS) in Germany: A prospective, multi-centre, population-based cohort study. EClinicalMedicine 51 , 101549 (2022).
Caroli, A. et al. Brain diffusion alterations in patients with COVID-19 pathology and neurological manifestations. NeuroImage Clin. 37 , 103338 (2023).
Díez-Cirarda, M. et al. Multimodal neuroimaging in post-COVID syndrome and correlation with cognition. Brain 146 , 2142–2152 (2023).
Lu, Y. et al. Cerebral micro-structural changes in COVID-19 patients–an MRI-based 3-month follow-up study. EClinicalMedicine 25 , 100484 (2020).
Ajcevic, M. et al. Cerebral hypoperfusion in post-COVID-19 cognitively impaired subjects revealed by arterial spin labeling MRI. Sci. Rep. 13 , 5808 (2023).
Article ADS CAS PubMed PubMed Central Google Scholar
Paolini, M. et al. Brain correlates of subjective cognitive complaints in COVID-19 survivors: A multimodal magnetic resonance imaging study. Eur. Neuropsychopharmacol. 68 , 1–10 (2023).
Zhao, S., Toniolo, S., Hampshire, A. & Husain, M. Effects of COVID-19 on cognition and brain health. Trends Cognit. Sci. 27 , 1053–1067 (2023).
Douaud, G. et al. SARS-CoV-2 is associated with changes in brain structure in UK Biobank. Nature https://doi.org/10.1038/s41586-022-04569-5 (2022).
Heine, J. et al. Articles structural brain changes in patients with post-COVID fatigue: A prospective observational study. eClinicalMedicine 58 , 101874 (2023).
Matías-Guiu, J. A. et al. Identification of cortical and subcortical correlates of cognitive performance in multiple sclerosis using voxel-based morphometry. Front. Neurol. 9 , 1–12 (2018).
Petracca, M. et al. Neuroimaging correlates of cognitive dysfunction in adults with multiple sclerosis. Brain Sci. 11 , 346 (2021).
Article CAS PubMed PubMed Central Google Scholar
Fernández-Castañeda, A. et al. Mild respiratory SARS-CoV-2 infection can cause multi-lineage cellular dysregulation and myelin loss in the brain. BioRxiv (2022).
Gold, J. E., Okyay, R. A., Licht, W. E. & Hurley, D. J. Investigation of long covid prevalence and its relationship to epstein-barr virus reactivation. Pathogens 10 , 1–15 (2021).
Aloisi, F., Giovannoni, G. & Salvetti, M. Epstein–Barr virus as a cause of multiple sclerosis: Opportunities for prevention and therapy. Lancet. Neurol. 22 , 338–349 (2023).
Perlis, R. H. et al. Association of Post-COVID-19 condition symptoms and employment status. JAMA Netw. Open 6 , e2256152 (2023).
Hanken, K., Eling, P. & Hildebrandt, H. Is there a cognitive signature for MS-related fatigue?. Multiple Scler. 21 , 376–381 (2015).
Calabria, M. et al. Post-COVID-19 fatigue: The contribution of cognitive and neuropsychiatric symptoms. J. Neurol. 269 , 3990–3999 (2022).
Matias-Guiu, J. A. et al. Neuropsychological predictors of fatigue in Post-COVID syndrome. J. Clin. Med. 11 , 1–13 (2022).
Leavitt, V. M. et al. Dissociable cognitive patterns related to depression and anxiety in multiple sclerosis. Multiple Scler 26 , 1247–1255 (2020).
Article CAS Google Scholar
Premraj, L. et al. Mid and long-term neurological and neuropsychiatric manifestations of post-COVID syndrome: A meta-analysis. J. Neurol. Sci. 434 , 120162 (2022).
Delgado-Alonso, C. et al. Unraveling brain fog in post-COVID syndrome: Relationship between subjective cognitive complaints and cognitive function, fatigue, and neuropsychiatric symptoms. Eur. J. Neurol. https://doi.org/10.1111/ene.16084 (2023).
Delgado-Alonso, C. et al. Cognitive dysfunction associated with COVID-19: A comprehensive neuropsychological study. J. Psychiatr. Res. 150 , 40–46 (2022).
Matías-Guiu, J. A. et al. Validation of the Neuronorma battery for neuropsychological assessment in multiple sclerosis. Multiple Scler. Relat. Disord. 42 , 102070 (2020).
Polman, C. H. et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol. 69 , 292–302 (2011).
Peña-Casanova, J. et al. Spanish multicenter normative studies (NEURONORMA project): Methods and sample characteristics. Arch. Clin. Neuropsychol. 24 , 307–319 (2009).
Peña-Casanova, J. et al. Estudios normativos españoles en población adulta joven (Proyecto NEURONORMA jóvenes): Métodos y características de la muestra. Neurologia 27 , 253–260 (2012).
Sánchez-Benavides, G. et al. Cognitive and neuroimaging profiles in mild cognitive impairment and Alzheimer’s disease: Data from the Spanish Multicenter Normative Studies (NEURONORMA Project). J. Alzheimer’s Dis. 41 , 887–901 (2014).
Kos, D. et al. Evaluation of the modified fatigue impact scale in four different European countries. Multiple Scler. 11 , 76–80 (2005).
Beck, A. T. Manual for the beck depression inventory-II. (No Title) (1996).
R Core Team. R: A Language and Environment for Statistical Computing. (2022).
Hancock, L. M. et al. A proposed new taxonomy of cognitive phenotypes in multiple sclerosis: The International Classification of Cognitive Disorders in MS (IC-CoDiMS). Multiple Scler. J. 29 , 615–627 (2022).
Matias-Guiu, J. A. et al. Development of criteria for cognitive dysfunction in post-COVID syndrome: The IC-CoDi-COVID approach. Psychiatry Res. 319 , 115006 (2023).
Norman, M. et al. Addressing neuropsychological diagnostics in adults with epilepsy: Introducing the International Classification of Cognitive Disorders in Epilepsy: The IC CODE Initiative. Epilepsia Open 6 , 266–275 (2021).
McDonald, C. R. et al. Development and application of the International Classification of Cognitive Disorders in Epilepsy (IC-CoDE): Initial results from a multi-center study of adults with temporal lobe epilepsy. Neuropsychology 37 , 301–314 (2022).
Gonzalez-Fernandez, E. & Huang, J. Cognitive aspects of COVID-19. Curr. Neurol. Neurosci. Rep. 23 , 531–538 (2023).
Benedict, R. H. B., Amato, M. P., DeLuca, J. & Geurts, J. J. G. Cognitive impairment in multiple sclerosis: Clinical management, MRI, and therapeutic avenues. Lancet Neurol 19 , 860–871 (2020).
Delgado-Álvarez, A. et al. Cognitive processes underlying verbal fluency in multiple sclerosis. Front. Neurol. 11 , 1–11 (2021).
Reyes, A. et al. Establishing the cross-cultural applicability of a harmonized approach to cognitive diagnostics in epilepsy: Initial results of the International Classification of Cognitive Disorders in Epilepsy in a Spanish-speaking sample. Epilepsia 64 , 728–741 (2023).
Delgado-Alonso, C. et al. Fatigue and cognitive dysfunction are associated with occupational status in post-COVID syndrome. Int. J. Environ. Res. Public Health 19 , 13368 (2022).
Moccia, M. et al. Determinants of early working impairments in multiple sclerosis. Front. Neurol. 13 , 1062847 (2022).
Oliver-Mas, S. et al. Transcranial direct current stimulation for post-COVID fatigue: A randomized, double-blind, controlled pilot study. Brain Commun. https://doi.org/10.1093/braincomms/fcad117 (2023).
Santana, K. et al. Non-invasive brain stimulation for fatigue in post-acute sequelae of SARS-CoV-2 (PASC). Brain Stimul. 16 , 100–107 (2023).
Paul, B. D., Lemle, M. D., Komaroff, A. L. & Snyder, S. H. Redox imbalance links COVID-19 and myalgic encephalomyelitis/chronic fatigue syndrome. Proc. Natl. Acad. Sci. 118 , e2024358118 (2021).
Ramakrishnan, R. K., Kashour, T., Hamid, Q., Halwani, R. & Tleyjeh, I. M. Unraveling the mystery surrounding post-acute sequelae of COVID-19. Front. Immunol. 12 , 686029 (2021).
Renaud-Charest, O. et al. Onset and frequency of depression in post-COVID-19 syndrome: A systematic review. J. Psychiatr. Res. 144 , 129–137 (2021).
Solaro, C., Gamberini, G. & Masuccio, F. G. Depression in multiple sclerosis: Epidemiology, aetiology, diagnosis and treatment. CNS Drugs 32 , 117–133 (2018).
Strober, L. et al. Symbol digit modalities test: A valid clinical trial endpoint for measuring cognition in multiple sclerosis. Multiple Scler 25 , 1781–1790 (2019).
Crivelli, L. et al. Changes in cognitive functioning after COVID-19: A systematic review and meta-analysis. Alzheimers Dement. 18 , 1047–1066 (2022).
Download references
Acknowledgements
The authors acknowledge all the participants in this study, and specifically the association of patients with long-COVID “Asociación Madrileña de Covid Persistente (AMACOP)” for their support.
This research has received funding from the Nominative Grant FIBHCSC 2020 COVID-19 (Department of Health, Community of Madrid) and Fundación para el Conocimiento Madri + d (Healthstart plus program, Community of Madrid, REACT-EU funds) through project G63-HEALTHSTARPLUS-HSP4. Jordi A Matias-Guiu is supported by Instituto de Salud Carlos III through the project INT20/00079 and INT23/00017 (co-funded by European Regional Development Fund “A way to make Europe”). María Valles-Salgado is supported by the Instituto de Salud Carlos III through a predoctoral contract (FI20/000145) (co-funded by European Regional Development Fund “A way to make Europe”). Maria Diez-Cirarda is funded by a Sara Borrell postdoctoral fellowship from the Instituto de Salud Carlos III (CD22/00043) (co-funded by European Regional Development Fund “A way to make Europe”). Silvia Mas-Oliver is supported by Fundación para el Conocimiento madri + d through project G63-HEALTHSTARPLUS-HSP4.
Author information
Authors and affiliations.
Department of Neurology, Hospital Clínico San Carlos, Instituto de Investigacion Sanitaria “San Carlos” (IdISSC), C/Profesor Martín Lagos, 28040, Madrid, Spain
Cristina Delgado-Alonso, Alfonso Delgado-Alvarez, María Díez-Cirarda, Silvia Oliver-Mas, Constanza Cuevas, Paloma Montero-Escribano, María José Gil-Moreno, Juan Ignacio López-Carbonero, Jorge Matias-Guiu & Jordi A. Matias-Guiu
Department of Endocrinology, Hospital Clínico San Carlos, Instituto de Investigacion Sanitaria “San Carlos” (IdISSC), Madrid, Spain
Ana Maria Ramos-Leví
Department of Neurology, School of Medicine and Public Health, University of Wisconsin, Madison, WI, USA
Bruce P. Hermann
You can also search for this author in PubMed Google Scholar
Contributions
Conceptualization: C.D.A., J.M.G., J.A.M.G. Methodology: C.D.A., M.D.C., B.P.H., J.A.M.G. Data curation: all. Investigation: all. Formal analysis: C.D.A., A.M.R.L., J.A.M.G. Project administration: J.M.G., J.A.M.G. Writing original draft: C.D.A., J.A.M.G. Writing – review & editing: A.D.A., M.D.C., J.M.G., B.P.H.
Corresponding author
Correspondence to Jordi A. Matias-Guiu .
Ethics declarations
Competing interests.
The authors declare no competing interests.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary legends., supplementary table 1., supplementary figure 1., supplementary figure 2., rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Cite this article.
Delgado-Alonso, C., Delgado-Alvarez, A., Díez-Cirarda, M. et al. Cognitive profile in multiple sclerosis and post-COVID condition: a comparative study using a unified taxonomy. Sci Rep 14 , 9806 (2024). https://doi.org/10.1038/s41598-024-60368-0
Download citation
Received : 29 June 2023
Accepted : 22 April 2024
Published : 29 April 2024
DOI : https://doi.org/10.1038/s41598-024-60368-0
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
By submitting a comment you agree to abide by our Terms and Community Guidelines . If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.

- Open access
- Published: 26 April 2024
Choroidal manifestations of non-ocular sarcoidosis: an enhanced depth imaging OCT study
- Ye Eun Han ORCID: orcid.org/0000-0002-0726-0193 1 ,
- Jaehyuck Jo ORCID: orcid.org/0009-0002-2419-9416 1 ,
- Ho Cheol Kim ORCID: orcid.org/0000-0002-3154-4858 2 &
- Junyeop Lee ORCID: orcid.org/0000-0001-5887-8033 1 , 3
BMC Ophthalmology volume 24 , Article number: 199 ( 2024 ) Cite this article
55 Accesses
1 Altmetric
Metrics details
Although choroidal thickening was reported as a sign of active inflammation in ocular sarcoidosis, there has been no research on the choroidal changes in non-ocular sarcoidosis (defined as systemic sarcoidosis without overt clinical signs of ocular involvement). Therefore, this study aimed to investigate choroidal structural changes in patients with non-ocular sarcoidosis.
This retrospective case–control study was conducted at Asan Medical Center, a tertiary referral center. We evaluated 30 eyes with non-ocular sarcoidosis and their age- and spherical equivalent-matched healthy control eyes. The subfoveal choroidal thickness, area ratio (Sattler layer-choriocapillaris complex [SLCC] area to Haller layer [HL] area), and choroidal vascularity index (CVI, luminal area to choroidal area) were analyzed using enhanced depth imaging in optical coherence tomography. Systemic and ocular factors associated with the choroidal thickness were investigated.
Compared with the healthy control group, the non-ocular sarcoidosis group had significantly thicker subfoveal choroid (total and all sublayers [SLCC and HL]) and lower area ratio. There were no significant differences in the CVIs at all sublayers between groups. In the non-ocular sarcoidosis group, eyes under oral steroid treatment had thinner choroid than eyes under observation. In the control group, eyes with older age and more myopic spherical equivalent had thinner choroidal thickness.
Total and all sublayers of the subfoveal choroid were significantly thicker without significant vascularity changes in non-ocular sarcoidosis eyes than in healthy control eyes. The degree of choroidal thickening was disproportionally greater at HL than at SLCC. These characteristic choroidal changes may be the subclinical manifestations in non-ocular sarcoidosis.
Peer Review reports
Sarcoidosis is a chronic multisystem disorder of unknown origin defined by non-caseating granulomas with the accumulation of T-lymphocytes [ 1 ]. Although the most commonly affected organs are the lungs and intrathoracic lymph nodes, almost any organ can be affected [ 2 ]. Ocular involvement is the second most common extrathoracic manifestation in 25–60% of patients with systemic sarcoidosis [ 2 , 3 ]. Ocular sarcoidosis can also involve any part of the eye and its adnexal tissue [ 2 , 3 ]. The most common ocular manifestation is uveitis, followed by conjunctival nodules [ 2 , 3 ]. Reportedly, approximately 25% of the patients initially diagnosed with pulmonary sarcoidosis were found to have bilateral uveitis [ 4 ]. The typical types of uveitis associated with sarcoidosis are granulomatous and bilateral; it can be anterior-, intermediate-, posterior-, and pan-uveitis [ 5 ]. Posterior uveitis involving the retina and/ or choroid accounts for 5–28% of ocular sarcoidosis [ 5 ].
Previous studies have shown that sarcoidosis-related uveitis results in changes in choroidal thickness in addition to retinal abnormalities using enhanced depth imaging in spectral-domain optical coherence tomography (EDI SD-OCT) [ 6 , 7 ]. Interestingly, changes in choroidal thickness were also found even in eyes without overt intraocular inflammation in patients with Behçet's disease, another multiorgan-involving inflammatory disease [ 8 ]. It suggests systemic inflammatory diseases may have subclinical manifestations in the choroid without apparent clinical signs of intraocular involvement. However, to our knowledge, there has been no research regarding choroidal changes in eyes with systemic sarcoidosis without overt clinical signs of ocular involvement (defined as non-ocular sarcoidosis). This study aimed to investigate choroidal structural changes in non-ocular sarcoidosis using EDI SD-OCT.
This retrospective observational case–control study was conducted at Asan Medical Center, a tertiary referral center in Seoul, South Korea. We retrospectively reviewed the medical records of all patients referred for ophthalmic examination under the diagnosis of systemic sarcoidosis from March 2020 to July 2021. Among them, eyes without ophthalmological signs for ocular involvement based on the International Workshop on Ocular Sarcoidosis criteria [ 9 ] were included. To thoroughly exclude intraocular inflammation in sarcoidosis, which may only be detectable through angiogenic evaluation [ 4 ], we additionally assessed wide-field fluorescein angiography [wFA] and indocyanine green angiography [wICGA]. After that, their age- and spherical equivalent (SE)-matched healthy controls were selected among those who visited our clinic for retinal screening. The OCT image acquisition times were also matched within a 2-h difference to minimize the confounding effect of the diurnal variation of choroidal thickness [ 10 ]. Eyes with any history of ocular surgery (including refractive or cataract surgery to make SE reflect axial length), incomplete ocular evaluations required for this study, and other ocular or systemic diseases (except sarcoidosis) that possibly cause intraocular complications were excluded. If both eyes were qualified for the study, the right eye of each patient was included in the analysis.
Ocular and systemic evaluation
The ocular examinations were assessed by retinal specialists (Y.E.H, J. J. and J. L.), which included best-corrected visual acuity (BCVA), intraocular pressure by non-contact tonometry (Topcon CT-60, Topcon; Tokyo, Japan), SE from manifested refraction, slit-lamp biomicroscopy, funduscopic examination, and EDI SD-OCT (Heidelberg Engineering GmbH; Heidelberg, Germany), for both the sarcoidosis and control groups. Additionally, wFA and wICGA (HRA-2; Heidelberg Engineering, Heidelberg, Germany) were assessed for the sarcoidosis group. Diagnosis (based on biopsy and radiological findings) and treatment regimen of systemic sarcoidosis were determined by a pulmonologist (H.C.K.). Blood tests (including Angiotensin-converting enzyme [ACE] and C-reactive protein [CRP]) were conducted on the day of referral to the ophthalmologists. Disease duration was defined as the time gap from the preliminary diagnosis of systemic sarcoidosis to the first day of the ophthalmologic examinations.
SD-OCT acquisition and analysis
SD-OCT with enhanced depth imaging (EDI) protocols [ 11 ] obtained detailed and measurable images of the choroid. Among horizontal raster pattern scans (30° × 5°, 9.0 mm × 1.5 mm field), umbo-centered images were selected for the analysis. As shown in Fig. 1 , the choroid was defined as the space between the retinal pigment epithelium and choroidoscleral junction. The choroid was subdivided into Sattler layer-choriocapillaris complex (SLCC; < 100-μm sized small-to-medium vascular luminal spaces plus choriocapillaris) and Haller layer (HL; ≥ 100-μm sized large vascular luminal spaces) [ 12 , 13 , 14 ]. The subfoveal zone was defined as the 750-μm distance around the umbo. Using built-in software (Heidelberg Eye Explorer version 1.10.1.0; Heidelberg Engineering), the subfoveal choroidal thickness (the mean value of the perpendicular thickness at three points; the umbo and 750-μm intervals [right and left]) of the total and each sublayer was manually measured. Additionally, the area of each sublayer at the subfoveal zone was also measured by manual tracing, and their area ratio was calculated by dividing SLCC area by HL area, indicating SLCC occupying area percentage from HL.

Representative enhanced depth imaging in spectral domain optical coherence tomography of ( a ) healthy control eye and ( b ) non-ocular sarcoidosis eye
After importing SD-OCT images into ImageJ software (version 1.52, Wayne Rasband, National Institutes of Health; Bethesda, MD, USA), the choroidal vascularity index (CVI) was calculated to assess the vascularity status of each sublayer of the choroid (Fig. 2 ). First, the manually subdivided SLCC and HL were binarized using Niblack’s auto-local threshold. After that, the selection of dark pixels (representing the luminal area) by color threshold was performed, and CVI was calculated by dividing the luminal area by the total choroidal area [ 15 , 16 ]. All manual segmentation and measurements were carried out by two independent examiners (Y.E.H. and J.J.), and averaged data were used in the final analysis. The degree of inter-examiner agreement in each measurement was assessed by Interclass correlation coefficient (ICC) and shown by Bland–Altman plot.

Measurement of choroidal vascularity index in healthy control eye and non-ocular sarcoidosis eye. a Sattler layer-choriocapillaris complex and ( b ) Haller layer in healthy control eye and ( c ) Sattler layer-choriocapillaris complex and ( d ) Haller layer in eye with non-ocular sarcoidosis
Statistical analysis
Descriptive statistics were demonstrated in numbers and percentages for categorical variables and means ± standard deviations for continuous variables. A Student’s t-test and Chi-squared test were used to evaluate the demographic and ocular differences between the groups depending on the variable types. Univariate and multivariable linear regression analysis and Chi-squared test were used to estimate the relationship between choroidal thickness and the demographic and ocular factors depending on their variable types. We considered a p -value of less than 0.05 as statistically significant and less than 0.10 as borderline significant. All of the statistical analyses were performed using SPSS software (version 21.0, IBM Corp.; Armonk, NY, USA).
During the study period, we screened 71 systemic sarcoidosis patients, and of these, 19 patients (26.8%) were diagnosed with ocular sarcoidosis. Among 52 non-ocular sarcoidosis patients, 30 patients met the study eligibility criteria. Therefore, a total of 30 eyes of 30 non-ocular sarcoidosis patients and their age- and spherical equivalent-matched healthy controls were included in this study. The demographics and ocular characteristics are shown in Table 1 . The mean age of the patients with non-ocular sarcoidosis was 55.13 ± 11.58 years, with a male-to-female ratio of 11:19. The mean logMAR BCVA, SE, and intraocular pressure were 0.03 ± 0.05, -0.71 ± 1.93 diopters and 15.73 ± 2.40 mmHg, respectively. Twenty-seven patients (90%) were diagnosed with pulmonary sarcoidosis; three patients (10%) were extrapulmonary sarcoidosis (skin involvement [ n = 3, 10%]). During 16.10 ± 26.18 months of systemic sarcoidosis duration, eleven patients (36.66%) have received medical treatments (oral steroid, prednisolone 10-40 mg/day [ n = 6, 20.00%] and methotrexate 15 mg/day [ n = 5, 16.66%]), while others ( n = 19, 63.33%) were under observation. The mean referral-to-ophthalmologic screening duration was 33.38 ± 41.12 days. The healthy control group showed no significant difference in baseline demographic and ocular characteristics compared with the non-ocular sarcoidosis group.
Choroidal characteristics of are summarized in Table 2 . Total and all sublayers (SLCC and HL) were significantly thicker in the non-ocular sarcoidosis group than in the healthy control group (Total: 349.86 ± 62.28 μm vs. 272.13 ± 65.27 μm, p < 0.001; SLCC: 103.66 ± 20.28 μm vs. 88.73 ± 20.10 μm, p = 0.006; HL: 246.20 ± 54.85 μm vs. 183.40 ± 54.40 μm, p < 0.001). The area ratio was significantly lower in the non-ocular sarcoidosis group than the control group (0.43 ± 0.11 vs. 0.50 ± 0.13, p = 0.048), indicating the degree of choroidal thickening at HL was greater than SLCC in non-ocular sarcoidosis. There were no significant differences in CVIs of all sublayers between the two groups (SLCC: 67.97 ± 4.30% vs. 68.48 ± 3.67%, p = 0.626; HL: 60.03 ± 2.56% vs. 59.89 ± 3.64%, p = 0.862). Their distributions are displayed in Fig. 3 . The inter-examiner agreements were demonstrated to be good to excellent [ 17 ] in all measurements, as assessed by ICC (thickness of total choroid = 0.977 [95% confidence interval, CI = 0.692–0.986, p < 0.001], thickness of SLCC = 0.910 [95% CI = 0.850–0.946, p < 0.001], thickness of HL = 0.957 [95% CI = 0.929–0.975, p < 0.001], the area ratio = 0.839 [95% CI = 0.730–0.904, p < 0.001], CVI of SLCC = 0.980 [95% CI = 0.967–0.988, p < 0.001], and CVI of HL = 0.960 [95% CI = 0.932–0.976, p < 0.001]). The differences between measurements from two examiners were shown by Bland–Altman plots (Fig. 4 ).

Boxplots of choroidal parameters in healthy control eyes and with non-ocular sarcoidosis eyes. a total choroidal thickness (interquartile range [IQR] = 226–332 μm vs. 311–382 μm, median = 260 μm vs. 354 μm) ( b ) Sattler layer-choriocapillaris complex thickness (IQR = 72–104 μm vs. 90–120 μm, median = 84 μm vs. 106 μm), c Haller layer thickness (IQR = 154–237 μm vs. 219–283 μm, median = 169 μm vs. 244 μm), d choroidal area ratio (IQR = 0.42–0.56 vs. 0.32–0.53, median = 0.47 vs. 0.41), and choroidal vascular index (CVI) of ( e ) Sattler layer-choriocapillaris complex (IQR = 65.97–70.61% vs. 65.03–69.58%, median = 67.82% vs. 67.83%) and ( f ) Haller layer (IQR = 57.80–61.54% vs, 58.16–61.82%, median = 60.48% vs. 60.08%). (box = interquartile range, horizontal line = median, whiskers = 10 to 90 percentile, dots = outliers)

Bland–Altman plots of choroidal measurements in the entire study eyes. a total choroidal thickness, b Sattler layer-choriocapillaris complex thickness, c Haller layer thickness, d choroidal area ratio, and choroidal vascular index (CVI) of ( e ) Sattler layer-choriocapillaris complex and ( f ) Haller layer
In the healthy control group, older age showed a significant association with thinner total choroid ( r 2 = 0.200, p = 0.013), SLCC ( r 2 = 0.183, p = 0.018), and HL ( r 2 = 0.143, p = 0.039) in both univariate and multivariable analysis, whereas, more myopic SE showed its significance only in univariate analysis (total [ r 2 = 0.186, p = 0.017], SLCC [ r 2 = 0.178, p = 0.020], and HL [ r 2 = 0.130, p = 0.049]) (Table 3 ). In the non-ocular sarcoidosis group, eyes treated with oral steroids showed significantly thinner choroidal thickness than eyes under observation (total choroid: 305.83 μm vs. 360.87 μm, p = 0.015; SLCC: 90.33 μm vs. 107.00 μm, p = 0.073; and HL: 215.50 μm vs. 253.87 μm, p = 0.082) (Table 3 ). No other systemic or ocular factors were associated with choroidal thickness in both groups.
In this study, all sublayers of the subfoveal choroid were significantly thicker, especially HL, without vascularity changes in non-ocular sarcoidosis eyes compared with healthy control eyes. To the best of our knowledge, this is the first study to demonstrate subclinical structural alterations of the choroid using EDI SD-OCT in eyes with systemic sarcoidosis without overt ocular involvement.
With the advancement of OCT technology allowing in-vivo cross-sectional visualization of the entire choroid, changes in choroidal thickness in ocular sarcoidosis have been reported. Mehta et al. [ 7 ] demonstrated a disproportionately enlarged Sattler layer in sarcoidosis-related uveitis and choroidal thickening in active granulomatous uveitis. On the other hand, Güngör et al. [ 6 ] reported that patients with ocular sarcoidosis had a thinner subfoveal choroid during the quiescent phases than normal controls. The choroid is supposed to be highly reactive to inflammatory conditions due to its highly vascularized structure without the autoregulation of perfusion [ 18 ]. Pro-inflammatory cytokines, such as prostaglandins, are known to be upregulated and have central roles in systemic sarcoidosis [ 19 , 20 , 21 ]. It is speculated that inflammatory reaction of the choroidal vascular network to pro-inflammatory cytokines is the main mechanism of increasing choroidal thickness in intraocular inflammation associated with sarcoidosis [ 6 ]. However chronic choroidal inflammation ultimately leads to choroidal atrophy and thinning in the quiescent phase [ 7 ].
The thicknesses and CVIs of the total and each sublayer of the choroid were within the normal range in both groups of this study, based on results from large cohort studies [ 15 , 22 ]. However, there were notable relative differences in choroidal thickness between non-ocular sarcoidosis and healthy control groups. Specifically, total and all sublayers of the choroid were thicker in non-ocular sarcoidosis group compared to healthy control group. Moreover, the degree of choroidal thickening in non-ocular sarcoidosis group was significantly greater at HL than at SLCC, which contrasts with a previous report indicating predominant Sattler layer thickening in active sarcoid-related uveitis [ 7 ]. Furthermore, although it is reported that CVI increases along with choroidal enlargement in active intraocular inflammation, such as human leukocyte antigen-B26 related uveitis [ 23 ], no significant changes in CVIs were observed across all sublayers in non-ocular sarcoidosis group compared with the control group in this study. These findings suggest that choroidal thickening in all sublayers, especially HL, without changes in vascularity, is a characteristic choroidal manifestation of non-ocular sarcoidosis. We suspect that non-ocular sarcoidosis may be under subclinical inflammation, without apparent signs of intraocular inflammation, resulting in both vasodilation and stromal edema (increase of both luminal and stromal area), thereby leading to choroidal expansion without changes in vascular density. These characteristic choroidal alterations of non-ocular sarcoidosis captured on EDI SD-OCT may shed light on the pathophysiological understanding of how sarcoidosis initiates sarcoidosis-associated ocular inflammation from subclinical stage. It also implies that eyes may be more often affected by systemic sarcoidosis than previously known, considering subclinical changes.
Several reports demonstrated that a subsequent decrease in choroid thickness after steroid treatments when it is initially increased in response to the intraocular inflammation in conditions such as human leukocyte antigen-B27 related uveitis, Behçet's disease, and Vogt-Koyanagi-Harada disease [ 24 , 25 , 26 ]. Notably, in this non-ocular sarcoidosis group, steroid treatment also showed a significant association with choroidal thickness; Eyes treated with oral steroids had thinner choroid compared with eyes under observation. This choroidal response to the steroid treatment may further support that eyes with non-ocular sarcoidosis are under subclinical choroidal inflammation. Unfortunately, we could not identify serum biomarkers reflecting localized and subclinical choroidal inflammation status in eyes with non-ocular sarcoidosis; Choroidal thickness in the non-ocular sarcoidosis group did not show significant association with CRP (an inflammation marker in various inflammatory systemic diseases) [ 27 , 28 , 29 ] or ACE (a biomarker for systemic sarcoidosis, correlated with the granuloma burden and disease severity) levels [ 30 , 31 ]. Caution is needed in interpreting these results due to a time gap between blood tests and OCT acquisition caused by referral-to-ophthalmologic screening duration (mean 33.38 ± 41.12 days). Further prospective studies, including additional blood test components besides CRP and ACE, are necessary for validation of this issue.
Age and axial length are considered as significant factors influencing choroidal thickness, with older age and longer axial length associated with reduced total choroidal thickness [ 22 ]. However, in this study, a significant association between age and choroidal thickness was found only in healthy control eyes, not in those with non-ocular sarcoidosis. Furthermore, SE, which is expected to reflect axial length, also showed a significant association with choroidal thickness only in healthy control, not in non-ocular sarcoidosis. These findings suggest that pro-inflammatory environment of systemic sarcoidosis may exert a more substantial influence on choroidal thickness than age or axial length alone. While some studies [ 32 , 33 ] have reported a decrease in choroidal thickness proportional to the rise in intraocular pressure, and others [ 34 , 35 ] have suggested no correlation, this study found no significant association between intraocular pressure and choroidal thickness in both groups.
Our study had several limitations. First is a small sample size. Second is the retrospective study design. Thus, it was impossible to adjust all known confounding factors between groups, most importantly, axial length and diurnal variation. SE-matching and OCT image acquisition time-matching within 2 h difference may help mitigate this issue. Third is manual segmentation and measurement. The participation of two independent examiners and binarization at the standard threshold might overcome these challenges. Nonetheless, this study is meaningful because this is the first investigation of choroidal changes associated with systemic sarcoidosis without overt ocular sarcoidosis using EDI SD-OCT. The more detailed morphological characteristics of the choroidal vasculature in non-ocular sarcoidosis can be explored in further studies using wICGA analysis. A large-scale prospective longitudinal study is required to clarify whether the subclinical choroidal thickening in non-ocular sarcoidosis is a pre-inflammatory sign by evaluating whether they progress to overt ocular inflammation.
In conclusion, this study demonstrated that systemic sarcoidosis may have subclinical manifestations in the choroid, resulting in total and all sublayers thickening, especially HL, without significant vascularity changes. Early ophthalmologic screening using EDI-SD OCT is important to detect these subclinical choroidal changes in systemic sarcoidosis patients.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Grunewald J, Grutters JC, Arkema EV, Saketkoo LA, Moller DR, Muller-Quernheim J. Sarcoidosis. Nat Rev Dis Primers. 2019;5(1):45.
Article PubMed Google Scholar
Ungprasert P, Ryu JH, Matteson EL. Clinical manifestations, diagnosis, and treatment of sarcoidosis. Mayo Clin Proc Innov Qual Outcomes. 2019;3(3):358–75.
Article PubMed PubMed Central Google Scholar
Pasadhika S, Rosenbaum JT. Ocular sarcoidosis. Clin Chest Med. 2015;36(4):669–83.
Lee JH, Han YE, Yang J, Kim HC, Lee J. Clinical manifestations and associated factors of uveitis in patients with pulmonary sarcoidosis: a case control study. Sci Rep. 2023;13(1):22380.
Article CAS PubMed PubMed Central Google Scholar
Giorgiutti S, Jacquot R, El Jammal T, Bert A, Jamilloux Y, Kodjikian L, Sève P. Sarcoidosis-related uveitis: a review. J Clin Med. 2023;12(9):3194.
Gungor SG, Akkoyun I, Reyhan NH, Yesilirmak N, Yilmaz G. Choroidal thickness in ocular sarcoidosis during quiescent phase using enhanced depth imaging optical coherence tomography. Ocul Immunol Inflamm. 2014;22(4):287–93.
Mehta H, Sim DA, Keane PA, Zarranz-Ventura J, Gallagher K, Egan CA, Westcott M, Lee RW, Tufail A, Pavesio CE. Structural changes of the choroid in sarcoid- and tuberculosis-related granulomatous uveitis. Eye (Lond). 2015;29(8):1060–8.
Article CAS PubMed Google Scholar
Mittal A, Velaga SB, Falavarjani KG, Nittala MG, Sadda SR. Choroidal thickness in non-ocular Behçet’s disease - a spectral-domain OCT study. J Curr Ophthalmol. 2017;29(3):210–3.
Mochizuki M, Smith JR, Takase H, Kaburaki T, Acharya NR, Rao NA. International Workshop on Ocular Sarcoidosis Study Group: Revised criteria of International Workshop on Ocular Sarcoidosis (IWOS) for the diagnosis of ocular sarcoidosis. Br J Ophthalmol. 2019;103(10):1418–22.
Tan CS, Ouyang Y, Ruiz H, Sadda SR. Diurnal variation of choroidal thickness in normal, healthy subjects measured by spectral domain optical coherence tomography. Invest Ophthalmol Vis Sci. 2012;53(1):261–6.
Spaide RF, Koizumi H, Pozzoni MC. Enhanced depth imaging spectral-domain optical coherence tomography. Am J Ophthalmol. 2008;146(4):496–500.
Adhi M, Lau M, Liang MC, Waheed NK, Duker JS. Analysis of the thickness and vascular layers of the choroid in eyes with geographic atrophy using spectral-domain optical coherence tomography. Retina (Philadelphia, Pa). 2014;34(2):306–12.
Branchini LA, Adhi M, Regatieri CV, Nandakumar N, Liu JJ, Laver N, Fujimoto JG, Duker JS. Analysis of choroidal morphologic features and vasculature in healthy eyes using spectral-domain optical coherence tomography. Ophthalmology. 2013;120(9):1901–8.
Sim DA, Keane PA, Mehta H, Fung S, Zarranz-Ventura J, Fruttiger M, Patel PJ, Egan CA, Tufail A. Repeatability and reproducibility of choroidal vessel layer measurements in diabetic retinopathy using enhanced depth optical coherence tomography. Invest Ophthalmol Vis Sci. 2013;54(4):2893–901.
Agrawal R, Gupta P, Tan KA, Cheung CM, Wong TY, Cheng CY. Choroidal vascularity index as a measure of vascular status of the choroid: Measurements in healthy eyes from a population-based study. Sci Rep. 2016;6:21090.
Iovino C, Pellegrini M, Bernabei F, Borrelli E, Sacconi R, Govetto A, Vagge A, Di Zazzo A, Forlini M, Finocchio L, et al. Choroidal vascularity index: an in-depth analysis of this novel optical coherence tomography parameter. J Clin Med. 2020;9(2):595.
Koo TK, Li MY. A Guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–63.
Bill A, Sperber GO. Control of retinal and choroidal blood flow. Eye (Lond). 1990;4(Pt 2):319–25.
Williams TJ. Oedema and vasodilatation in inflammation: the relevance of prostaglandins. Postgrad Med J. 1977;53(625):660–2.
Wahlund CJE, Gucluler Akpinar G, Steiner L, Ibrahim A, Bandeira E, Lepzien R, Lukic A, Smed-Sörensen A, Kullberg S, Eklund A, et al. Sarcoidosis exosomes stimulate monocytes to produce pro-inflammatory cytokines and CCL2. Sci Rep. 2020;10(1):15328.
Baughman RP, Culver DA, Judson MA. A concise review of pulmonary sarcoidosis. Am J Respir Crit Care Med. 2011;183(5):573–81.
Zhao J, Wang YX, Zhang Q, Wei WB, Xu L, Jonas JB. Macular choroidal small-vessel layer, Sattler’s layer and Haller’s layer thicknesses: the Beijing Eye Study. Sci Rep. 2018;8(1):4411.
Kim M, Kim RY, Park YH. Choroidal vascularity index and choroidal thickness in human leukocyte antigen-b27-associated uveitis. Ocul Immunol Inflamm. 2019;27(8):1280–7.
Ahn SJ, Kim JH, Lee BR. Choroidal change in acute anterior uveitis associated with human leukocyte antigen-B27. PLoS ONE. 2017;12(6):e0180109.
Kim M, Kim H, Kwon HJ, Kim SS, Koh HJ, Lee SC. Choroidal thickness in Behcet’s uveitis: an enhanced depth imaging-optical coherence tomography and its association with angiographic changes. Invest Ophthalmol Vis Sci. 2013;54(9):6033–9.
Maruko I, Iida T, Sugano Y, Oyamada H, Sekiryu T, Fujiwara T, Spaide RF. Subfoveal choroidal thickness after treatment of Vogt-Koyanagi-Harada disease. Retina. 2011;31(3):510–7.
Aydin E, Atik S, Koc F, Balikoglu-Yilmaz M, Akin Sari S, Ozmen M, Akar S. Choroidal and central foveal thickness in patients with scleroderma and its systemic associations. Clin Exp Optom. 2017;100(6):656–62.
Gundogan FC, Akay F, Uzun S, Ozge G, Toyran S, Genç H. Choroidal thickness changes in the acute attack period in patients with familial Mediterranean fever. Ophthalmologica. 2016;235(2):72–7.
Steiner M, Del Mar Esteban-Ortega M, Thuissard-Vasallo I, García-Lozano I, García-González AJ, Pérez-Blázquez E, et al. Choroidal Thickness Is a Biomarker Associated With Response to Treatment in Ankylosing Spondylitis. J Clin Rheumatol. 2020. https://journals.lww.com/jclinrheum/abstract/9000/choroidal_thickness_is_a_biomarker_associated_with.98616.aspx .
Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. N Engl J Med. 2007;357(21):2153–65.
Studdy P, Bird R, James DG. Serum angiotensin-converting enzyme (SACE) in sarcoidosis and other granulomatous disorders. Lancet. 1978;2(8104–5):1331–4.
Hata M, Hirose F, Oishi A, Hirami Y, Kurimoto Y. Changes in choroidal thickness and optical axial length accompanying intraocular pressure increase. Jpn J Ophthalmol. 2012;56(6):564–8.
Wang YX, Jiang R, Ren XL, Chen JD, Shi HL, Xu L, Wei WB, Jonas JB. Intraocular pressure elevation and choroidal thinning. Br J Ophthalmol. 2016;100(12):1676–81.
Usui S, Ikuno Y, Akiba M, Maruko I, Sekiryu T, Nishida K, Iida T. Circadian changes in subfoveal choroidal thickness and the relationship with circulatory factors in healthy subjects. Invest Ophthalmol Vis Sci. 2012;53(4):2300–7.
Wei WB, Xu L, Jonas JB, Shao L, Du KF, Wang S, Chen CX, Xu J, Wang YX, Zhou JQ, et al. Subfoveal choroidal thickness: the Beijing Eye Study. Ophthalmology. 2013;120(1):175–80.
Download references
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (2018R1A5A1025511). The funding organization had no role in the design or conduct of this research.
Author information
Authors and affiliations.
Department of Ophthalmology, Asan Medical Center, University of Ulsan College of Medicine, 88, Olympic-Ro 43-Gil, Songpa-Gu, Seoul, 05505, Republic of Korea
Ye Eun Han, Jaehyuck Jo & Junyeop Lee
Department of Pulmonology and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, South Korea
Ho Cheol Kim
Translational Biomedical Research Group, Asan Institute for Life Science, Asan Medical Center, Seoul, South Korea
Junyeop Lee
You can also search for this author in PubMed Google Scholar
Contributions
J.L.: Conceptualization and methodology, Y.E.H. and J.J.: Formal analysis and investigation, writing original draft of paper, J.L. and H.C.K.: writing review and editing, Funding acquisition, supervision. All authors approved the submitted version.
Corresponding author
Correspondence to Junyeop Lee .
Ethics declarations
Ethics approval and consent to participate.
This study was reviewed and ethically approved by the Institutional Review Board of the Asan Medical Center, affiliated with the University of Ulsan College of Medicine, Seoul, South Korea (IRB number: 2021–1385). Written informed consent from patients were waived, considering the retrospective nature of the study, by the Institutional Review Board of the Asan Medical Center. The authors declare that this study complied with the tenets of the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Han, Y.E., Jo, J., Kim, H.C. et al. Choroidal manifestations of non-ocular sarcoidosis: an enhanced depth imaging OCT study. BMC Ophthalmol 24 , 199 (2024). https://doi.org/10.1186/s12886-024-03463-0
Download citation
Received : 16 June 2023
Accepted : 22 April 2024
Published : 26 April 2024
DOI : https://doi.org/10.1186/s12886-024-03463-0
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Sarcoidosis
- Choroidal thickness
- Choroidal vascularity index
- Enhanced depth imaging
- Spectralis-domain optical coherence tomography
BMC Ophthalmology
ISSN: 1471-2415
- General enquiries: [email protected]
- Open access
- Published: 22 April 2024
Off- to in-season body composition adaptations in elite male and female endurance and power event athletics competitors: an observational study
- Stefan Pettersson 1 , 2 ,
- Anton Kalén 2 , 3 ,
- Mikael Gustafsson 1 ,
- Stefan Grau 1 , 4 &
- Andreas Caspers 1
BMC Sports Science, Medicine and Rehabilitation volume 16 , Article number: 90 ( 2024 ) Cite this article
149 Accesses
1 Altmetric
Metrics details
Monitoring elite athletes’ body composition (BC) is vital for health and optimizing performance in sports emphasizing leanness, such as athletics. This study aims to investigate and compare sex- and event-specific off-to in-season BC changes in endurance and power event athletics competitors.
Elite male and female endurance athletes (> 800 m runners; n = 21) and power event athletes (sprinters, jumpers; n = 32) underwent dual-energy X-ray absorptiometry (DXA) scans for whole and regional lean mass (LM), fat mass (FM), bone mineral content (BMC), and density (BMD) during off-season (September-October) and in-season (April-May). Linear mixed models tested between-group off-season differences in BC, within-group off-season to in-season changes, and between-group differences in change. To assess meaningful or least significant changes (LSC) in BC, DXA precision errors were determined from two consecutive total body scans in a subsample of athletes ( n = 30).
Male athletes ( n = 26) gained significantly ( p < 0.05) more body mass (BM; mean difference 1.5 [95% confidence interval (CI):0.5–2.4] kg), LM (843 [95% CI:-253:1459] g), and trunk LM (756 [-502:1156] g) than female athletes ( n = 27). The proportion of changes in athlete’s BC exceeding the LSC threshold for LM and trunk LM were 70% and 65% in males, and 48% and 26% in females. Significant ( p < 0.05) within-group off-season to in-season increases in LM were found for male endurance and power athletes, and female power athletes. All groups significantly increased BMD ( p < 0.05). Only male and female power athletes had significant in- to-off-season increases in BMC. 80% of all athletes who had a meaningful increase in BMC belonged to the power event group. No significant within- or between group change in FM was observed.
Conclusions
The present study found that male athletes gained more BM, LM and trunk LM than females. Within-group increases in regional and whole-body LM and BMC were predominantly found among power event competitors. Incorporating individual meaningful changes alongside traditional statistics provided additional insights into sex and event-group differences. Future research on elite athletic event groups should include DXA measurements closer to major outdoor-season competitions, coupled with site-specific measures (ultrasound, MRI) for better detection of subtle changes in LM and FM.
Peer Review reports
Introduction
Estimation of whole and regional body composition (BC) may be valuable for improving performance, injury prevention, and assessing health risks in athletes [ 1 ]. Generally, a high power-to weight-ratio, characterized by a greater proportion of lean mass (LM), of which a significant fraction is skeletal muscle, and a lower proportion of fat mass (FM) is considered crucial for locomotion and athletic performance [ 2 ]. On the other hand, an excessive focus on obtaining a low body mass (BM) and FM content has been related to negative outcomes, including decreased bone mineral density (BMD), reduced LM, disordered eating habits and menstrual dysfunction [ 3 ]. Monitoring changes of BC during an athletic season can provide vital information for coaches, athletes, and sport medicine professionals. It facilitates the evaluation of training program effectiveness, and identification of potential health and injury risks in sports emphasizing leanness such as athletics (track and field).
Numerous studies have examined BC in athletics athletes across various events, including middle- to long-distance running (800 m to marathon), sprinting (60–400 m including hurdles), jumping (long jump, triple jump, high jump, pole vault) and throwing (shot put, javelin, discus, hammer) [ 4 , 5 , 6 , 7 , 8 , 9 , 10 ]. Each event category imposes distinct physical demands that necessitate specific anthropometric dimensions and BC for optimal performance. For example, research on middle- to long-distance runners has demonstrated an inverse relationship between regional, total, and relative FM (%FM) and performance, while LM has been positively associated with higher aerobic capacity (e.g., V̇O 2 max) in both male and female runners [ 11 , 12 , 13 , 14 ].
Similarly, sprinters and jumpers, known as power event athletes, typically exhibit a lean physique [ 15 , 16 ]. Cross-sectional studies have demonstrated that the fastest sprinters tend to possess the greatest lower body muscle mass [ 17 , 18 , 19 ]. These findings suggest that during the transition from the off-season to the competitive season, endurance event athletes may benefit from a gradual reduction in total BM by decreasing FM while minimizing changes in LM. Conversely, power event athletes may benefit from increasing LM, particularly in thigh skeletal muscle mass thickness. Studies conducted by Stanforth et al. [ 9 ] and Carbuhn et al. [ 5 ] have reported reductions in FM and %FM, accompanied by increases in LM and BMD over the course of a competitive season in female sprinters and jumpers. However, it is essential to consider the disparities in training methods between sprinters/jumpers (involving sprinting, plyometric exercises, and power lifts) and middle- to long-distance runners (primarily comprising high-volume, low-intensity aerobic exercise). These divergent training approaches likely influence seasonal changes in BC in an event-specific manner [ 20 , 21 ], however event comparisons have not been systematically researched with regards to BC methodology.
Dual-energy X-ray absorptiometry (DXA) has become an increasingly popular method for quantifying whole and regional FM, LM, BMD, and bone mineral content (BMC) in athletes [ 22 ]. While DXA is renowned for its excellent reproducibility, it is important to acknowledge that both biological factors (such as age, sex, body size, prior exercise, and acute food and fluid intake) and technical factors (DXA model, scan mode, and subject positioning on the scanning bed) can contribute to measurement errors [ 22 ]. Although adhering to a meticulous scanning protocol can mitigate some of these issues, understanding the measurement precision of the DXA device is crucial for interpreting meaningful changes when conducting consecutive BC measurements. The International Society for Clinical Densitometry (ISCD) recommends the use of the least significant change (LSC), which is calculated based on the precision error for a specific group. The LSC represents the smallest change in a BC variable that can be considered beyond the margin of error or the inherent variability in the measurement process. The objective of this study was to assess variations in BC changes between sex and event categories, and to determine the proportion of athletes who had BC changes that exceeded the DXA’s LSC.
From a prospective cohort study consisting of 96 participants, which aimed to investigate risk factors and injuries over an eleven-month athletics season [ 23 ], a subsample of 53 elite athletics competitors (26 males (M), 27 females (F)) aged 22.2 ± 2.8 years, were selected for inclusion in this study. The majority of these athletes were part of the Swedish national team and regularly participated in international events. All participants were required to be over 18 years of age, resulting in the exclusion of n = 35 athletes from the initial cohort study. Additionally, one athlete who ceased training due to severe injury for more than three consecutive weeks (10% of the study duration), between the off-season and in-season DXA measurement periods, was excluded from the analysis. Four athletes underwent the off-season DXA measurement, but not the in-season scan and were therefore excluded. Three throwing event athletes were also excluded due to their significantly different training plans, both in terms of frequency and content, compared to the other included event categories (see below). The study was conducted in accordance with the declaration of Helsinki [ 24 ], and all procedures were approved by the Regional Ethical Committee in Gothenburg (dnr. 723–16), Sweden. Additionally, all athletes gave their written informed consent.
DXA measurements
After an overnight fast, the athletes had their BM measured on a digital scale (Seca 764, Hamburg, Germany) to the nearest 0.1 kg while wearing underwear only. Height was measured to the nearest 0.5 cm with a standard wall-mounted stadiometer. Subsequently, BC was assessed using a fan-beam DXA scanner (iDXA GE Medical Systems, Madison, WI, USA) in the standard mode as determined automatically by the DXA software (EnCore, version 16.10) based on BMI. The athletes were positioned in a supine position, centrally aligned with their extremities fitting inside the measuring parameter and their feet and hands placed in custom-made radio-opaque positioning aids [ 22 ]. All scans were inspected for regions of interest misalignments and artefacts by two experienced technicians. The EnCore software automatically calculated whole- and regional FM, LM, BMC, BMD, and BMD Z-score. BMD Z-scores were calculated using the combined NHANES/Lunar database. Fat mass index (FMI) and fat-free mass index (FFMI) were calculated using the following formulas:
The DXA assessments were conducted at two seasonal periods defined in this study: off-season assessments were completed after the outdoor athletic season (September-October), while in-season assessments were conducted at the beginning of the outdoor athletic season (April-May). DXA measurements were conducted during two seasonal periods: off-season assessments occurred after the outdoor athletic season (September-October), while in-season assessments were done at the beginning of the outdoor athletic season (April-May). Time between the off-season and in-season measurements was 5.7 ± 0.7 months. The athletes were classified into one of two event categories: Endurance athletes (M/F = 9/12) competing in running events from 800 m to 10,000 m and Power athletes (M/F = 17/15) including sprinters (M/F = 14/7), long- (F = 1), triple- (M/F = 2/1) and high jumpers (F = 1) and pole-vaulters (M/F = 1/5).
Following the ISCD guidelines [ 25 ], a precision estimation of the DXA equipment was performed on a subsample of the athletes ( n = 30; M/F = 15/15; height 176 ± 6.9, BMI = 21.6 ± 2.0) who underwent duplicate scans with dismounting and repositioning on the scanning bed between measurements. The LSC was calculated following the recommended approach by the ISCD: RMS-SD × 2.77 (95% confidence interval (CI)), see Table 1 .
Training frequencies
Supplementary Fig. 1 provides information on the monthly number of training sessions and training days from October to April. The mean training hours per week (14 ± 3 h) did not significantly differ between event categories or sexes. Throughout the study period, the endurance athletes performed approximately two resistance training sessions per week, while the majority of the power athletes engaged in four strength sessions per week from October to December and two sessions per week from January to April, (as per personal communication with the strength and conditioning coaches).
Statistical analysis
Linear mixed model was fitted for each variable using cluster-robust standard errors. Time (off-season or in-season), sex (male or female), and event type (endurance or power), along with their two- and three-way interactions were included as fixed factors. The model contained a random intercept for each athlete. Difference in estimated marginal means from the models were used to test for between-group off-season differences in BC, within-group off-season to in-season change, and for between-group differences in change.
Based on the LSC calculations (Table 1 ), the off-season to in-season change of each athlete was categorized as meaningful increase, no change or decrease. All statistical analyses were conducted using R software (version 4.1.2). A significance level of p < 0.05 was used to determine statistical significance, and the Benjamini–Hochberg procedure was applied to control for the false discovery rate in all contrasts.
Off-season sex- and event-specific differences in BC
The overall off- and in-season whole and regional BC estimates of the athletes are presented in Table 2 , and off-season sex and event differences (mean [lower: upper, 95% CI]) can be found in Supplementary Table 1 . Male athletes had significantly higher BM, FFMI, BMD, BMD Z-score and total and regional LM and BMC than female athletes (p ≤ 0.042). Males, in comparison to females, also had lower FMI, %FM and total and regional FM ( p ≤ 0.006; Table 2 and Supplementary Table 1 ), except for trunk FM (mean difference − 568; [-1280: 144] g; p = 0.116).
Off-season event comparisons showed that power athletes ( n = 32) had significantly higher BM, FFMI, BMD, BMD Z-score, FMI, and FM, and total- and regional LM and BMC ( p ≤ 0.02) than endurance athletes ( n = 21), while no significant differences between events in % FM and arms FM were observed.
Male power athletes had significantly higher FFMI, FMI, BMC, BMD and BMD Z-score ( p ≤ 0.046) than male endurance athletes, but no significant differences in LM, FM, %FM or BM were observed (mean group BM difference 6.0 [0.6: 11.4] kg; p = 0.051). Female power athletes had, except for total %FM ( p = 0.058) and arms FM ( p = 0.072), significantly higher off-season BMD, BMD Z-score and total- and regional LM, BMC, and FM than the female endurance athletes ( p ≤ 0.041, see Table 2 and Supplementary Table 1 ).
Sex and event-type off- to in-season BC changes
Table 2 presents the within-group differences in total and regional body composition estimates from the off-season to the in-season. Additionally, Fig. 1 illustrates the changes in total body and trunk LM, FM, and BMC from the off- to in-season periods, while Fig. 2 displays the alterations in BC specifically in the extremities (arms and legs). No significant change in absolute or %FM was observed. The male athletes gained 1.1 kg in BM (0.5: 1.8 kg; p = 0.004), a BM change which mainly consisted of LM accretion (mean change 1257 g, [757: 1757] g, p < 0.001) in the trunk and legs (mean change 851 g and 363 g, p = < 0.001 and p = 0.009, respectively). Consequently, mean FFMI increased by 0.4 kg/m 2 ( p < 0.001) and significant increases in BMD, BMD Z-score, total BMC, and legs BMC were also noted ( p ≤ 0.015).

Individual off-season to in-season changes in whole body (a, c, e) and trunk (b, d, f) composition in elite male and female endurance and power athletics event competitors ( n = 53). Grey area represents least significant change (LSC)-95% confidence interval, i.e., precision error of DXA measurement. The green lines represent athletes who experienced off- to in-season changes in LM, FM, and BMC that exceeded the LSC threshold. Red lines indicate athletes who experienced reductions surpassing the LSC threshold, while purple lines represent athletes who neither increased nor reduced beyond the LSC threshold

Individual off-season to in-season changes in legs (a, c, e) and arms (b, d, f) composition in elite male and female endurance and power athletics event competitors ( n = 53). Grey area represents least significant change (LSC)-95% confidence interval, i.e., precision error of DXA measurement. The green lines represent athletes who experienced off- to in-season changes in LM, FM, and BMC that exceeded the LSC threshold. Red lines indicate athletes who experienced reductions surpassing the LSC threshold, while purple lines represent athletes who neither increased nor reduced beyond the LSC threshold
Figure 3 illustrates mean changes in total and regional LM and BMC for power and endurance athletes, respectively. The male power athletes significantly increased BM (mean change 1.4 [0.6: 2.3] kg), LM (1416 [703 to 2130] g) and arms, legs, and trunk LM and FFMI ( p ≤ 0.023). BMD, BMD Z-score (Fig. 4 ), total BMC, and legs and arms BMC were also higher in-season than at off-season ( p ≤ 0.023), while no significant change was noted for FM variables except an increase in arms FM ( p = 0.023). In male endurance athletes, increments in LM (1097 [396: 1797] g; p = 0.019), trunk LM (1089 g; p = 0.001) and FFMI (0.3 kg/m 2 ; p = 0.019) were the only significant BC changes noted.
For the female athletes ( n = 27) no significant changes were found for whole or regional FM and LM variables, except legs LM which increased by 275 g from off-season to in-season (79: 475 g, p = 0.030). Furthermore, female athletes BMD, BMD Z-score, total BMC and legs BMC were significantly ( p ≤ 0.030) higher at in-season than off-season.
Female power athletes significantly increased LM (mean change 618 [133: 1103] g, p = 0.041) and FFMI (0.2 kg/m 2 , p = 0.041), total BMC and BMD (22 g and 0.039 g/cm 2 , p = 0.024 and p = 0.001, respectively) and BMD Z-score ( p = 0.008) but also legs LM (324 [67: 581] g; p = 0.041) and legs BMC (12 [4: 19] g; p = 0.024). In the female endurance athlete group, the only significant BC change observed over the course of the season were increased legs BMC (mean change 11 [6: 17] g; p = 0.001) and BMD Z-score (mean change 0.35 [0.15:0.55] p = 0.009).

Mean off- to in-season whole and regional lean mass and bone mineral content (BMC) changes in elite male and female power ( n = 32) and endurance ( n = 21) athletics event competitors. Grey area represents least significant change (LSC)-95% confidence interval, i.e., precision error of DXA measurement

Off-season (Off) to in-season (In) changes in whole-body bone mineral density (BMD) Z-scores among elite female and male competitors in power (F: n = 15, M: n = 17) and endurance (F: n = 12, M: n = 9) athletics events. The box plots depict the mean BMD Z-score and the range of values (min-max distribution). Significant indicators denote within-group off- to in-season changes
Sex and event-type differences in off- to in-season BC changes
The results of the sex and event-type differences in off- to in-season BC changes, including 95% CI and p-values, are presented in Supplementary Table 2 . Male athletes gained significantly more BM (mean difference 1.5 [0.5: 2.4] kg; p = 0.027), LM (mean difference 843 [-253: 1459] g; p = 0.048) and Trunk LM (mean difference 756 [-502: 1156] g; p = 0.007) than female athletes. No other significant differences in BC change were found for sex and event-type.
Meaningful off- to-in-season BC changes
The figures (Figs. 1 , 2 and 3 ) present the number of athletes surpassing the LSC estimates for alterations in whole- and regional LM, BMC, BMD, and FM between the off-season and in-season, while additional statistical inferences are provided in Supplementary Table 3 . Notably, 58% of all athletes (20 power and 11 endurance) experienced a substantial increase (> 496 g) in LM whereas six athletes (11% of the total sample) exhibited a meaningful decrease in LM (> -496 g). In terms of regional LM changes, 51% and 45% respectively demonstrated a significant increase in leg LM (> 417 g) and trunk LM (> 417 g), while five athletes exhibited a decrease in leg LM (see Figs. 1 d and 2 c).
30% of athletes exhibited a verifiable increase, while 40% demonstrated a noteworthy decrease in whole-body FM (LSC = ± 396 g). Among all athletes, 32% ( n = 17) exhibited an increase in leg FM (> 202 g) with a similar relative distribution across sex and event groups (27–35%, Supplementary Table 4 ). One-third of participants ( n = 13) displayed a meaningful decrease in leg FM (Supplementary Table 4 and Fig. 2 a).
All participants had high off-season BMD (1.35 ± 0.11 cm 2 , min-max = 1.14–1.65 cm 2 ) and high BMD Z-score (2.23 ± 1.1, min-max = 0.0–5.3) values; however, 30% ( n = 16) demonstrated a meaningful increase in whole-body BMC (> 21 g), with the majority (81%) comprising power athletes ( n = 13; M/F = 8/5, Fig. 1 e). Three athletes showcased a decrease in whole-body BMC (Figs. 2 e and 3 ) that exceeded the LSC. 38% of all athletes experienced a meaningful increase (> 14 g) in leg BMC, with a larger proportion of the male power athletes (47%; n = 8) compared to the other three groups (33%, respectively).
The study aimed to investigate and compare changes in BC among elite athletics competitors during the transition from off-season to in-season, focusing on sex- and event-related variations. The results highlighted significant increases in BM, total LM, and trunk LM in male athletes compared to females. Significant within-group off-season to in-season increases in regional and whole-body LM, BMC and BMD Z-score were more prominent in power athletes than in endurance athletes. About 60% and 30% of all athletes demonstrated a meaningful increase in LM and BMC, respectively. For BMC, 80% of power athletes had a true increase, distributed equally between sexes. No significant changes were observed in any variable related to FM, except for an increase in arms FM in male power athletes.
Off- to in-season changes in LM
Sex comparisons revealed that male athletes, in contrast to females, exhibited a significant increase in LM and trunk LM from the off-season to the in-season period. The initial lower LM in females during the off-season may induce bias in favor of their increases in both total and trunk LM [ 26 ]. Other factors, such as differences in FFMI during the off-season could also contribute to the observed variation in LM accrual. Although we did not find any significant within- or between-group associations between off-season LM/FFMI and change in LM/FFMI (likely due to small sample sizes), female athletes in power and endurance events exhibited higher off-season FFMI compared to normative sport-specific FFMI values [ 27 ]. In contrast, male athletes had lower off-season muscularity index (FFMI = 19.0 ± 1.5) compared to previously reported values in aged-matched male track and field athletes (FFMI = 22.4 ± 3.7) [ 28 ], suggesting a greater potential for LM increase than in the female athletes. However, it is important to note that skeletal muscle mass only makes up for approximately 30% of total trunk LM [ 29 ]. Still, 68% of the total LM accrual in male athletes consisted of trunk LM, while in females, this proportion was 23%. Previous research on healthy non-athletes [ 30 ] and world-class powerlifters [ 31 ] has indicated that females generally exhibit lower trunk muscle thickness/mass compared to males, implying a lesser potential for significant increases in trunk skeletal mass and thus absolute trunk LM. Sex-differences in trunk LM accrual was also observed regarding meaningful changes, with 25% of all female endurance and power athletes exceeding the LSC, compared to 65% of their male counterparts, respectively.
While no significant between-event-group comparisons were found, there were significant within-group increases in LM observed in all groups, except for female endurance athletes. The off- to in-season increases in LM in the male and female power event group concur with previous findings in male and female NCAA Division 1 jumpers and sprinters [ 5 , 32 ] studied during the same period of the training year as the present study. Correspondingly, Trinschek and colleagues [ 33 ] showed that the percentage of LM in elite male polish endurance runners and sprinters significantly increased between consecutive phases of the annual training cycle. Considering that even modest resistance training frequencies have been shown to be effective in increasing muscle mass and strength [ 34 ] the inclusion of two (for endurance athletes) up to four (for power athletes) resistance training sessions per week during the study period is a plausible explanation as to why almost all athletes (87%) in the present study were able to maintain (28%) or increase (59%) LM above the LSC threshold. However, although the DXA in this study demonstrated commendable short-term precision error values for total LM (0.3%), below the ISCD [ 25 ] recommended limit (LM < 2%), future research should consider combining DXA with site-specific measures (ultrasound, CT, MRI) for improved detection of subtle seasonal changes in LM between different athletic events [ 35 ].
Off- to in-season changes in FM
Contrarily to LM changes, no significant within- or between-group reductions in whole body FM, or %FM, were observed. Off-season %FM ranged from 11.6 to 19.3% (endurance males and female power athletes, respectively) which is similar to some studies [ 9 , 33 ], but higher than other previously published DXA-derived off-season FM values in elite athletics athletes [ 32 ]. Low initial (off-season) FM levels of athletes have previously been suggested as a possible explanation for the lack of change observed during different seasons of training and/or competition [ 36 ]. However, considering that the athletes off-season FM levels in the present cohort are well above the minimum %FM cut-off values proposed by the International Olympic Committee´s Medical Commission [ 3 ] (i.e., < 5 and 12%, males and females respectively), an alternative explanation for the lack of significant off- to in-season change in FM could be the timing of the present study’s BC measurements in relation to the annual training cycle. A systematic review [ 37 ] demonstrated that male and female endurance athletes had a significantly lower percentage of FM during the competition phase compared to the preparation phase, and Mangine et al. [ 32 ] recently reported a ∼ 5% reduction in %FM in collegiate male and female sprint and power athletes between the return from winter break (early January) and the end of the indoor season (early April) but a substantially higher reduction ( ∼ 20%) between April and late May (before the NCAA Championships). Thus, future research on seasonal changes in FM should consider additional BC measurements closer to major outdoor-season competitive events. Nevertheless, the results of the present investigation are still highly relevant since prioritization of BM/FM loss in athletes is generally recommended to take place before, not during, the competitive season [ 3 ]. It is also worth noting that although the present study’s short-term precision error value for total FM (1.3%) was below the recommended limit by the ISCD [ 25 ] (< 3%), it was still considerably high compared to whole body CV’s of LM, BMC and BMD.
Off- to in-season changes in BMC and BMD
Within-group analysis revealed a significant off- to in-season increase in BMD Z-score for all groups. However, only male and female power athletes demonstrated a significant increase in whole-body BMC. Carbuhn et al. [ 5 ] discovered similar off- to in-season mean increases in absolute and relative BMC (26 g and ∼ 0.9% BMC increase, respectively) among collegiate female sprinters and jumpers, as observed in our female power event cohort (22 g and ∼ 0.8% BMC increase, respectively). However, the present LSC-analysis revealed that only 40% of the female sprinters and jumpers experienced a meaningful increase in BMC (≥ 21 g). Furthermore, the majority ( ∼ 80%) of athletes with a meaningful increase in BMC belonged to the power event group, with equal relative distribution between sexes. However, within-group off- to in-season changes in BMD found that both male/female power athletes and female endurance athletes significantly increased BMD (male endurance athletes p = 0.054; BMD Z-score significantly increased in all groups). This finding aligns with previous research [ 38 ] indicating that while the axial loading and weight-bearing nature of middle- to long-distance running can enhance bone turnover and increase BMD, the heavier power event athletes, who impose a greater vertical load on the skeleton, may further augment BMD deposition. Furthermore, all athletes were found to have high whole-body BMD (e.g., a Z-score above − 1.0) [ 39 ]. It is also important to note that three athletes experienced a meaningful decrease in BMC, highlighting the clinical relevance of LSC estimates [ 3 ].
Strength and limitations of the study
The study prioritized a high level of measurement precision by conducting fasted state DXA scans with a standardized positioning protocol [ 22 ]. Another strength of the study was the adherence to recommended guidelines by the ISCD in performing reliability statistics on a subsample of the athletes being studied. Limitations include the small sample size of the participant group, the lack of access to more detailed training diaries, and the absence of data on the athletes’ dietary intake. Training diaries should be developed in close cooperation with the athletes’ coaches to increase compliance, and could be based on e.g., volume and type of training. A 7-day diet-monitoring period during both off- and in-season could have offered insights into implementing periodized energy and macronutrient intakes for changes in BC [ 40 ]. Finally, previous DXA research has illustrated racial differences in body proportion, fat-free mass (FFM) density, and BMD [ 41 ]. Thus, the limited ethnic diversity observed within the current study’s cohort (all Caucasian/White) hinders the ability to generalize these findings to broader populations [ 41 ].
The present study revealed significant sex differences in off-to-in-season changes in total BM, LM, and trunk LM. Significant within-group increases were observed in regional and whole-body LM, BMC, predominantly among power event athletes. Even though all athletes had high off-season BMD, almost all athletes increased BMD over the six-month period. Supplementing traditional statistics with individual meaningful changes in BC also yielded additional insights into the practical relevance of off-to-in-season differences. For example, even though there was a statistically significant difference in BMC in male and female power athletes from off-to-in-season, only 40% in each group showed a meaningful change. Furthermore, it is advisable to include additional DXA measurements closer to major outdoor-season events, coupled with site-specific measures (ultrasound, MRI), to enhance the detection of subtle changes in LM and FM.
Data availability
The datasets used during the current study are available from the corresponding author on reasonable request.
Abbreviations
Body composition
Bone mineral content
Bone mineral density
Confidence interval
Coefficients of variation
- Dual-energy X-ray absorptiometry
Fat-free mass index
Fat mass index
International Society for Clinical Densitometry
- Least significant change
Standard deviation
Ackland TR, Lohman TG, Sundgot-Borgen J, Maughan RJ, Meyer NL, Stewart AD et al. Current status of body composition assessment in sport: review and position statement on behalf of the ad hoc research working group on body composition health and performance, under the auspices of the I.O.C. Medical Commission. Sports medicine (Auckland, NZ). 2012;42(3):227–49.
Thomas DT, Erdman KA, Burke LM. Position of the Academy of Nutrition and Dietetics, dietitians of Canada, and the American College of Sports Medicine: Nutrition and athletic performance. J Acad Nutr Diet. 2016;116(3):501–28.
Article PubMed Google Scholar
Sundgot-Borgen J, Meyer NL, Lohman TG, Ackland TR, Maughan RJ, Stewart AD, et al. How to minimise the health risks to athletes who compete in weight-sensitive sports review and position statement on behalf of the Ad Hoc Research Working Group on Body Composition, Health and Performance, under the auspices of the IOC Medical Commission. Br J Sports Med. 2013;47(16):1012–22.
Bennell KL, Malcolm SA, Khan KM, Thomas SA, Reid SJ, Brukner PD, et al. Bone mass and bone turnover in power athletes, endurance athletes, and controls: a 12-month longitudinal study. Bone. 1997;20(5):477–84.
Article CAS PubMed Google Scholar
Carbuhn AF, Fernandez TE, Bragg AF, Green JS, Crouse SF. Sport and training influence bone and body composition in women collegiate athletes. J Strength Conditioning Res. 2010;24(7):1710–7.
Article Google Scholar
Fields JB, Merrigan JJ, White JB, Jones MT. Body composition variables by Sport and Sport-position in Elite Collegiate athletes. J Strength Conditioning Res. 2018;32(11):3153–9.
Hirsch KR, Smith-Ryan AE, Trexler ET, Roelofs EJ. Body composition and Muscle Characteristics of Division I track and field athletes. J Strength Conditioning Res. 2016;30(5):1231–8.
Spenst LF, Martin AD, Drinkwater DT. Muscle mass of competitive male athletes. J Sports Sci. 1993;11(1):3–8.
Stanforth PR, Crim BN, Stanforth D, Stults-Kolehmainen MA. Body composition changes among female NCAA division 1 athletes across the competitive season and over a multiyear time frame. J Strength Conditioning Res. 2014;28(2):300–7.
Vucetić V, Matković BR, Sentija D. Morphological differences of elite Croatian track-and-field athletes. Coll Antropol. 2008;32(3):863–8.
PubMed Google Scholar
Brandon LJ, Boileau RA. The contribution of selected variables to middle and long distance run performance. J Sports Med Phys Fit. 1987;27(2):157–64.
CAS Google Scholar
Brandon LJ, Boileau RA. Influence of metabolic, mechanical and physique variables on middle distance running. J Sports Med Phys Fit. 1992;32(1):1–9.
Hetland ML, Haarbo J, Christiansen C. Regional body composition determined by dual-energy X-ray absorptiometry. Relation to training, sex hormones, and serum lipids in male long-distance runners. Scand J Med Sci Sports. 1998;8(2):102–8.
Yoshiga CC, Higuchi M. Oxygen uptake and ventilation during rowing and running in females and males. Scand J Med Sci Sports. 2003;13(6):359–63.
Malina RM, Harper AB, Avent HH, Campbell DE. Physique of female track and field athletes. Med Sci Sports. 1971;3(1):32–8.
CAS PubMed Google Scholar
Pipes TV. Body composition characteristics of male and female track and field athletes. Res Q. 1977;48(1):244–7.
Kubo K, Ikebukuro T, Yata H, Tomita M, Okada M. Morphological and mechanical properties of muscle and tendon in highly trained sprinters. J Appl Biomech. 2011;27(4):336–44.
Kumagai K, Abe T, Brechue WF, Ryushi T, Takano S, Mizuno M. Sprint performance is related to muscle fascicle length in male 100-m sprinters. Journal of applied physiology (Bethesda, Md: 1985). 2000;88(3):811-6.
Sugisaki N, Kanehisa H, Tauchi K, Okazaki S, Iso S, Okada JJIJS et al. The relationship between 30-m sprint running time and muscle cross-sectional areas of the psoas major and lower limb muscles in male college short and middle distance runners. 2010:1101140066-.
Haugen T, Seiler S, Sandbakk Ø, Tønnessen E. The training and development of Elite Sprint performance: an integration of Scientific and best practice literature. Sports Med - open. 2019;5(1):44.
Article PubMed PubMed Central Google Scholar
Tjelta, LIJIJoSS. Coaching. The training of international level distance runners. 2016;11(1):122– 34.
Nana A, Slater GJ, Stewart AD, Burke LM. Methodology review: using dual-energy X-ray absorptiometry (DXA) for the assessment of body composition in athletes and active people. Int J Sport Nutr Exerc Metab. 2015;25(2):198–215.
Lundberg Zachrisson A, Ivarsson A, Desai, Karlsson J, Grau S. Risk factors for overuse injuries in a cohort of elite Swedish track and field athletes. BMC Sports Sci Med Rehabilitation. 2021;13(1):73.
Association GAotWM. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. J Am Coll Dent. 2014;81(3):14–8.
Google Scholar
Hangartner TN, Warner S, Braillon P, Jankowski L, Shepherd J. The Official positions of the International Society for Clinical Densitometry: acquisition of dual-energy X-ray absorptiometry body composition and considerations regarding analysis and repeatability of measures. J Clin Densitometry: Official J Int Soc Clin Densitometry. 2013;16(4):520–36.
Alway SE, Grumbt WH, Gonyea WJ, Stray-Gundersen J. Contrasts in muscle and myofibers of elite male and female bodybuilders. Journal of applied physiology (Bethesda, Md: 1985). 1989;67(1):24–31.
Blue MNM, Hirsch KR, Pihoker AA, Trexler ET, Smith-Ryan AE. Normative fat-free mass index values for a diverse sample of collegiate female athletes. J Sports Sci. 2019;37(15):1741–5.
Currier BS, Harty PS, Zabriskie HA, Stecker RA, Moon JM, Jagim AR, et al. Fat-Free Mass Index in a diverse sample of male Collegiate athletes. J Strength Conditioning Res. 2019;33(6):1474–9.
McCarthy C, Tinsley GM, Bosy-Westphal A, Müller MJ, Shepherd J, Gallagher D, et al. Total and regional appendicular skeletal muscle mass prediction from dual-energy X-ray absorptiometry body composition models. Sci Rep. 2023;13(1):2590.
Article CAS PubMed PubMed Central Google Scholar
Abe T, Kearns CF, Fukunaga T. Sex differences in whole body skeletal muscle mass measured by magnetic resonance imaging and its distribution in young Japanese adults. Br J Sports Med. 2003;37(5):436–40.
Abe T, Bell ZW, Wong V, Spitz RW, Yamada Y, Song JS, et al. Skeletal muscle size distribution in large-sized male and female athletes. Am J Hum Biology: Official J Hum Biology Council. 2021;33(2):e23473.
Mangine GT, Mangine GT, Eggerth A, Gough J, Stratton MT, Feito Y, et al. Endocrine and body composition changes across a competitive season in Collegiate speed-power track and field athletes. J Strength Conditioning Res. 2021;35(8):2067–74.
Trinschek J, Zieliński J, Kusy K. Maximal oxygen uptake adjusted for skeletal muscle Mass in competitive speed-power and endurance male athletes: changes in a one-year training cycle. Int J Environ Res Public Health. 2020;17(17).
Gomes GK, Franco CM, Nunes PRP, Orsatti FL. High-frequency resistance training is not more effective than low-frequency resistance training in increasing muscle Mass and Strength in Well-trained men. J Strength Conditioning Res. 2019;33(Suppl 1):S130–9.
Levine JA, Abboud L, Barry M, Reed JE, Sheedy PF, Jensen MD. Measuring leg muscle and fat mass in humans: comparison of CT and dual-energy X-ray absorptiometry. Journal of applied physiology (Bethesda, Md: 1985). 2000;88(2):452-6.
Koutedakis Y. Seasonal variation in fitness parameters in competitive athletes. Sports Med (Auckland NZ). 1995;19(6):373–92.
Article CAS Google Scholar
Heydenreich J, Kayser B, Schutz Y, Melzer K. Total energy expenditure, Energy Intake, and body composition in Endurance Athletes across the Training Season: a systematic review. Sports Med - open. 2017;3(1):8.
Maïmoun L, Sultan C. Effects of physical activity on bone remodeling. Metab Clin Exp. 2011;60(3):373–88.
Jonvik KL, Torstveit MK, Sundgot-Borgen J, Mathisen TF. Do we need to change the guideline values for determining low bone mineral density in athletes? Journal of applied physiology (Bethesda, Md: 1985). 2022;132(5):1320-2.
Magkos F, Yannakoulia M. Methodology of dietary assessment in athletes: concepts and pitfalls. Curr Opin Clin Nutr Metab Care. 2003;6(5):539–49.
Stults-Kolehmainen MA, Stanforth PR, Bartholomew JB, Lu T, Abolt CJ, Sinha R. DXA estimates of fat in abdominal, trunk and hip regions varies by ethnicity in men. Nutr Diabetes. 2013;3(3):e64.
Download references
Acknowledgements
The authors wish to thank the athletes who volunteered to participate in this study.
Open access funding provided by University of Gothenburg.
Author information
Authors and affiliations.
Center for Health and Performance, Department of Food and Nutrition, and Sport Science, University of Gothenburg, Gothenburg, Sweden
Stefan Pettersson, Mikael Gustafsson, Stefan Grau & Andreas Caspers
Swedish Olympic Committee, Sofiatornet, Olympiastadion, Stockholm, Sweden
Stefan Pettersson & Anton Kalén
Department of Computer Science, Electrical and Space Engineering, Luleå University of Technology, Luleå, Sweden
Anton Kalén
Department of Sports Medicine, University Clinic Tübingen, Tübingen, Germany
Stefan Grau
You can also search for this author in PubMed Google Scholar
Contributions
SP, AC and SG contributed to the original idea, study design and the conception of the work. AC and SP performed measurements and AK performed all statistical analysis except for the DXA’s reliability statistics (MG). SP wrote the main manuscript text. SP, AK, MG, AC and SG revised and edited the manuscript. All authors have read and approved the manuscript.
Corresponding author
Correspondence to Stefan Pettersson .
Ethics declarations
Ethics approval and consent to participate.
All participants were informed of the potential risks, benefits, and dissemination of the research before providing written informed consent to participate. Furthermore, all participants provided voluntary written informed consent prior to their involvement in the study. During the study process the authors followed the rules of the Helsinki Declaration. Ethics approval was obtained from the Regional Ethical Committee in Gothenburg (dnr. 723–16), Sweden.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Pettersson, S., Kalén, A., Gustafsson, M. et al. Off- to in-season body composition adaptations in elite male and female endurance and power event athletics competitors: an observational study. BMC Sports Sci Med Rehabil 16 , 90 (2024). https://doi.org/10.1186/s13102-024-00877-7
Download citation
Received : 07 July 2023
Accepted : 03 April 2024
Published : 22 April 2024
DOI : https://doi.org/10.1186/s13102-024-00877-7
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Track and field
BMC Sports Science, Medicine and Rehabilitation
ISSN: 2052-1847
- General enquiries: [email protected]
Does the SARS-CoV-2 mRNA vaccine and its serum IgG levels affect fertility treatments and obstetric outcomes? An observational cohort study
- Open access
- Published: 23 April 2024
- Volume 24 , article number 81 , ( 2024 )
Cite this article
You have full access to this open access article

- Netanella Danielli Miller 1 , 2 ,
- Nitzan Goren Gepstein 1 , 2 ,
- Dovev Cohen 1 , 2 ,
- Einat Haikin Herzberger 1 , 2 ,
- Hila Shalev Ram 1 , 2 ,
- Jordana Mashiach Friedler 1 , 2 ,
- Maya Sharon Weiner 1 , 2 ,
- Roni Rahav 1 , 2 ,
- Victoria Indenbaum 3 ,
- Yaniv Lustig 3 &
- Amir Wiser 1 , 2
1410 Accesses
311 Altmetric
Explore all metrics
Although there are some data regarding the COVID-19 vaccine and in in vitro fertilization (IVF) treatments, its potential impact in terms of serum immunoglobulin G (IgG) levels has not been evaluated prospectively. This study aimed to assess the effect of COVID-19 vaccine and IgG levels on IVF outcomes.
This observational, cohort study was conducted at a referral IVF unit. Couples undergoing IVF treatment during the COVID-19 vaccination period were recruited from March–April 2021. The study compared 38 women who had received the Pfizer mRNA COVID-19 vaccination to 10 women who had not and were not infected by the virus. We also compared pre- and post-vaccination IVF treatments for 24 women. The relation between serologic titers and IVF treatment outcomes was also assessed.
No significant difference was found between the vaccinated and unvaccinated/uninfected groups regarding the main outcome measures. However, there was a trend toward a higher pregnancy rate for the unvaccinated group (57% vs. 23%, p = 0.078) but no difference in delivery rate ( p = 0.236), gestational week ( p = 0.537) or birth rate ( p = 0.671).
We cautiously state that the COVID-19 mRNA vaccine does not affect fertility outcomes, including fertilization, pregnancy and delivery rates, obstetric outcomes, and semen parameters, regardless of measured IgG levels.
Similar content being viewed by others

COVID-19 infection and vaccine have no impact on in-vitro fertilization (IVF) outcome

Effects of COVID-19 vaccination status, vaccine type, and vaccination interval on IVF pregnancy outcomes in infertile couples

Does mRNA SARS-CoV-2 vaccine influence patients' performance during IVF-ET cycle?
Avoid common mistakes on your manuscript.
The coronavirus disease 2019 (COVID-19) is an ongoing global pandemic caused by the severe acute respiratory syndrome coronavirus (SARS-CoV-2) [ 1 ]. COVID-19 has a high prevalence [ 2 ], long incubation period [ 3 ] and efficient transmission [ 4 ].
Vaccines are the most promising and effective solution for preventing infectious diseases [ 5 ]. At the end of 2020, the FDA issued its first emergency use authorization for the Pfizer mRNA BioNtech COVID-19 vaccine [ 6 , 7 ], with a reported 94%–95% efficacy in preventing COVID-19 [ 8 ]. Other vaccines, such as Moderna (mRNA vaccine) and Janssen followed.
Inactive, toxin-free vaccines are considered safe during pregnancy [ 9 ]. Although animal studies also did not show adverse effects on female reproduction or fetal/embryonal development, the data are still limited [ 10 , 11 ]. Some data regarding the effect of the COVID-19 vaccine on fertility have shown that the vaccine itself may not affect fertility outcomes in terms of the number of oocytes retrieved, blastulation rate and pregnancy rate [ 12 ].
Another study evaluated 36 couples before and after the vaccine and found that the SARS-CoV-2 mRNA vaccine did not affect patient performance or ovarian reserve in their immediate subsequent IVF cycle [ 13 ]. However, it did not include serologic tests to evaluate the vaccination status of the couples. Moreover, few studies have tried to evaluate the effect of the COVID-19 vaccine and the IgG levels on treatment outcomes.
Given this, the current study examined the effect of COVID-19 vaccines on women and men undergoing IVF treatments. We investigated the following: a) differences in IVF treatment outcomes and semen analyses between vaccinated and unvaccinated/uninfected patients, b) differences in treatment outcomes before and after the vaccine among vaccinated patients, and c) correlations between IVF treatment outcomes and humoral response among vaccinated patients.
We believe that understanding the effects of the vaccine allows women and men to receive accurate advice and make informed decisions regarding COVID-19 vaccination and fertility treatments.
Materials and methods
Study design.
This observational cohort study included women and men who were vaccine recipients and those who were neither vaccinated nor infected and were undergoing IVF treatments in a secondary medical center. We conducted serologic tests for all participants to exclude those who were not vaccinated and had been infected unknowingly.
Study population
Couples undergoing IVF treatment during the COVID-19 vaccination period were recruited in March and April 2021. Eligibility criteria were ages 18–45 years and a well-documented COVID-19 vaccination for the vaccinated group. Exclusion criteria included women who did not plan embryo transfer (surrogacy, social or medical fertility preservation). Women with a positive SARS-CoV-2 polymerase chain reaction (PCR) test were also excluded.
Participants who met the eligibility criteria signed an informed consent and blood was drawn for serology. Women who were not vaccinated and had a positive serology test were also excluded. Demographic and fertility information were obtained from the electronic medical records.
Serology assays
Samples from participants were tested with an enzyme-linked immunosorbent assay (ELISA) that detects IgG antibodies against the receptor-binding domain (RBD) of SARS-CoV-2. Titers > 1.1 were defined as positive.
A SARS-CoV-2 pseudo-virus neutralization assay was performed using a propagation–competent–spike [ 14 ], which was kindly provided by Gert Zimmer, University of Bern, Switzerland. Sera unable to reduce viral replication by 50% at a 1–8 dilution or below were considered non-neutralizing. All samples positive for RBD-IgG were tested for neutralization assay. Negative RBD-IgG tests were not tested since these have been shown to yield negative neutralization assay tests.
Fertility-related outcomes of interest included total drug dose for induction, endometrial thickness, number of retrieved oocytes, estradiol and progesterone levels on the day of triggering, the ratio between estradiol on trigger day per retrieved oocyte, fertilization rate, embryo quality, number of blastocysts and clinical pregnancy rate. We also evaluated the semen total motile count (TMC), which is calculated by multiplying volume by concentration (million sperm/ml) by motility (percent moving). Clinical pregnancy was defined as one with a high concentration of human chorionic gonadotrophin and ultrasound confirmation of a gestational sac and was calculated as a percentage from women who had gone through embryo transfer.
The outcomes of vaccinated and unvaccinated/uninfected patients were compared. The latest cycle for the unvaccinated and the cycle at least one week post-vaccination were included. We confirmed that the treatment was at least one week after vaccination, as antibody levels are detectable at least 7 days after the second vaccination [ 15 ].
For vaccinated patients, treatment outcomes were compared between the most recent treatments before and after the vaccine. In addition, the associations between serologic IgG levels and neutralizing levels and fertility outcomes were evaluated. Also defined was a group of women with high IgG antibody levels (cut-off defined as the level above the median of IgG antibodies of the vaccinated group) who were compared to patients with low IGG levels.
Statistical analysis
Data were analyzed using SPSS 24.0 for Windows (IBM Corp., Armonk, NY). Discrete variables are presented as numbers and percentages, and continuous variables as means and standard deviations (SD). We calculated p values using t test or chi-squared for continuous and categorical variables, respectively. Pearson’s coefficients were calculated between relevant variables. Multivariate regression was conducted to evaluate variables affecting the number of oocytes retrieved, fertilization rate and pregnancy rate. To compare pre- and post-vaccination, we used a paired t test. For all tests, a p value < 0.05 was considered significant.
The cohort included 52 women and 21 men. Among the women, 40 were vaccinated (77%) and 12 were not (23%). Of the men, 7 were vaccinated (33%) and 14 were not (67%). After serology testing, 2 women (17%) and 2 men (14%) in the unvaccinated group were found to have positive serology and were excluded from the analysis. In the vaccinated group, 2 women whose treatment started less than a week after the second vaccine were also excluded. Figure 1 presents a flow diagram of cases included in the study.

Flow diagram of cases included in the study
Comparison between vaccinated and unvaccinated/uninfected
The cohort included 38 vaccinated women and 10 who were not vaccinated or infected. Table 1 shows the basic characteristics and the fertility outcomes between groups. No differences in BMI ( p = 0.108) or marital status were found ( p = 0.198). There was a trend toward older age among the women in the vaccinated group compared to the non-vaccinated (38 ± 4.4 years vs. 35 ± 5.8 years, p = 0.083). No significant differences were found between groups regarding total drug dose for induction, endometrial thickness, number of retrieved oocytes, estradiol and progesterone levels on the triggering day, ratio between estradiol on triggering day per retrieved oocyte, fertilization rate, or embryo quality (Table 1 ). There was a trend toward higher pregnancy rate for the unvaccinated group (57% vs. 23%, p = 0.078). However, multivariable logistic regression for pregnancy rate showed no differences regarding fertilization rates ( p = 0.842) or pregnancy rates ( p = 0.414) between vaccinated and unvaccinated women. No difference was found between groups in terms of missed abortion rate ( p = 0.125) and delivery rate ( p = 0.236). Additionally, regarding obstetric outcomes, we did not find any significant differences in gestational week ( p = 0.537) or birth weight percentile ( p = 0.671; Table 2 ).
Semen analysis did not find any differences in the TMC between men who were vaccinated and those who were not ( p = 0.711; Table 2 ).
Comparison between pre- and post-vaccination treatment outcomes
Data regarding pre- and post-vaccine treatment were available for 24 of the 40 vaccinated patients. The mean interval between ovum pick-up cycles and the second vaccination was 33 days (range 11–69 days).
Data regarding the IVF outcomes before and after the SARS-CoV-2 mRNA vaccine are shown in Table 3 . No significant differences were found regarding total drug dose for induction, endometrial thickness, number of retrieved oocytes, estradiol and progesterone on the day of triggering, the ratio between estradiol on trigger day per retrieved oocyte, fertilization rate, embryo quality, number of blastocysts and clinical pregnancy rate.
Correlation between serum IGG levels and fertility outcomes
All 40 vaccinated patients were found to have neutralizing antibodies (above 16), defined as a positive vaccination status [ 14 ].
The only positive correlation found was between neutralization titer and progesterone level on the day of induction (Pearson = 0.787, p = 0.001; Fig. 1 ). We also conducted a secondary analysis of women with high vs. low IGG levels. No difference was found regarding any of the measured fertility outcomes (data not shown).
Reluctance of women and men of fertility age to receive a new vaccine is common, especially due to uncertainty regarding its possible long-term effects and when a new vaccine, such as the mRNA COVID-19, is produced and approved emergently [ 16 ]. Yet, lack of knowledge or misleading information may cause uncertainty. Thus, it is essential to evaluate the safety of the COVID-19 mRNA vaccine regarding fertility and sterility.
The current study did not find any differences in fertility treatment or obstetric outcomes between women who were vaccinated and those who were not. In addition, no differences were found among patients before and after receiving the vaccine.
Our results support those of Bentov et al. who showed that neither COVID-19 infection, the BNT162b2 mRNA vaccine, nor the immune response, resulted in any measurable detrimental effects on IVF treatment and outcome parameters [ 17 ]. Moreover, Orvieto et al. showed that the mRNA SARS-CoV-2 vaccine did not affect patient performance or ovarian reserve in the immediate, subsequent IVF cycle [ 13 ]. Aharon et al. reported similar results [ 12 ]. However, it is important to mention that the authors did not conduct serology tests to exclude unvaccinated patients who might have been exposed to the virus.
A study of frozen embryo transfer cycles compared implantation rates among women who were SARS-CoV-2 vaccine seropositive, infection seropositive or seronegative. No difference was found in serum-documented hCG implantation rates or sustained implantation rates among the 3 groups [ 18 ]. We also evaluated pregnancy rates between vaccinated and unvaccinated/uninfected patients. Although we found a trend toward a higher pregnancy rate, this was not sustained in multivariant regression.
The lack of negative effects of the vaccine may be related to its biological activity, as it is composed of nucleoside-modified RNA (modRNA) [ 19 ] encoding the SARS-CoV-2 full-length spike, modified by two proline mutations. mRNA-based therapy avoids deleterious side effects (which include integration into chromosomes) that limit clinical application of most virus- and DNA-based vectors [ 20 ]. Other mRNA-based vaccines that have been investigated primarily with animals, including influenza A virus [ 21 ], rabies virus [ 22 ], HIV-1 [ 23 ], and Ebola virus [ 24 ], also showed efficacy of the mRNA vaccines combined with safety data.
The current study found no differences between semen analysis among vaccinated and unvaccinated men. Orvietto et al. also did not find any differences in semen volume, sperm concentration, sperm %, and pre-wash TMC, based on vaccine status [ 13 ]. This may be explained by the biological activity of the vaccine, as mentioned above [ 20 ]. In addition, spermatogenesis takes 74 days and another 12–21 days to be transported through the epididymis to the ejaculatory ducts [ 25 ]. Thus, the specific semen analysis examined may have represented sperm parameters before exposure to the vaccine.
This study supports the approach of major professional associations. The most recent SRM, ACOG and SMFM Joint Statement notes that medical experts continue to assert that COVID-19 vaccines do not affect fertility [ 26 ].
When evaluating IgG serology titers, the only effect on fertility outcomes that we found was a positive relation between progesterone levels on the day of triggering and IgG titer. Bentov et al. also found that serum progesterone was lower in the non-exposed group compared to the exposed group [ 17 ]. Progesterone is known to be involved in the immune response. Progesterone receptors are expressed in most immune cells, including epithelial cells, macrophages, dendrites, lymphocytes, mast cells, and eosinophils, and help modulate the immune response to pathogens [ 27 ]. Moreover, women are known to have higher levels of estrogen and progesterone, which have been shown to modulate a more robust immune response [ 27 ]. During the COVID-19 pandemic, this study suggested giving hormone replacement therapy, including estrogen and progesterone, to older patients based on the evidence that sex hormone levels can influence immune system function [ 28 ]. Accordingly, it may be suggested that the higher immune response in some women may have triggered activation of progesterone as an immune system modulator. Further studies are needed to evaluate this issue.
The strengths of this study relate to the prospective evaluation of the important question regarding whether mRNA COVID-19 vaccination affects fertility treatments. Evaluation of the serologic titer was also very important. Moreover, we evaluated treatment measures, pregnancy and obstetric outcomes and semen analyses. It was also important that we evaluated the serologic status of each patient to exclude exposed, unvaccinated patients; rendering our analyses more accurate and precise. Therefore, to avoid selection bias, it was essential to exclude these individuals when analyzing the unvaccinated population. However, this study was limited by its relatively small sample size. In addition, it is essential to evaluate long-term pregnancy outcomes, congenital malformations. Future, larger studies will be needed to validate our observations and to maintain longer follow-up of these patients.
Conclusions
We cautiously state that the COVID-19 mRNA vaccine does not affect fertility outcomes, including fertilization, pregnancy and delivery rates, obstetric outcomes, and semen parameters, regardless of the IgG levels. Moreover, no relation to IgG titers and fertility outcomes was found, except for higher progesterone levels on triggering day. Larger, prospective studies are needed to validate these observations.
Data availability
The data presented in this study are available upon request from the corresponding author. The data are not publicly available due to privacy limitations.
Di Gennaro F, Pizzol D, Marotta C, Antunes VR, Veronese NSL. Coronavirus diseases (COVID-19) current status and future perspectives: a narrative review. Int J Env Res Public Heal. 2020;17(8):2690. https://doi.org/10.3390/ijerph17082690 .
Article CAS Google Scholar
World Health Organization (WHO). Coronavirus disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. 2021.
Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med [Internet]. 2020;382(13):1199–207. https://doi.org/10.1056/NEJMoa2001316 .
Article CAS PubMed Google Scholar
Klompas M, Baker MA, Rhee C. Airborne transmission of SARS-CoV-2: theoretical considerations and available evidence. JAMA. 2020. https://doi.org/10.1001/jama.2020.12458 .
Article PubMed PubMed Central Google Scholar
Van Panhuis WG, Grefenstette J, Jung SY, Chok NS, Cross A, Eng H, et al. Contagious diseases in the United States from 1888 to the present. N Engl J Med [Internet]. 2013;369(22):2152–8. https://doi.org/10.1056/NEJMms1215400 .
FDA. USF and DA. “FDA Takes Key Action in Fight Against COVID-19 By Issuing Emergency Use Authorization for First COVID-19 Vaccine.” 2020; Available at: https://www.fda.gov/news-events/press-announcements/fda-takes-key-action-fight-against-covid-19-issuing-emergency-use-authorization-first-covid-19 .
Skowronski DM, De Serres G. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med [Internet]. 2021;384(16):1576–7. https://doi.org/10.1056/NEJMc2036242 .
Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med. 2020;383(27):2603–15. https://doi.org/10.1056/NEJMoa2034577 .
Maertens K, Orije MRP, Van Damme P, Leuridan E. Vaccination during pregnancy: current and possible future recommendations. Eur J Pediatr [Internet]. 2020;179(2):235–42. https://doi.org/10.1007/s00431-019-03563-w .
Article PubMed Google Scholar
Michailidou A, Trenz H-J, de Wilde P. Covid 19 vaccine Astrazeneca report. Internet Eur Integr. 2019;167–72.
Michailidou A, Trenz H-J, de Wilde P. Pfizer vaccination product information. Internet Eur Integr. 2019;167–72.
Aharon D, Lederman M, Ghofranian A, Hernandez-Nieto C, Canon C, Hanley W, Gounko D, et al. In vitro fertilization and early pregnancy outcomes after coronavirus disease 2019 (COVID-19) vaccination. Obstet Gynecol. 2022;139(4):490–7. https://doi.org/10.1097/AOG.0000000000004713 .
Orvieto R, Noach-Hirsh M, Segev-Zahav A, Haas J, Nahum R, Aizer A. Does mRNA SARS-CoV-2 vaccine influence patients’ performance during IVF-ET cycle? Reprod Biol Endocrinol. 2021;19(1):69. https://doi.org/10.1186/s12958-021-00757-6 .
Article CAS PubMed PubMed Central Google Scholar
Lustig Y, Sapir E, Regev-Yochay G, Cohen C, Fluss R, Olmer L, et al. BNT162b2 COVID-19 vaccine and correlates of humoral immune responses and dynamics: a prospective, single-centre, longitudinal cohort study in health-care workers. Lancet Respir Med. 2021;9(9):999–1009. https://doi.org/10.1016/S2213-2600(21)00220-4 .
Arunachalam PS, Scott MK, Hagan T, Li C, Feng Y, Wimmers F, Grigoryan L, Trisal M, Edara VV, Lai L, Chang SE. Systems biological assessment of human immunity to BNT162b2 mRNA vaccination. Res Square. 2021. https://doi.org/10.21203/rs.3.rs-438662/v15 .
Article Google Scholar
Lu-Culligan A, Iwasaki A. The false rumors about vaccines that are scaring women. The New York Times. Available at: https://www.nytimes.com/2021/01/26/opinion/covid-vaccine-rumors.html .
Bentov Y, Beharier O, Moav-Zafrir A, Kabessa M, Godin M, Greenfield CS, et al. Ovarian follicular function is not altered by SARS-CoV-2 infection or BNT162b2 mRNA Covid-19 vaccination. Hum Reprod. 2021;36(9):2506–13. https://doi.org/10.1093/humrep/deab182 .
Morris RS. SARS-CoV-2 spike protein seropositivity from vaccination or infection does not cause sterility. F&S Rep. 2021. https://doi.org/10.1016/j.xfre.2021.05.010 .
Karikó K, Muramatsu H, Welsh FA, Ludwig J, Kato H, Akira S, et al. Incorporation of pseudouridine into mRNA yields superior nonimmunogenic vector with increased translational capacity and biological stability. Mol Ther [Internet]. 2008;16(11):1833–40. https://doi.org/10.1038/mt.2008.200 .
Hacein-Bey-Abina S, Von Kalle C, Schmidt M, McCormack MP, Wulffraat N, Leboulch P, et al. LMO2-associated clonal T cell proliferation in two patients after gene therapy for SCID-X1. Sci [Internet]. 2003;302(5644):415–9. https://doi.org/10.1126/science.1088547 .
Bahl K, Senn JJ, Yuzhakov O, Bulychev A, Brito LA, Hassett KJ, et al. Preclinical and clinical demonstration of immunogenicity by mRNA vaccines against H10N8 and H7N9 influenza viruses. Mol Ther [Internet]. 2017;25(6):1316–27. https://doi.org/10.1016/j.ymthe.2017.03.035 .
Schnee M, Vogel AB, Voss D, Petsch B, Baumhof P, Kramps T, et al. An mRNA vaccine encoding rabies virus glycoprotein induces protection against lethal infection in mice and correlates of protection in adult and newborn pigs. PLoS Negl Trop Dis [Internet]. 2016;10(6): e0004746. https://doi.org/10.1371/journal.pntd.0004746 .
Pardi N, Secreto AJ, Shan X, Debonera F, Glover J, Yi Y, et al. Administration of nucleoside-modified mRNA encoding broadly neutralizing antibody protects humanized mice from HIV-1 challenge. Nat Commun [Internet]. 2017;8:14630. https://doi.org/10.1038/ncomms14630 .
Meyer M, Huang E, Yuzhakov O, Ramanathan P, Ciaramella G, Bukreyev A. Modified mRNA-based vaccines elicit robust immune responses and protect guinea pigs from Ebola virus disease. J Infect Dis [Internet]. 2018;217(3):451–5. https://doi.org/10.1093/infdis/jix592 .
Jung A, Schuppe H-C. Influence of genital heat stress on semen quality in humans. Andrologia. 2007;39(6):203–15. https://doi.org/10.1111/j.1439-0272.2007.00794.x .
COVID-19 Vaccination Considerations for Obstetric–Gynecologic Care. ACOG July 2021.
Mauvais-Jarvis F, Klein SL, Levin ER. Estradiol, progesterone, immunomodulation, and COVID-19 outcomes. Endocrinology. 2020;161(9):bqaa127.
Okpechi SC, Fong JT, Gill SS, Harman JC, Nguyen TH, Chukwurah QC, et al. Global sex disparity of COVID-19: a descriptive review of sex hormones and consideration for the potential therapeutic use of hormone replacement therapy in older adults. Aging Dis [Internet]. 2021;12(2):671–83. https://doi.org/10.14336/AD.2020.1211 .
Download references
Acknowledgements
Not applicable.
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Author information
Authors and affiliations.
IVF Unit, Department of Obstetrics and Gynecology, Meir Medical Center, 4428164, Kfar Saba, Israel
Netanella Danielli Miller, Nitzan Goren Gepstein, Dovev Cohen, Einat Haikin Herzberger, Hila Shalev Ram, Jordana Mashiach Friedler, Maya Sharon Weiner, Roni Rahav & Amir Wiser
School of Medicine, Tel Aviv University, Tel Aviv, Israel
Central Virology Laboratory, Public Health Services, Ministry of Health, Chaim Sheba Medical Center, Tel Aviv, Israel
Victoria Indenbaum & Yaniv Lustig
You can also search for this author in PubMed Google Scholar
Contributions
NDM initiated the study, recruited participants, analyzed the data, and wrote the final version of the article. YGG, DC, EHH, JMF, MSW, and RR recruited participants, and coded the data. AA, HSR, and OM recruited participants and wrote the article. VI and YL conducted the laboratory analyses. AW initiated the study, recruited participants, analyzed the data, and wrote the final version of the article. All authors read and approved the final manuscript.
Corresponding author
Correspondence to Netanella Danielli Miller .
Ethics declarations
Conflict of interest.
The authors have no relevant financial or non-financial interests to disclose.
Ethical approval
The study was performed in accordance with the principles of the Declaration of Helsinki. Approval was granted by the Meir Medical Center Ethics Review Board, approval number MMC-0017–21.
Consent to participate
All participants provided signed informed consent.
Consent for publication
Additional information, publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Miller, N.D., Goren Gepstein, N., Cohen, D. et al. Does the SARS-CoV-2 mRNA vaccine and its serum IgG levels affect fertility treatments and obstetric outcomes? An observational cohort study. Clin Exp Med 24 , 81 (2024). https://doi.org/10.1007/s10238-024-01345-9
Download citation
Received : 11 December 2023
Accepted : 02 April 2024
Published : 23 April 2024
DOI : https://doi.org/10.1007/s10238-024-01345-9
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- mRNA COVID-19 vaccine
- Corona virus
- In vitro fertilization
- Find a journal
- Publish with us
- Track your research
- Open access
- Published: 24 April 2024
Trends and regional differences in antidiabetic medication use: a nationwide retrospective observational study
- Márta Csatordai 1 , 2 ,
- Ria Benkő 1 , 2 ,
- Mária Matuz 1 , 2 ,
- Zsófia Engi 1 ,
- Dezső Csupor 1 ,
- Csaba Lengyel 3 &
- Péter Doró 1
Diabetology & Metabolic Syndrome volume 16 , Article number: 88 ( 2024 ) Cite this article
100 Accesses
1 Altmetric
Metrics details
The prevalence of diabetes is increasing, and several new drug groups have been authorized and used successfully in the treatment of diabetes, while older drug groups are still in use. Our aim was to assess the utilization tendencies and regional differences in antidiabetic medication consumption in Hungary between 2015 and 2021 and to identify the possible determinants of regional differences in antidiabetic medication use.
For this retrospective drug utilization study, yearly wholesale database was used, which provides total coverage for ambulatory antidiabetic drug sales in Hungary, including both reimbursed and non-reimbursed medications. Data were expressed as Defined Daily Dose per 1000 inhabitants per day (DDD/TID), percentage of total use and the ratio of the highest and lowest utilization values among the counties (max/min ratio). To assess the potential reasons for regional differences in antidiabetic drug use, we analyzed the associations between regional drug utilization data and possible determinants.
The total national antidiabetic medication use has increased by 7.6% and reached 94.8 DDD/TID in 2021. Regarding antidiabetic subgroups, the use of metformin and novel antidiabetics (DPP4Is, GLP1As and SGLT2Is) and their combinations increased in all counties, while sulfonylurea consumption decreased, and insulin use was stable. In 2021, 19.2–24.1% of the total antidiabetic medication consumption was novel antidiabetics, 39.1–47.2% metformin, 14.8–25.8% sulfonylureas and 23.6–30.5% were insulins. Regional differences in antidiabetic medication consumption were considerable mainly in the case of GLP1As (max/min ratio:3.00), sulfonylureas (2.03) and SGLT2Is (1.92) in 2021. The association between antidiabetic medication use and possible determinants was confirmed in the case of unemployment rate and sulfonylurea use, the number of public medical card holders per ten thousand inhabitants and human insulin and sulfonylurea use. GLP1As were the only antidiabetic drug group that did not correlate with any of the investigated factors.
Conclusions
Although novel antidiabetic drug use was growing dynamically in Hungary, sulfonylurea use is still considerable. Differences in antidiabetic drug consumption were substantial between the regions.
Introduction
Diabetes is a chronic disease affecting an increasing number of people worldwide. According to the International Diabetes Federation Diabetes Atlas 2021, 537 million adults aged 20 to 79 years (10.5% of the population) had diabetes worldwide, and by 2045, this number will reach 783 million (12.2% of the expected population) [ 1 ]. In Hungary, 14.2% of adults (aged 19 and older) registered with general practitioners had diabetes in 2021, according to the database of the Hungarian Central Statistical Office [ 2 ]. The alarming rate of diabetic patients has led to intensive pharmacological research, and therapeutic approaches for diabetes have changed considerably in recent decades [ 3 ]. Novel drug groups, namely, dipeptidyl peptidase 4 inhibitors (DPP4Is), glucagon-like peptide-1 analogues (GLP1As) and sodium-glucose co-transporter 2 inhibitors (SGLT2Is), were developed and included in the therapeutic guidelines. Although metformin remains the first choice in the treatment of type 2 diabetes, GLP1As and SGLT2Is have become preferred agents in adults with type 2 diabetes with an established/high risk of atherosclerotic cardiovascular disease or chronic kidney disease [ 3 , 4 , 5 , 6 ]. According to the American Diabetes Association-European Association for the Study of Diabetes Consensus Report, diabetes therapy should be individualized, and clinicians should consider patient-specific factors and social determinants that affect treatment choice, such as impact on weight, cardiorenal protection, side effects (e.g., hypoglycemia), complexity of regimen, cost and availability of medication, age, education, and mental status [ 7 ]. Taking into consideration the variety of these factors, the regional differences in diabetes prevalence, and the high number of antidiabetic medications, antidiabetic therapy may vary over a wide range, both at the patient and at regional levels. These differences can be quantitative and qualitative.
Previously published data on the utilization of antidiabetic medicines in Italy and Portugal revealed substantial regional differences [ 8 , 9 ]. Regional differences in medication use can be associated with several factors. Beyond the previously mentioned patient-specific factors, social determinants, disease prevalence, regional differences in health policies, differences in accessibility to healthcare and the characteristics of prescribing doctors may also influence regional differences [ 10 ]. Identifying regional differences in the utilization of medicines can be useful for developing national action plans to improve treatment strategies, optimize the allocation of healthcare resources, and consequently improve the health outcomes of diabetic patients.
Although previous studies have investigated reimbursed antidiabetic drug utilization in Hungary both at the national and patient levels, complete utilization (including both reimbursed and non-reimbursed medications) of this medication group and regional utilization differences and their possible determinants have not yet been investigated [ 11 , 12 ].
Our aim was to assess the utilization tendencies and regional differences in antidiabetic medication consumption in Hungary between 2015 and 2021, and to identify the possible determinants of regional differences in antidiabetic medication use.
For the retrospective drug utilization study, yearly wholesale data on antidiabetic drugs were kindly provided by IQVIA for each Hungarian county (19 counties and capital, covering the total Hungarian population of nearly 10 million people) for the period between 2015 and 2021. IQVIA is a multinational company, that provides clinical research services for life science research, including data on drug utilization. The database covers the total ambulatory drug sales in Hungary, including both reimbursed and non-reimbursed medications. The database contains aggregated sales data at the product level: year, region where the drug was purchased, anatomical therapeutic chemical classification code (ATC) of the active ingredient, name of the product, number of boxes and number of defined daily doses (DDDs) of each product per year per county. DDD is the average daily maintenance dose of a medication when used in adults in its main indication [ 13 ].
Data were analyzed using the WHO ATC/DDD system (version 2022), and the filtered ATC code was A10, which is drugs used in diabetes. Regional consumption data were expressed as defined daily dose per 1000 inhabitants per day (DDD/TID), and relative use was expressed as the percentage of total antidiabetic medication use [ 13 , 14 ]. The following formula was used to calculate DDD/TID: (total number of DDDs used in 1 year x 1000) / (population x 365). DDD/TID is a standardized technical unit that helps to compare drug utilization across different populations [ 14 ]. When analyzing the utilization of each pharmacological subgroup, monocomponent products and combination products were added together to provide the results of the overall use of each active ingredient and each pharmacological subgroup. Consequently, the combination products were considered in both relevant pharmacological subgroups (Suppl. 2 ). However, when calculating the overall use of antidiabetic medication, the combination products were included only once, avoiding the addition of the same product twice.
To show the extent of regional utilization differences, the ratio of the highest and lowest utilization values among the counties was calculated (max/min ratio). To analyze time trends in the use of antidiabetic drug groups, simple linear regression was applied and described with the regression coefficient and significance (p value) of the coefficient. Statistical significance was set at P < 0.05. The dependent variable was the use of antidiabetic drug groups (expressed as DDD/TID), and the independent variables was time (years). The regression coefficient describes trends and shows the average annual changes, while positive coefficients indicate increasing trends, and negative coefficients indicate decreasing trends.
To assess the potential reasons for regional differences in antidiabetic drug use, we analyzed associations between regional drug utilization data for the year 2021 and possible determinants. Demographic data and possible determinants of antidiabetic drug use were extracted from the Hungarian Central Statistical Office database and the National Health Insurance Fund of Hungary report on the World Diabetes Day if relevant regional data were available [ 15 , 16 ]. These extracted determinants were as follows: unemployment rate, number of public medical card holders per ten thousand inhabitants (type of financial support to reduce medical expenses for socially disadvantaged people as they can obtain specific medicine free of charge up to a monthly maximum limit), regional prevalence of diabetes, percentage of the 60 years and older among the total population, and number of attendances in diabetologic outpatient service (diabetologists) per thousand inhabitants.
Correlations were assessed using the Spearman’s rank test. Microsoft Excel (Microsoft Office, 2010, Microsoft Corp., Redmond, WA, USA), R (version 3.6.0, R Foundation for Statistical Computing Vienna, Austria) and Datawrapper (Datawrapper GmbH, Berlin, Germany) were used for data analysis and plotting.
Regarding the reimbursement system in Hungary, the National Health Insurance Fund is the sole mandatory national health insurance company. In our study, all antidiabetic active ingredients were reimbursed, but not necessarily every product. GPs can prescribe all antidiabetic medications, but in the case of insulins, GLP1As, SGLT2Is and DPP4Is for the reimbursement, regular diabetologist recommendations and follow-ups are necessary [ 17 ].
Ethical approval was not required because wholesale drug utilization data were aggregated and not linked to any patient data.
During the study period, both national and regional antidiabetic medication use showed a growing tendency, but to different extent. The total national antidiabetic medication use increased by 7.6% and reached 94.8 DDD/TID in 2021, however, in 2020, there was a peak of 97.4 DDD/TID. In most of the counties the rise in total antidiabetic consumption was considerable between 4.5% and 16.5% over the 7 years, except in the capital (Budapest) and in Győr-Moson-Sopron County (in the northwestern part of the country). The highest antidiabetic medication utilization in 2021 and the highest increase in use during the study period were observed in Békés County (in the southeastern part of the country) (Table 1 ). The difference in antidiabetic medication use between counties was relatively stable, the max/min ratio was between 1.37 and 1.41 during the study period and south-southwest counties tended to use more antidiabetics.
Regarding the use of antidiabetic subgroups, large and stable interregional differences were observed. During the study period, both insulin use and interregional differences in insulin use were stable (max/min ratio: 1.65–1.70) without a clear geographical gradient (Table 1 .). In 2021, insulin use was 23.6–30.5% of total antidiabetic medication consumption. In contrast to insulin utilization, metformin and sulfonylurea use showed dynamic alterations. The utilization of metformin and its combinations showed an emerging trend in all counties and reached 39.1–47.2% of the total antidiabetic medication use at the end of the study period, which means that metformin and its combinations were the most frequently used antidiabetic medications (Table 1 ). The south-southwest counties tended to use more metformin than the northeast counties, but the interregional differences in metformin use were the smallest among all antidiabetic drug groups (max/min ratio: 1.46 in 2021, ranging between 1.46 and 1.52). Although sulfonylurea use decreased in all counties during the study period, notable differences were observed in regional consumption (Table 1 ). While the use of sulfonylureas was the lowest in Budapest, with 14.8 DDD/TID in 2021, the use of this drug group was the highest in Békés County, with 30.1 DDD/TID (max/min ratio of 2.03). The relative use of sulfonylureas in different regions was still between 14.8% and 25.8% of the total antidiabetic medication consumption in 2021.
The use of novel antidiabetic drug groups, namely, DPP4Is, SGLT2Is and GLP1As and their combinations, showed an emerging tendency. The use of DPP4Is was the highest among these drug groups, but after dynamic growth between 2015 and 2020, its use decreased slightly and, in some counties, SGLT2I utilization exceeded DPP4I use by 2021 (Table 1 , Suppl. 1 ). DPP4Is, SGLT2Is, GLP1As, and their combinations accounted for 19.2–24.1% of the total use of antidiabetic drugs in Hungary in 2021. Regarding interregional differences, GLP1A use showed the highest difference among the antidiabetic drug groups in 2021 (max/min ratio: 3.00). GLP1A utilization was the highest in the western regions, mainly in the southwest (Southern Transdanubia), whereas utilization was much lower in the east, mainly in the northern regions of Hungary and the Northern Great Plain (Table 1 ; Fig. 1 ). SGLT2I use tended to be higher in the southern counties, while in the northern counties, the utilization was much lower, with a max/min ratio of 1.92 in 2021 (Table 1 ). In the case of DPP4Is, the difference between the regions was lower than that of the other two drug groups; the max/min ratio was 1.70 in 2021, and a clear geographical gradient was not observed.

Regional differences in the use of glucagon-like peptide-1 analogues and their combinations in 2021 (expressed in DDD/TID)
The utilization of these antidiabetic subgroups expressed in DDD/TID is summarized in Table 1 , and the regional utilization tendencies of different antidiabetic groups are shown in Suppl. 1 . The changes in the regional differences in the utilization of antidiabetic drug groups between 2015 and 2021 are shown in Fig. 2 .

Change in regional antidiabetic drug group utilization between 2015 and 2021. Red square and lines: county average ± 95% CI; Yellow circle: county utilization data. A10: Antidiabetics total, A10A: Insulins, A10BA+: Biguanides and combinations, A10BB: Sulfonylureas, A10BD: Combinations of antidiabetics, A10BF: Alpha glucosidase inhibitors, A10BG+: Thiazolidindiones and combinations, A10BH+: dipeptidyl peptidase 4 inhibitors and combinations, A10BJ+: glucagon-like peptide-1 analogues and combinations, A10BK+: sodium-glucose co-transporter 2 inhibitors and combinations, A10BX: Glinides
The use of alpha glucosidase inhibitors, thiazolidinediones and glinides constantly decreased and were 0.07 DDD/TID, 0.04 DDD/TID and 0.03 DDD/TID in 2021, which was marginal compared to other antidiabetic subgroups. Therefore, these drug groups were not included in the tables and correlation analysis was not performed on these data.
Regarding antidiabetic medication use and possible determinants, total antidiabetic medication use and almost all investigated drug subgroups correlated positively with the percentage of those 60 years and older among the total population and the number of attendances in diabetologic outpatient services per thousand inhabitants, except for GLP1As and human insulins. The unemployment rate was correlated only with sulfonylurea use, and the number of public medical card holders per ten thousand inhabitants was correlated only with human insulin and sulfonylurea use. The regional prevalence of diabetes did not correlate with the use of any of the investigated drug groups. GLP1As were the only antidiabetic drug group that did not correlate with any of the investigated factors. The associations between antidiabetic medication use and possible determinants are presented in Table 2 .
This is the first study to analyze antidiabetic drug utilization in Hungary, including not only reimbursed but also non-reimbursed antidiabetics. It is also the first study to analyze antidiabetic medication use and its determinants at the regional level in Hungary. In recent years, substantial novelties in diabetes therapy and therapeutic protocols impacted antidiabetic medication utilization patterns [ 11 ]. This retrospective drug utilization study confirmed that antidiabetic medication use has changed remarkably between 2015 and 2021 in Hungary.
In all Hungarian counties, total antidiabetic use emerged, but with an interesting peak in 2020. This utilization peak coincided with the coronavirus disease-19 outbreak when the Hungarian population tended to stock their chronic medications. This stockpiling effect was also observed in the medication utilization data of other nations [ 18 ].
Regarding antidiabetic subgroups, metformin was the most commonly used antidiabetic alone or in fixed-combination with other antidiabetic drugs (DPP4Is and SGLT2Is) during the entire study period. This was explained by the Hungarian guidelines where metformin is the first drugs of choice alone or in combination if the patients are newly diagnosed with type 2 diabetes and do not have HbA1c above 9% with catabolic symptoms [ 5 ]. The high rate of metformin use is similarly observed in Denmark, where metformin use was 39% of the total antidiabetic use in 2021 [ 19 ]. Sulfonylureas are still included in Hungarian and international therapeutic guidelines but not as preferred agents due to their side effects, such as hypoglycemia and weight gain, and furthermore, this drug group does not decrease the risk of major cardiovascular events [ 4 , 5 , 7 ]. Although sulfonylurea use has decreased continuously, its share of total antidiabetic medication use was still remarkable in Hungary. The utilization of sulfonylureas has shown high differences among some European countries. In Hungary the share of sulfonylurea use at the national level was 19.2% in 2021; in Denmark, it was only 3.6% in 2021, while in Romania, the sulfonylurea use was estimated to be 27.9% of the total antidiabetic medication use in 2019 [ 19 , 20 ]. Despite the growing prevalence of diabetes, insulin use remained relatively stable, while the utilization of newer antidiabetics, mainly SGLT2Is and GLP1As, has emerged dynamically. The use of newer antidiabetic groups may delay the initiation of insulin therapy in type 2 diabetes, because the availability of these drug groups provides a wider choice for clinicians before considering insulin therapy [ 21 ]. Additionally, while SGLT2Is and GLP1As have positive cardiovascular and renal effects, insulin has a neutral effect in this respect, but has a high risk of hypoglycemia and weight gain [ 4 , 5 , 7 ]. The emerging tendency of SGLT2I and GLP1A use and the change in the use of DPP4I in 2021 is partly due to the different place of these drug groups in therapeutic guidelines. Currently, GLP1As and SGLT2Is are preferred agents in cases of established/high risk of atherosclerotic cardiovascular disease or chronic kidney disease [ 4 , 22 ]. In addition, SGLT2Is are preferred in cases of established/high risk of heart failure and GLP1As are preferred if the main goal is weight management above glycemic targets [ 4 , 22 ]. DPP4Is have neutral effects on weight and cardiovascular and renal problems with moderate effect on blood glucose control, and their use is preferred if the main goal is to improve glucose control without hypoglycemia in the case of elder, frail people [ 3 , 4 ]. The emerging use of DPP4Is, SGLT2Is and GLP1As use has also been observed in other countries’ utilization data, such as Denmark or Portugal [ 9 , 19 ].
Regarding interregional differences, we found stable and considerable variability in the use of antidiabetics which has not been previously studied. Regional differences in total antidiabetic use remained stable and low, in contrast with some antidiabetic subgroups. Insulin use and its regional differences were relatively stable in all counties, and we did not find a geographical gradient in the utilization pattern or association with regional diabetes prevalence. Although insulin use did not correlate with the unemployment rate, an association was found between insulin use and the number of public medical card holders per ten thousand inhabitants. The initiation of insulin therapy is not a financial issue, because human insulin preparations are available with 100% reimbursement (with only minimal patient co-payment of approx. 0.8 EUR/box), so the patient’s financial situation has no influence on receiving insulin therapy [ 17 ]. However, if patients with type 2 diabetes need to receive insulin analogues that are more expensive, these preparations are available with 50% or 100% reimbursement coverage depending on the patients’ HbA1c levels [ 17 , 23 ]. Therefore, patients with a poorer financial situation are more likely to receive human insulin therapy than the more expensive insulin analogues. This is supported by the positive association between human insulin use and the number of public medical card holders. The positive correlation between insulin use and the number of attendances in diabetologic outpatient service per thousand inhabitants may be explained by the fact that insulin can be prescribed with reimbursement only under regular diabetologist supervision [ 17 ]. The positive correlation between insulin use and percentage of people with age 60 years or older can be explained by the fact that older people are more likely to have diabetes for a longer period of time, therefore, their diabetes is more likely to have progressed to the stage where insulin therapy is necessary to be initiated.
In the case of metformin, the relatively low difference in use among counties and the lack of associations with socioeconomic factors may be explained by the high use of metformin in all counties because of therapeutic recommendations, and its affordability and availability. Metformin alone is relatively inexpensive and therefore does not impose a high financial burden on patients, and GPs can prescribe these agents without regular supervision by diabetologists [ 17 ]. Other fixed-dose preparations, mainly with DPP4Is and SGLT2Is are available with 70% reimbursement, but only under regular diabetologist supervision [ 17 ].
In addition to the considerable utilization of sulphonylureas, we found high differences among counties. The high use of sulfonylureas in Hungary can be explained by some factors. Sulfonylureas are inexpensive agents, especially in contrast to newer drug groups, such as GLP1As, which are the most expensive antidiabetic drug group. In Hungary, the full price of sulfonylurea is approximately 0.06–0.14 EUR/DDD and available with 55% reimbursement. Although GLP1As are available with 70% reimbursement coverage, their full price is much higher, approximately 2.12–4.72 EUR/DDD. Additionally, sulfonylureas, similar to metformin, are easily accessible because GPs can prescribe these drugs, while other drug groups (e.g. novel antidiabetic drug groups) can be prescribed with reimbursement only under regular diabetologists’ supervision [ 17 ]. This seemed to be confirmed by the positive associations with some socioeconomic factors such as unemployment rate, the number of public medical card holders per ten thousand inhabitants and percentage of the 60 years and older among the total population.
Regarding DPP4I use, although the max/min difference between regions was 1.70 in 2021, a notable regional pattern and association with socioeconomic factors could not be detected. Higher interregional differences were found in the case of SGLT2Is, and higher use was observed in the southern counties; however, we did not find any relevant socioeconomic factors that explains these differences. The utilization of GLP1As showed the largest interregional differences among antidiabetics (max/min ratio 3.00 in 2021). We did not find any socioeconomic factors that explained the detected southwest-northeast gradient. Although we did not detect an association with socioeconomic factors, many issues may influence the use of these drug groups. First, their price (mainly GLP1As and SGLT2Is) was significantly higher than that of metformin or SU. Second, these drugs can only be prescribed with reimbursement by GPs under the recommendations of diabetologists [ 17 ], which may complicate access to these medications for some patients. Additionally, most GLP1As are subcutaneous injections, which may be difficult for some patients to accept, although one orally administered GLP1A has been available since 2020.
Our data clearly show that drug choice depends not only on socioeconomic factors, but also on numerous other factors, which may be difficult to detect at the population level, as the choice of drug is highly individualized. We did not find any other studies that investigated the possible determinants of regional antidiabetic medication use. However, in one study that investigated geographical variation in antibiotic use and its possible determinants in Hungary, large interregional differences and associations with some socioeconomic factors were found [ 24 ].
Comparing the results of our study, which included both reimbursed and non-reimbursed medication use, to the results of a previously published study based on only reimbursed medication use, it was revealed that there were considerable differences in the results [ 11 ]. The overall use of antidiabetic medications was 24% higher in our study in 2015 compared to the use of only reimbursed medication. In the cases of most antidiabetic subgroups, the differences were very small (the lowest was for insulins being only 1.2%) but was enormous in the case of metformin. The overall use of metformin in our study was more than double that of the reimbursed only metformin use. This can be explained by the fact that while most antidiabetic medications are reimbursed, some widely used metformin products are not.
The present study has some strengths and limitations that must be considered. As far the strengths, first, to the best of our knowledge this is the first study to investigate both total national and interregional antidiabetic medication utilization trends and differences in Hungary. Second, the database covers total antidiabetic drug sales in Hungary, including both reimbursed and non-reimbursed medications, and our study has total population coverage (nearly 10 million people), which enables us to detect a complete and detailed picture of the national and interregional trends and differences in antidiabetic medication use.
Regarding the limitations of this retrospective study, a wholesale database containing antidiabetic medication sales for pharmacies was used. Due to the nature of the data source, it provides a slight overestimation of antidiabetic use, as not all the medications acquired by pharmacies reach the patients for various reasons (e.g. medication expires before selling, damaged medications). In addition, the data were aggregated and it was not possible to distinguish between the drug claims of patients with type 1 and type 2 diabetes. Some antidiabetics, such as metformin, may be used for indications other than diabetes, but our data did not contain information about indications of use. The database contains sales data of reimbursed and non-reimbursed medicines, however, the differentiation among these drug categories was not possible in the present study. In some cases, data on regional level were not available for potentially relevant determining factors. It should be noted that this study aimed to analyze antidiabetic medication use at the population level and explore the changes over time, but did not aim to evaluate the appropriateness of the choice of treatment, as it could only be performed on individual patient-level medication use and clinical data.
In this study, we provided a detailed picture of antidiabetic medication use patterns in Hungary at both the national and regional levels. Although DPP4I, GLP1A and SGLT2I use was dynamically growing in Hungary, the share of sulfonylurea use is still considerable. Differences in antidiabetic drug consumption are substantial between regions, mainly in the case of GLP1As, SGLT2Is and sulfonylureas. The association between socioeconomic factors and regional drug use was confirmed only for sulfonylureas. The choice of therapy is highly individual and may depend on several patient- and healthcare-related factors; therefore, population level determining factors cannot necessarily explain regional differences. Future analysis of patient level data may help identify patient related and healthcare related factors that possibly contribute to regional differences in antidiabetic medication use.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
Dipeptidyl peptidase 4 inhibitor
Glucagon-like peptide-1 analogue
Sodium-glucose co-transporter 2 inhibitor
Anatomic therapeutic chemical classification code
Defined daily doses
Defined daily dose per 1000 inhabitants per day
Glycated hemoglobin A1c
International Diabetes Federation. IDF Diabetes Atlas, 10th edition. Brussels, Belgium. 2021. https://www.diabetesatlas.org . Last accessed 08 January 2024.
Hungarian Central Statistical Office. Dissemination database Statistics by subject. Main diseases of adults. http://statinfo.ksh.hu/Statinfo/ . Last accessed 08 January 2024.
Scheen AJ. Clinical pharmacology of antidiabetic drugs: what can be expected of their use? Presse Med. 2022;52(1):104158. https://doi.org/10.1016/j.lpm.2022.104158 .
Article PubMed Google Scholar
American Diabetes Association. Pharmacologic approaches to Glycemic Treatment: standards of Medical Care in Diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S140–57. https://doi.org/10.2337/dc23-S009 .
Article Google Scholar
Jermendy G, editor. Clinical Practice Guideline– Diagnosis of diabetes, and antihyperglycaemic treatment and care of patients with diabetes in adulthood. Diabetologia Hungarica 2020; 28(3): 119–204. https://doi.org/10.24121/dh.2020.14 [In Hungarian].
Jermendy G, editor. Clinical Practice Guideline– Diagnosis of diabetes, and antihyperglycaemic treatment and care of patients with diabetes in adulthood. Diabetologia Hungarica 2023; 31(5): 331–444. https://doi.org/10.24121/dh.2023.20 [In Hungarian].
Davies MJ, Aroda VR, Collins BS, Gabbay RA, et al. Management of hyperglycemia in type 2 diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753–86. https://doi.org/10.2337/dci22-0034 .
Article CAS PubMed PubMed Central Google Scholar
The Medicines Utilisation Monitoring Centre. National Report on Medicines use in Italy. Year 2022. Rome: Italian Medicines Agency. 2023. ISBN: 979-12-80335-30-2 https://www.aifa.gov.it/documents/20142/1967301/Rapporto-OsMed-2022.pdf Last accessed 20 February 2024.
Moura AM, Martins SO, Raposo JF. Consumption of antidiabetic medicines in Portugal: results of a temporal data analysis of a thirteen-year study (2005–2017). BMC Endocr Disord. 2021;21(1):30. https://doi.org/10.1186/s12902-021-00686-w .
Russo V, Orlando V, Monetti VM, Galimberti F. at al,; Geographical Variation in Medication Prescriptions: A Multiregional Drug-Utilization Study. Front Pharmacol. 2020;11:418. https://doi.org/10.3389/fphar.2020.00418 .
Csatordai M, Benkő R, Matuz M, Bor A, et al. Use of glucose-lowering drugs in Hungary between 2008 and 2017: the increasing use of novel glucose-lowering drug groups. Diabet Med. 2019;36(12):1612–20. https://doi.org/10.1111/dme.14117 .
Article CAS PubMed Google Scholar
Jermendy G, Kiss Z, Rokszin G, Abonyi-Tóth Z, et al. Changing Patterns of Antihyperglycaemic Treatment among Patients with Type 2 Diabetess. Med in Hungary between 2015 and 2020-Nationwide Data from a Register-Based Analysis. Med (Kaunas). 2022;58(10):1382 https://doi.org/10.3390/medicina58101382
WHO Collaborating Centre for Drug Statistics Methodology. Guidelines for ATC classification and DDD assignment, 2022. Oslo: WHO Collaborating Centre for Drug Statistics Methodology; 2021.
Google Scholar
World Health Organization. Introduction to drug utilization research. Geneva: World Health Organization; 2003.
Hungarian Central Statistical Office. http://statinfo.ksh.hu/ Last accessed 08 January 2024.
National Health Insurance Fund of Hungary. Report on the World Diabetes Day. 2020. http://neak.gov.hu/sajtoszoba/kozlemenyek_eu_napok/egeszsegugyi_vilagnapok_cukorbetegseg Last accessed 08 January 2024.
National Health Insurance Fund of Hungary. Precribing with reimbursement. https://neak.gov.hu/felso_menu/szakmai_oldalak/gyogyszer_segedeszkoz_gyogyfurdo_tamogatas/Szakembereknek/Tajekoztato Last accessed 08 January 2024.
Krulichová IS, Selke GW, Bennie M, Hajiebrahimi M, et al. Comparison of drug prescribing before and during the COVID-19 pandemic: a cross-national European study. Pharmacoepidemiol Drug Saf. 2022;31(10):1046–55. https://doi.org/10.1002/pds.5509 .
Article CAS Google Scholar
Pottegård A, Andersen JH, Søndergaard J, Thomsen RW, et al. Changes in the use of glucose-lowering drugs: a Danish nationwide study. Diabetes Obes Metab. 2023;25(4):1002–10. https://doi.org/10.1111/dom.14947
Bucsa C, Farcas A, Iaru I, Mogosan C, et al. Drug utilization study of antidiabetic medication during 2021– 2019 in Romania. Int J Clin Pract. 2021;75(11):e14770. https://doi.org/10.1111/ijcp.14770
Kostev K, Gölz S, Scholz B, Kaiser M, et al. Time to insulin initiation in type 2 diabetes patients in 2010/2011 and 2016/2017 in Germany. J Diabetes Sci Technol. 2019;13(6):1129–34. https://doi.org/10.1177/1932296819835196 .
Samson SL, Vellanki P, Blonde L, Christofides EA, et al. American Association of Clinical Endocrinology Consensus Statement: Comprehensive Type 2 Diabetes Management Algorithm– 2023 update. Endocr Pract. 2023;29(5):305–40. https://doi.org/10.1016/j.eprac.2023.02.001 .
National Health Insurance Fund of Hungary. Medication dispensing database. http://www.neak.gov.hu/felso_menu/szakmai_oldalak/publikus_forgalmi_adatok/gyogyszer_forgalmi_adatok . Last accessed 08 January 2024.
Matuz M, Benko R, Doro P, Hajdu E, et al. Regional variations in community consumption of antibiotics in Hungary, 1996–2003. Br J Clin Pharmacol. 2006;61(1):96–100. https://doi.org/10.1111/j.1365-2125.2005.02525.x
Article PubMed PubMed Central Google Scholar
Download references
Acknowledgements
Not applicable.
This work has been implemented with support provided by the Ministry of Innovation and Technology of Hungary from the National Research, Development and Innovation Fund, financed by ITM NKFIA TKP2021-EGA-32. The funder had no influence on the study design, data analysis, data interpretation, or the writing of the article. University of Szeged Open Access Fund Grant Number: 6747.
Open access funding provided by University of Szeged.
Author information
Authors and affiliations.
Faculty of Pharmacy, Institute of Clinical Pharmacy, University of Szeged, Szikra utca 8, 6725, Szeged, Hungary
Márta Csatordai, Ria Benkő, Mária Matuz, Zsófia Engi, Dezső Csupor & Péter Doró
Albert Szent-Györgyi Health Centre, Central Pharmacy, University of Szeged, Szeged, Hungary
Márta Csatordai, Ria Benkő & Mária Matuz
Albert Szent-Györgyi Health Centre, Department of Internal Medicine, University of Szeged, Szeged, Hungary
Csaba Lengyel
You can also search for this author in PubMed Google Scholar
Contributions
Conceptualization: MC, PD; methodology: MC, PD, MM, RB; data analysis: MC, PD, MM; interpretation of data: all authors; writing– original draft: MC, PD; writing– review and editing: all authors. All authors read and approved the final version of the manuscript.
Corresponding author
Correspondence to Péter Doró .
Ethics declarations
Ethics approval and consent to participate, consent for publication, competing interests.
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1:
Utilization tendencies of antidiabetic medication in Hungarian regions between 2015 and 2021.
Supplementary Material 2:
Available fixed-dose combinations in Hungary during the study period
Supplementary Material 3:
Calculation of DDD/TID
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Csatordai, M., Benkő, R., Matuz, M. et al. Trends and regional differences in antidiabetic medication use: a nationwide retrospective observational study. Diabetol Metab Syndr 16 , 88 (2024). https://doi.org/10.1186/s13098-024-01334-8
Download citation
Received : 11 January 2024
Accepted : 10 April 2024
Published : 24 April 2024
DOI : https://doi.org/10.1186/s13098-024-01334-8
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Diabetes mellitus
- Drug utilization
- Antidiabetics
- Regional differences
- Glucagon-like peptide-1 analogues
- Sodium-glucose co-transporter 2 inhibitors
- Sulfonylureas
Diabetology & Metabolic Syndrome
ISSN: 1758-5996
- Submission enquiries: [email protected]
- Open access
- Published: 22 April 2024
Molar root canal treatment performed by undergraduate dental students; an observational study of procedural errors and student perception
- Ahmad M. El-Ma’aita 1 , 2 ,
- Sari A. Mahasneh 1 , 2 ,
- Maryam A. Hamandi 2 &
- Mohammad A. Al-Rabab’ah 1 , 2
BMC Medical Education volume 24 , Article number: 437 ( 2024 ) Cite this article
250 Accesses
Metrics details
Molar root canal treatment (RCT) is challenging and requires training and specific skills. Rotary instrumentation (RI) reduces the time needed for instrumentation but may increase the risk of certain procedural errors. The aims of this study were to evaluate the quality of molar RCTs provided by undergraduate students, to compare the prevalence of procedural errors following manual and RI, and to assess the students’ self-perceived confidence to perform molar RCT without supervision and their preference for either manual or RI.
Molar RCTs performed by the final year students were evaluated radiographically according to predefined criteria (Appendix 1). The procedural errors, treatment details, and the students’ self-perceived confidence to perform molar RCT and their preference for either manual or RI were recorded. Descriptive statistics were performed, and the Chi-squared test was used to detect any statistically significant differences.
60.4% of RCTs were insufficient. RI resulted in more sufficient treatments compared with MI (49% vs. 30.3% respectively. X 2 : 7.39, p = 0.007), required fewer visits to complete (2.9 vs. 4.6 respectively. X 2 : 67.23, p < 0.001) and was the preferred technique by 93.1% of students. The most common procedural errors were underextension of the root canal obturation (48.4%), insufficient obturation (45.5%), and improper coronal seal (35.2%) without a significant difference between the two techniques. 26.4% of the participating students reported that they did not feel confident to perform molar RCT without supervision.
The quality of molar RCT provided by UG students was generally insufficient. RI partially improved the technical quality of RCT compared with MI. UG students need further endodontic training and experience before they can safely and confidently practise molar RCT.
Peer Review reports
Root canal treatment (RCT) aims to control intra-radicular infection and prevent or treat apical periodontitis [ 1 ]. It comprises chemo-mechanical disinfection, where canals are instrumented and shaped to their full extension and disinfected using irrigants and medicaments, and then obturated in three-dimension to ensure a fluid-tight seal apically, laterally and coronally [ 2 , 3 ]. RCT is a technically demanding procedure that requires specific training and skills especially in molar teeth. Undergraduate (UG) students may lack the skills and experience necessary to carry out molar RCT. Only 13–47% of RCTs completed by UG students were of acceptable quality [ 4 , 5 , 6 , 7 , 8 ].
Procedural errors may occur during RCT even with experienced clinicians. They can manifest as errors in length control, instrumentation-related errors and insufficient obturation. The presence of such errors can jeopardize canal debridement, which may, in turn, compromise the outcome of endodontic treatment [ 9 , 10 ]. Rotary instrumentation (RI) uses motor driven nickel-titanium (NiTi) instruments that are super-elastic and demonstrate higher resistance to torsional failure compared with stainless steel instruments [ 11 , 12 ]. RI was shown to perform better than manual instrumentation (MI) when used by unexperienced clinicians and resulted in fewer procedural errors [ 13 , 14 ]. Its integration into UG dental education was suggested [ 13 ].
Research that evaluates student learning outcome should utilize competency measures as the main outcome [ 15 ]. However, students’ self-perceived confidence can influence the student’s ability to demonstrate competency and may be useful as a secondary outcome [ 16 ]. The students’ self-perceived confidence in performing endodontic procedures was the lowest for performing RCT of maxillary and mandibular molars among a list that involves a wide range of endodontic procedures [ 17 ]. Less than 40% of new dental graduates were confident to perform endodontic treatment on multirooted teeth [ 18 ].
The need for this study stems from multiple observations by our faculty supervising UG endodontic work that students struggled to perform molar RCT and that procedural errors were frequent. The aims of this observational study were (a) to assess the quality of molar RCTs provided by UG students, (b) to compare the prevalence of procedural errors associated with manual and rotary instrumentation and (c) to assess the students’ self-perceived confidence to perform molar RCT without supervision and their preference for either manual or RI.
The protocol of this study was approved by the review board committee of the Jordan University Hospital (ref 10/2022/1726). Informed consent was obtained from the participating students and their patients. All final year dental students at the University of Jordan ( n = 149) were invited to participate in this study. No exclusion criteria were implemented, and no students form other colleges were included. Molar RCTs performed by the final year dental students at the University of Jordan between October 2021– May 2022 were evaluated radiographically according to predefined criteria (Appendix 1 ). All the treated cases were of low difficulty according to the American Association of Endodontists’ case difficulty assessment form [ 19 ]. All RCTs were performed under rubber dam isolation. Working length was determined using apex locators and confirmed with a working length radiograph. Canal instrumentation was performed either manually using the step back technique, or with rotary instrumentation using the ProTaper Gold® system (Dentsply Maillefer, Baillagues, Switzerland). Obturation was carried out with gutta percha and resin sealer (AH-plus, Dentsply DeTrey, Konstanz, Germany) using cold lateral condensation. Students were supervised by faculty throughout the treatments provided. However, different supervisors were allocated to different groups of students. It was not possible to assign the same supervisors for all students due to the busy clinics schedule.
Treatment details including the number of visits used to complete the treatment, the students’ preference for either instrumentation technique, and their self-perceived confidence to perform RCT without supervision were recorded using an online questionnaire (Appendix 2 ). The questionnaire was designed was piloted on 10 students and was tested for face and content validity. The first 10 respondents were asked to complete the survey once again after one week to ensure the survey was reliable.
Post-obturation radiographs (manual type E films, Kodak, Carestream Health, Rochester, NY, USA) were assessed in a dark room using an X-ray viewer (Dentsply Rinn, Konstanz, Germany). Procedural errors that were detectable on the post-obturation peri-apical radiograph were recorded, and each completed RCT was marked as either sufficient or insufficient (Appendix 1 ). The first 10 RCTs were jointly evaluated by 3 assessors (AE, MA, and SM) following a discussion of the errors detected to ensure good calibration of the assessors. The rest of the RCTs were evaluated independently by 2 clinicians (AE and MA). In cases where there was a disagreement, the third experienced consultant endodontist (SM) was consulted. Descriptive statistics as well as the Chi-squared test were used.
A total of 109 students consented to participate. 104 students performed molar RCTs using both techniques and 5 students only performed manual instrumentation. Post-obturation radiographs of 213 RCTs were assessed (109 using MI and 104 using RI). 75.6% of treated teeth were first molars (26.8% maxillary and 48.8% mandibular) while 24.4% were second molars (10.3% maxillary and 14.1% mandibular). The overall mean number of visits required to complete the treatment was 3.7 (median: 4, standard deviation: 1.55). RI enabled the students to complete their treatment in fewer visits compared with MI (2.9 vs. 4.6 visits respectively, X 2 : 67.23, p < 0.001).
The procedural errors (as defined in Appendix 1 ) and their prevalence are summarised in Table 1 . Examples of the procedural errors are illustrated in Fig. 1 .

Procedural errors detected in the post-obturation radiographs; ( a ) under-extension of obturation in the mesio-buccal root of the maxillary right first molar, ( b ) canal transportation in the mesial root of the mandibular left first molar, ( c ) separated instrument in the mesio-lingual root of the mandibular left first molar, and ( d ) Defective coronal restoration in the mandibular right first molar
The overall technical quality of RCTs was deemed sufficient in 39.6% of the cases. There was no statistically significant difference in the quality of RCTs provided or the prevalence of procedural errors between maxillary and mandibular molars. RI resulted in more sufficient treatments compared with MI (49% vs. 30.3% respectively) (X 2 : 7.39, p = 0.007). The interrater reliability was excellent (Kappa statistic: 0.83).
Most students (93.1%) reported that they preferred RI over manual, while 6.9% of them had no preference. More than one quarter of the students (26.4%) reported that they did not feel confident to perform molar RCT without supervision.
Patients with procedural errors were informed of the unfortunate mishap and were either kept under observation, referred to a consultant endodontist or the post-graduate endodontic clinics, or, where the procedural errors were non-reparable, referred for extraction of the involved tooth.
This study demonstrated that procedural errors were very common, be it in manual or RI, and that students generally did not feel confident to perform molar RCT on their own without being supervised.
More than 60% of the treatments provided were judged to have either compromised the tooth structure, resulted in irreversible damage to the tooth or required further intervention before definitive restoration of the tooth could be completed. This is in agreement with the reported quality of RCT performed by UG students in different parts of the world [ 4 , 5 , 6 , 7 ]. RI only partially improved the quality of RCT and did not result in an acceptable level of sufficient treatments. A recent systematic review demonstrated a high tendency for procedural errors with MI [ 20 ].
The most common procedural error detected was under-extension of the root canal filling. The position of the apical constriction in relation to the radiographic apex is variable. In our study, 2 mm short of the radiographic apex was used as the cut-off point in accordance with previously published literature [ 6 , 21 , 22 ]. Under-extended root canal obturation could be explained by multiple reasons including errors in working length determination, ledge formation, lack of recapitulation during the step-back phase of instrumentation, separated instruments, improper master cone selection and improper obturation technique. The specific reason for this procedural error could not be identified in this observational study. Over-extension of the root canal filling was observed more often in MI. Lack of apical stop creation and overzealous instrumentation can be implicated for this procedural error.
Canal transportation was encountered more frequently following MI. It occurs due to the files’ inherent tendency to restore their original linear shape during canal instrumentation [ 23 ]. This is in accordance with other published studies [ 24 , 25 ].
Obturation of the instrumented canals is essential and aims to entomb any residual infection and provide a fluid-tight seal against the ingress of fluids from the peri-radicular tissues [ 3 ]. Different techniques and materials have been described but none proved to be superior to the rest. In this study, obturation was completed using cold lateral condensation. Unexperienced clinicians may find this technique difficult to apply especially in narrow canals and in patients with limited mouth openings. This was evident in our results as almost half of the obturations had voids or were poorly condensed. The sealer-based obturation technique used with calcium silicate sealers can provide a simpler obturation option as it only requires the insertion of a single cone of gutta percha with no further condensation [ 26 ]. Coronal seal is an essential part of RCT [ 27 ]. Proper adaptation of a coronal restoration to sound tooth structure prevents the ingress of saliva into the obturated root canal system, and therefore prevents reinfection. A leaky coronal restoration (definitive or provisional) not only risks reinfection of the root canal system, but also exposes the tooth to recurrent caries which may compromise its restorability [ 27 ].
This study was based on radiographic assessment of the RCTs provided. While radiographs can reveal important mechanical aspects of RCT such as the extension, taper, and condensation of the root filling as well as the adaptation of the coronal restoration, they do not allow the assessment of the biological part of treatment [ 28 ]. Isolation during treatment, the irrigation protocol (solution(s), volume, time, activation… etc.), interappointment medication and quality and timing of coronal restoration are all factors that may influence the treatment outcome yet cannot be assessed radiographically. However, to achieve the best possible outcome, the mechanical steps of RCT should be executed to a very high standard and procedural errors should be avoided as much as possible. Poor technical quality of RCT was demonstrated to be a risk factor for apical periodontitis [ 9 , 29 ].
The European society of endodontology’s undergraduate curriculum guidelines for endodontology recommend that “all students should gain adequate experience in the treatment of anterior, premolar and molar teeth in both the pre-clinical and clinical environment” [ 30 ]. They also state that clinical training should be based on competencies rather than a minimum number of performed procedures. Students should be trained to consider all treatment options, be competent at assessing tooth restorability and treatment complexity and to recognize when referral to a specialist should be considered [ 30 ].
This study has multiple limitations. It only evaluated the radiographic quality of molar RCTs. No clinical aspect was taken into consideration. Its lack of temporal factor precluded any observation of the success or failure of treatments and their association (or lack of) with the technical quality of the treatments provided. Clinical supervision varied between the participating students and there was no correlation between the students’ academic performance and the technical quality of RCTs. Potential confounding factors to the results include the level of academic performance of students, the variance in clinical supervision, the technical difficulty of the RCT provided, and the variation in outcome assessment between the assessors. No attempts to adjust for the confounding factors were made as the purpose of the study was to report on the prevalence of procedural errors rather than investigating the potential reasons for them. However, this study demonstrates an overall poor quality of molar RCT provided by UG students, combined with their lack of confidence to perform this procedure without supervision. This invites the question of whether UG students should be expected to perform molar RCT at such an early stage of their careers, or whether this procedure requires further training, mentorship and experience that may not be ideally delivered during undergraduate training. Inexperienced clinicians may benefit from a wider exposure to simple RCTs of anterior and premolar teeth before they can embark on the more technically demanding molar RCT. The authors suggest that UG endodontic clinical training should emphasize on providing simple RCTs on anterior and premolar teeth and on the conservative and emergency management of molar teeth such as vital pulp therapy, access cavity and coronal pulp extirpation, and incision and drainage. Clinicians who wish to perform molar RCT should receive further training following graduating from the dental school.
The technical quality of molar RCT provided by UG students is generally insufficient. RI partially improved the quality of RCT compared with MI when used by inexperienced operators (UG students). Most students preferred RI over MI. UG students need further endodontic training and experience before they can safely and confidently practise molar RCT.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
manual instrumentation
root canal treatment
rotary instrumentation
undergraduate
Schilder H. Cleaning and shaping the root canal. Dent Clin North Am. 1974;18(2):269–96.
Article Google Scholar
Ruddle CJ. Cleaning and shaping the root canal system. In: Cohen S, Bums RC, eds Pathways of Pulp, 8th edn St Louis, MO, USA: Mosby. 2002:231–291.
European Society of E. Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J. 2006;39(12):921–30.
Barrieshi-Nusair KM, Al-Omari MA, Al-Hiyasat AS. Radiographic technical quality of root canal treatment performed by dental students at the Dental Teaching Center in Jordan. J Dent. 2004;32(4):301–7.
Elsayed RO, Abu-Bakr NH, Ibrahim YE. Quality of root canal treatment performed by undergraduate dental students at the University of Khartoum, Sudan. Aust Endod J. 2011;37(2):56–60.
Hayes SJ, Gibson M, Hammond M, Bryant ST, Dummer PM. An audit of root canal treatment performed by undergraduate students. Int Endod J. 2001;34(7):501–5.
Kumar M, Duncan HF. Radiographic evaluation of the technical quality of undergraduate endodontic ‘competence’ cases in the Dublin Dental University Hospital: an audit. J Ir Dent Assoc. 2012;58(3):162–6.
Google Scholar
Micoogullari Kurt S, Kandemir Demirci G, Serefoglu B, Kaval ME, Guneri P, Caliskan MK. Quality of root canal treatment performed by undergraduate students using nickel-titanium reciprocating versus hand instruments. J Dent Educ 2022.
Eckerbom M, Flygare L, Magnusson T. A 20-year follow-up study of endodontic variables and apical status in a Swedish population. Int Endod J. 2007;40(12):940–8.
Sjogren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod. 1990;16(10):498–504.
Thompson SA. An overview of nickel-titanium alloys used in dentistry. Int Endod J. 2000;33(4):297–310.
Zhou B, Zhou Y, Tang K. An overview of structure, mechanical properties, and treatment for age-related tendinopathy. J Nutr Health Aging. 2014;18(4):441–8.
Sonntag D, Delschen S, Stachniss V. Root-canal shaping with manual and rotary Ni-Ti files performed by students. Int Endod J. 2003;36(11):715–23.
Fariniuk LF, Westphalen VP, Silva-Neto UX, Carneiro E, Baratto Filho F, Fidel SR, Fidel RA. Efficacy of five rotary systems versus manual instrumentation during endodontic retreatment. Braz Dent J. 2011;22(4):294–8.
Gabbard T, Romanelli F. The Accuracy of Health professions Students’ self-assessments compared to objective measures of competence. Am J Pharm Educ. 2021;85(4):8405.
Hay I, Ashman A, van Kraayenoord CE. Investigating the influence of achievement on self-concept using an intra-class design and a comparison of the PASS and SDQ-1 self-concept tests. Br J Educ Psychol. 1997;67(Pt 3):311–21. discussion 339–343.
Javed MQ, Bhatti UA. Students’ performance in clinics and self-perceived confidence in performing endodontic procedures: a correlation study. Pak J Med Sci. 2023;39(1):203–8.
Alsoghier A, Ali K. Self-perceived preparedness of new dental graduates from a Middle Eastern university. Eur J Dent Educ. 2023. https://doi.org/10.1111/eje.12981 .
AAE Endodontic Case Difficulty Assessment Form and, Guidelines. [ https://www.aae.org/specialty/wp-content/uploads/sites/2/2022/01/CaseDifficultyAssessmentFormFINAL2022.pdf ].
Ribeiro DM, Reus JC, Felippe WT, Pacheco-Pereira C, Dutra KL, Santos JN, Porporatti AL, De Luca Canto G. Technical quality of root canal treatment performed by undergraduate students using hand instrumentation: a meta-analysis. Int Endod J. 2018;51(3):269–83.
Ray HA, Trope M. Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. Int Endod J. 1995;28(1):12–8.
Saunders WP, Saunders EM, Sadiq J, Cruickshank E. Technical standard of root canal treatment in an adult Scottish sub-population. Br Dent J. 1997;182(10):382–6.
American Association of Endodotists. Glossary of Endodontic Terms. 2020, 10th edition ( https://www.aae.org/specialty/clinical-resources/glossary-endodontic-terms/ ).
Guelzow A, Stamm O, Martus P, Kielbassa AM. Comparative study of six rotary nickel-titanium systems and hand instrumentation for root canal preparation. Int Endod J. 2005;38(10):743–52.
Peralta-Mamani M, Rios D, Duarte MAH, Santiago Junior JF, Honorio HM. Manual vs. rotary instrumentation in endodontic treatment of permanent teeth: a systematic review and meta-analysis. Am J Dent. 2019;32(6):311–24.
Kim JH, Cho SY, Choi Y, Kim DH, Shin SJ, Jung IY. Clinical efficacy of Sealer-based Obturation Using Calcium Silicate Sealers: a Randomized Clinical Trial. J Endod. 2022;48(2):144–51.
Atlas A, Grandini S, Martignoni M. Evidence-based treatment planning for the restoration of endodontically treated single teeth: importance of coronal seal, post vs no post, and indirect vs direct restoration. Quintessence Int. 2019;50(10):772–81.
Eckerbom M, Magnusson T. Evaluation of technical quality of endodontic treatment–reliability of intraoral radiographs. Endod Dent Traumatol. 1997;13(6):259–64.
Kirkevang LL, Vaeth M, Horsted-Bindslev P, Bahrami G, Wenzel A. Risk factors for developing apical periodontitis in a general population. Int Endod J. 2007;40(4):290–9.
De Moor R, Hulsmann M, Kirkevang LL, Tanalp J, Whitworth J. Undergraduate curriculum guidelines for endodontology. Int Endod J. 2013;46(12):1105–14.
Download references
Acknowledgements
Not applicable.
This research received no funding.
Author information
Authors and affiliations.
Restorative Dentistry Department, University of Jordan, Amman, Jordan
Ahmad M. El-Ma’aita, Sari A. Mahasneh & Mohammad A. Al-Rabab’ah
Jordan University Hospital, Amman, Jordan
Ahmad M. El-Ma’aita, Sari A. Mahasneh, Maryam A. Hamandi & Mohammad A. Al-Rabab’ah
You can also search for this author in PubMed Google Scholar
Contributions
A.E.: Study design and writing the manuscript. S.M.: Writing the discussion. M.H.: Data collection and processing. M.A.: Statistical analysis and reviewed the manuscript.
Corresponding author
Correspondence to Ahmad M. El-Ma’aita .
Ethics declarations
Ethics approval and consent to participate.
The protocol of this study was approved by the review board committee of the Jordan University Hospital (ref 10/2022/1726). Informed consent was obtained from the participating students and their patients.
Consent for publication
Competing interests.
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary material 2, rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
El-Ma’aita, A.M., Mahasneh, S.A., Hamandi, M.A. et al. Molar root canal treatment performed by undergraduate dental students; an observational study of procedural errors and student perception. BMC Med Educ 24 , 437 (2024). https://doi.org/10.1186/s12909-024-05397-z
Download citation
Received : 23 August 2023
Accepted : 05 April 2024
Published : 22 April 2024
DOI : https://doi.org/10.1186/s12909-024-05397-z
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Dental education
- Manual instrumentation
- Procedural errors
- Root canal treatment
- Rotary instrumentation
BMC Medical Education
ISSN: 1472-6920
- Submission enquiries: [email protected]
- General enquiries: [email protected]
- Open access
- Published: 22 April 2024
Association of healthy eating index and self-rated health in adults living in Tehran: a cross-sectional study
- Bahareh Jabbarzadeh-Ganjeh 1 ,
- Kurosh Djafarian 2 &
- Sakineh Shab-Bidar 1 , 3
BMC Public Health volume 24 , Article number: 1106 ( 2024 ) Cite this article
205 Accesses
1 Altmetric
Metrics details
Self-rated health (SRH) has been identified in many studies as a valid predictor of mortality and healthcare utilization. There is limited research on SRH and dietary intake. This study aimed to investigate the association between healthy eating index (HEI) and SRH in adults living in Tehran.
This cross-sectional study was carried out among 850 adult men and women aged 20–59 years who visited health centers in Tehran from 2021 to 2022. Dietary intake was assessed using a validated and reliable semiquantitative food frequency questionnaire with 168 food items, and SRH was assessed with one question: “In general, how do you rate your health?“. We categorized SRH into excellent/very good, good, and fair/poor. In the descriptive statistics part, we used mean ± standard deviation or number (ratio) for quantitative and qualitative variables, respectively. The chi-squared test and one-way analysis of variance were used to calculate the percentage and mean for demographic characteristics across tertiles of SRH. An analysis of covariance was used to compare the means of energy, macronutrients, the HEI, and its component variables across the tertiles of SRH.
The final sample included 795 participants (68.2% female; mean ± standard deviation age: 44.81 ± 10.62 years) whose 40% reported excellent/very good SRH, and 30% reported good and fair/poor SRH separately. There was no association between body mass index, physical activity, education, health status, smoking, and sleep duration with SRH. After adjustment, the total HEI score and its component scores did not differ across the tertiles of SRH status. However, participants with good SRH had a higher intake of total energy (mean difference (MD): 180.33 Kcal, P value < 0.001), total fat (MD: 8.15 gr, P value = 0.002), and total carbohydrates (MD: 20.18 gr, P value = 0.004) than those with fair/poor SRH.
According to our findings, fair/poor SRH was associated with a lower consumption of total energy, total fat, and total carbohydrates in Iranian adults. Additional observational studies would be necessary to clarify these findings.
Peer Review reports
Introduction
Self-rated health (SRH) is one of the most commonly evaluated health conceptions in population-based and clinical studies [ 1 , 2 ]. SRH asks people to rate their general health qualitatively via a short question [ 3 ]. It has been identified in many studies as a strong predictor of mortality and might predict the incidence of diseases [ 4 ]. Some studies have shown that poor SRH status could predict greater healthcare utilization and diminish physical performance in the adult population [ 3 , 5 ]. The total cost of physical or psychological disorders and illnesses, including healthcare expenses and lost economic productivity, amounts to trillions [ 6 ]. Therefore, SRH as a screening tool [ 2 ] might be helpful to lower the healthcare budget. SRH affects the healthy behaviors of people. For older adults, SRH is a retrospective health history assessment and is, therefore, more indicative of their health status than many blood markers [ 7 ].
In the past, nutritional epidemiology mostly focused on the relationship between diseases and specific nutrients, such as vitamins, or specific food groups, such as vegetables and fruits. However, currently, more studies are focused on dietary patterns and evaluating the quality and variety of the whole diet [ 5 ]. Based on dietary guidelines, the diet plan should be low-fat, rich in fruits and vegetables, and generally have a high nutrient density [ 5 ]. There are different ways to assess diet quality, such as the food frequency questionnaire (FFQ), healthy eating index (HEI), alternative healthy eating index (AHEI), etc [ 5 , 8 , 9 ]... The HEI was created on dietary guidelines for Americans, and the scoring was based on adequacy components (foods to eat more of for good health) and moderation components (foods to limit for good health) [ 10 ]. Both HEI and AHEI scores ranged from 0 to 100, where a higher score presents a healthier diet [ 11 ]. A cross-sectional study in Tehran recently estimated the mean HEI score was 52.5, while it was 62.3 in 2001 [ 12 , 13 ]. A systematic review assessed the diet quality using AHEI, and the worldwide mean score was 40.3 among 185 countries from 1990 to 2018. Another systematic review of cohort studies found an association between higher scores of HEI and AHEI with lower risk of all-cause mortality (20%), cardiovascular disease (20%), cancer (14%), type 2 diabetes (19%), and neurodegenerative disease (18%) [ 14 ]. One study reported that those who consumed equal to or less than two servings of fruits and vegetables per day or consumed high-fat foods mostly had poor/fair SRH scores [ 15 ]. Another cross-sectional study revealed a significant and negative association between overweight and low physical activity with SRH [ 16 ].
To date, the status of SRH has not been investigated in Iran. Furthermore, studies exploring the relationship between SRH and the quality of diet, particularly HEI, are scarce. We wanted to determine whether having a better SRH can be associated with a better healthy diet. Conducting this study will help us to have a better understanding of SRH and self-assessment among Iranians. Therefore, this study aimed to determine the association between healthy eating index and self-rated health in adults living in Tehran.
Study design
The study was a cross-sectional population-based survey of those aged 20–59 years from 2021 to 2022. The data were collected from 850 healthy adult men and women through two-stage cluster sampling. In the first stage, a simple random sample was selected within 25 healthcare centers across five different geographic areas of Tehran, and a convenient sampling method was used for the second stage. People who visited health centers in Tehran and met the inclusion criteria were informed about the implementation and objectives of the study via informed consent forms. The research was approved by the Tehran University of Medical Science Human Research Ethics Committee (IR.TUMS.MEDICINE.REC.1401.604).
Data collection
A demographic questionnaire was used for general information through face-to-face interviews. It included age (year), sex (male/female), education level (illiterate/under diploma/diploma/university), occupation (employed/unemployed), marital status (single/married), smoking (yes/quit smoking/no), health status (healthy/one disease/comorbidity), and sleep duration.
Dietary intake assessment
We used a validated and reliable semiquantitative FFQ with 168 food items for each participant to assess their dietary intake. The nutritionist asked about FFQs from the participants through face-to-face interviews. The macro- and micronutrient intake were analyzed using Iranian-designed Nutrition IV Software (First Database, San Bruno, CA).
HEI was calculated based on predetermined criteria by the United States Department of Agriculture [ 17 ]. The 2015 version of this index has nine components related to adequacy and four related to moderation. The total score is the sum of the score of adequacy components (i.e. foods to eat more of for good health) and moderation components (i.e. foods to limit for good health). The HEI scores ranged from 0 to 100, where a higher score presents a healthier die [ 18 ]. The adequacy part includes the following: (1) Total fruit (includes fruit juice), (2) Whole fruits (all forms except fruit juice), (3) Total vegetables (includes any beans and peas), (4) Greens and beans (includes any beans and peas), (5) Whole grains, (6) Dairy (includes all milk products, such as fluid milk, yogurt, and cheese, and fortified soy beverages), (7) Total protein foods (beans and peas are included here (and not with vegetables) when the Total Protein Foods standard is otherwise not met), (8) Seafood and plant proteins (includes seafood, nuts, seeds, soy products (other than beverages) as well as beans and peas if they counted as Total Protein Foods), and (9) Fatty acids (ratio of poly- and monounsaturated fatty acids to saturated fatty acids). The moderation components consist of (1) refined grains, (2) sodium, (3) added sugars, and (4) saturated fats [ 18 ].
Self-rated health assessment
SRH was assessed by asking one question, “In general, how do you rate your health?“. The answers include excellent, very good, good, fair, and poor [ 19 ]. For this study, we combined the “excellent, very good” responses as one subgroup and “fair, poor” responses as another. Therefore, SRH responses were categorized into excellent/very good, good, and fair/poor. This method aligns with other studies that have used the SRH status question [ 2 , 20 ] and makes a better differentiation between positive and negative responses [ 21 ].
Physical activity
We used the short form of the international physical activity questionnaire, validated for the Iranian population [ 22 ]. Participants were questioned about the time spent on vigorous, moderate, and walking activities within the last seven days. The physical activity score was calculated based on the metabolic equivalent minutes per week (MET-minutes/week). At last, the physical activity level is categorized into low (< 600 MET-min/week), moderate (600–3000 MET-min/week), and high levels (> 3000 MET-min/week) [ 23 ].
Assessment of blood pressure
Blood pressure was measured twice by a digital sphygmomanometer (Beurer, BC 08, Germany) after at least 10–15 min of rest. An average of two blood pressures was reported for each person.
Anthropometric measurements
The participant’s height without shoes was measured using a wall stadiometer with a sensitivity of 0.1 cm (Seca, Germany). Weight was evaluated by a digital scale (808 Seca, Germany) with an accuracy of 0.1 kg with minimum clothes on. Body mass index (BMI) was calculated by dividing the weight (kg) by the square of the height (m) [ 24 ]. Based on the WHO, the BMI cut-off points for determining underweight, normal weight, overweight, and obesity are < 18.5, 18.5–24.9, 25-29.9, and ≥ 30, respectively [ 25 ]. Waist (WC) and hip (HC) circumferences were measured with a flexible nonelastic metric tape. WC was measured between the lowest rib and the Iliac crest during exhalation, while HC was at the point that yielded the maximum diameter over the buttocks [ 24 ]. The waist-to-hip ratio (WHR) was calculated by dividing the WC (cm) by HC (cm) [ 26 ]. The waist-to-height ratio (WHtR) was computed by dividing the WC (cm) by height (cm) [ 27 ]. We applied a single nutritionist performing all the measurements to reduce the odds of subjective errors.
Statistical analysis
The general characteristics of the participants are displayed as the mean and standard deviation or number and percent. We categorized SRH into excellent/very good, good, and fair/poor. The normality test of the data was through the Kolmogorov‒Smirnov test and the Q‒Q plot to determine the normal distribution of the data. The chi-squared test and one-way analysis of variance (ANOVA) were calculated as the percentage and mean for demographic characteristics across tertiles of SRH. To compare the means of energy, macronutrients, the HEI, and its component variables across the tertiles of SRH, we applied an analysis of covariance (ANCOVA), adjusting for age, sex, education, occupation, marital status, smoking status, health status, physical activity, and BMI. All analyses were performed with SPSS (SPSS Inc., version 26) software. A p-value less than 0.05 accounted for a significant difference.
Based on Table 1 , the mean ± standard deviation of the participant’s age was 44.81 ± 10.62 years old. Of 850 participants, 17 were excluded due to underreporting, extreme values for protein and total fat intake, and 38 due to lack of information. The final sample included 795 participants, and 542 were female. In total, 40% of the population reported excellent/very good SRH, and 30% reported good and fair/poor SRH separately.
Table 2 shows the frequency and the mean of some demographic characteristics across tertiles of SRH. There was no association between BMI, physical activity, education, health status, smoking, or sleep duration, and SRH.
Table 3 indicates the multivariate-adjusted means of the HEI and its component scores across tertiles of SRH status. The results from the Tukey post hoc test showed that participants with good SRH compared with fair/poor SRH had significant differences in total energy consumption (mean difference (MD): 180.33 Kcal, P value < 0.001), total carbohydrate (MD: 20.18 gr, P value = 0.004), and total fat intake (MD: 8.15 gr, P value = 0.002). Additionally, those with good SRH had lower scores for Total Vegetable (P value = 0.058), Greens and Beans (P value = 0.059), and Dairy (P value = 0.042) compared with participants with fair/poor SRH. However, after adjusting for confounders, the marginal and significant differences were all gone.
In this cross-sectional study, we aimed to investigate the association between a healthy eating index (HHEI) and self-rated health (SRH) in adults living in Tehran. Our study found that 40% (318 participants) reported excellent/very good SRH, 30.1% (239 participants) reported good SRH, and 29.9% (238 participants) reported fair/poor SRH. There were no statistically significant associations between BMI, physical activity, education, health status, smoking, or sleep duration, and SRH. After adjustment, the total HEI score and its component scores did not differ across the tertiles of SRH status. However, participants with good SRH had a higher intake of total energy, total fat, and total carbohydrates than those with fair/poor SRH.
Two studies involving younger populations reported similar findings. A cross-sectional study among 1504 US adolescents found no significant association between HEI score and SRH. However, further analysis revealed specific dietary differences: those with excellent-good SRH had a higher vegetable score, while those with fair/poor SRH had a higher total fat intake score [ 3 ]. A cohort study conducted from 2003 to 2012 on 953 German participants also found no significant association between SRH and those with high healthy nutrition scores and below-average scores in the physical activity and media use index [ 28 ]. The studies suggest this might be due to developmental differences and potentially limited awareness of healthy eating habits in younger individuals [ 3 , 28 ].
Several studies support the association between unhealthy lifestyle factors and poorer SRH. The Spanish DiSA-UMH study found that poorer SRH was linked to lower adherence to the Mediterranean diet, lower physical activity levels, excess weight, and smoking among university students [ 29 ]. Similarly, studies by Zarini et al. and Collins et al. linked fair/poor SRH to higher fat intake [ 5 , 15 ], lower fruit and vegetable intake, and lower physical activity, particularly among females [ 15 ]. These findings align with our null findings for BMI and smoking, as reported in another study conducted in a rural Greek population [ 2 ].
Some studies reported positive associations between HEI and SRH, contrasting with our findings. Vaudin et al. observed a link between better SRH and a more favorable HEI score in older adults [ 20 ]. Additionally, studies in rural populations found associations between healthier diets and better SRH [ 1 , 2 ], while lower education and chronic diseases were linked to poorer SRH [ 2 ]. A large survey [ 30 ] also reported associations between poor sleep, physical inactivity, and poor diet quality with higher odds of poor SRH. However, it’s important to note that the participants in this survey had reported “good” SRH earlier.
Possible explanations for these contrasting findings include:
Population differences: The studies with contrasting findings involved different age groups, health statuses, and potentially socioeconomic backgrounds compared to our study population.
Health awareness: Individuals with chronic diseases might have higher health awareness due to more frequent medical consultations, potentially leading to healthier dietary choices [ 15 ].
Confounding factors: Many variables beyond those we adjusted for in our study, such as socioeconomic status [ 31 , 32 ] and mental health [ 32 ], can influence SRH.
This study has some limitations. First, some confounders, such as social well-being, were not adjusted. Second, the cross-sectional design and the lack of significant associations between HEI and SRH might mirror low power due to the small sample size in this analysis. Our study also has some strengths. The strengths of the current observational study include a sample representative of Tehran’s general population, the first study in Iran around this field, using the latest version of the HEI, a gold standard tool for assessing usual food intake (FFQ), and the inclusion of a large number of covariates.
This is the first attempt to relate SRH status to HEI in healthy Iranian adults. The total HEI score did not vary by SRH status. In detail, those with good SRH had a higher intake of total energy, total fat, and total carbohydrates than those with fair/poor SRH. Additional observational studies are needed to clarify these findings.
Data availability
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
self-rated health
food frequency questionnaire
healthy eating index
Body mass index
Waist circumference
hip circumferences
waist-to-hip ratio
waist-to-height ratio
standard deviation
one-way analysis of variance
analysis of covariance
mean difference
An R, Xiang X, Liu J, Guan C. Diet and self-rated health among oldest-old Chinese. Arch Gerontol Geriatr. 2018;76:125–32.
Article PubMed Google Scholar
Darviri C, Fouka G, Gnardellis C, Artemiadis AK, Tigani X, Alexopoulos EC. Determinants of self-rated health in a representative sample of a rural population: a cross-sectional study in Greece. Int J Environ Res Public Health. 2012;9(3):943–54.
Article PubMed PubMed Central Google Scholar
Goodwin DK, Knol LL, Eddy JM, Fitzhugh EC, Kendrick OW, Donahue RE. The relationship between self-rated health status and the overall quality of dietary intake of US adolescents. J Am Diet Assoc. 2006;106(9):1450–3.
Loftfield E, Yi S, Immerwahr S, Eisenhower D. Construct validity of a single-item, self-rated question of diet quality. J Nutr Educ Behav. 2015;47(2):181–7.
Collins CE, Young AF, Hodge A. Diet quality is associated with higher nutrient intake and self-rated health in mid-aged women. J Am Coll Nutr. 2008;27(1):146–57.
Saklayen MG. The global epidemic of the metabolic syndrome. Curr Hypertens Rep. 2018;20(2):12.
Wang K, Zhang A, Sun F, Hu RX. Self-rated Health among older Chinese americans: the roles of Acculturation and Family Cohesion. J Appl Gerontol. 2021;40(4):387–94.
Guenther PM, Casavale KO, Reedy J, Kirkpatrick SI, Hiza HA, Kuczynski KJ, Kahle LL, Krebs-Smith SM. Update of the healthy eating index: HEI-2010. J Acad Nutr Diet. 2013;113(4):569–80.
Kennedy ET, Ohls J, Carlson S, Fleming K. The healthy eating index: design and applications. J Am Diet Assoc. 1995;95(10):1103–8.
Article CAS PubMed Google Scholar
Vahid F, Jalili M, Rahmani W, Nasiri Z, Bohn T. A higher healthy eating index is Associated with decreased markers of inflammation and lower odds for being Overweight/Obese based on a case-control study. Nutrients. 2022;14(23):5127.
Article CAS PubMed PubMed Central Google Scholar
Miller V, Webb P, Cudhea F, Shi P, Zhang J, Reedy J, Erndt-Marino J, Coates J, Mozaffarian D. Global dietary quality in 185 countries from 1990 to 2018 show wide differences by nation, age, education, and urbanicity. Nat Food. 2022;3(9):694–702.
Yazdani V, Zeraattalab-Motlagh S, Jayedi A, Majdi M, Mirrafiei A, Martami F, Djafarian K, Shab-Bidar S. The association between self-reported nocturnal sleep duration, irregularity in daily energy intake and diet quality in a sample of Iranian adults. Public Health Nutr. 2023;26(8):1609–16.
Diet quality indices and the risk of type 2 diabetes in the Tehran Lipid and Glucose Study. BMJ Open Diabetes Research & Care 2022, 10(5):e002818.
Morze J, Danielewicz A, Hoffmann G, Schwingshackl L. Diet Quality as assessed by the healthy eating index, alternate healthy eating Index, Dietary approaches to stop hypertension score, and Health outcomes: a second update of a systematic review and Meta-analysis of Cohort studies. J Acad Nutr Diet. 2020;120(12):1998–2031. e1915.
Zarini GG, Vaccaro JA, Canossa Terris MA, Exebio JC, Tokayer L, Antwi J, Ajabshir S, Cheema A, Huffman FG. Lifestyle behaviors and self-rated health: the living for health program. J Environ Public Health. 2014;2014:315042.
Aguilar-Palacio I, Gil-Lacruz AI, Sánchez-Recio R, Rabanaque MJ. Self-rated health in Europe and its determinants: does generation matter? Int J Public Health. 2018;63(2):223–32.
Guenther PM, Reedy J, Krebs-Smith SM, Reeve BB. Evaluation of the healthy eating Index-2005. J Am Diet Assoc. 2008;108(11):1854–64.
Krebs-Smith SM, Pannucci TE, Subar AF, Kirkpatrick SI, Lerman JL, Tooze JA, Wilson MM, Reedy J. Update of the healthy eating index: HEI-2015. J Acad Nutr Diet. 2018;118(9):1591–602.
Krause NM, Jay GM. What do global self-rated health items measure? Med Care. 1994;32(9):930–42.
Vaudin A, Wambogo E, Moshfegh A, Sahyoun NR. Awareness and use of nutrition information predict measured and self-rated diet quality of older adults in the USA. Public Health Nutr. 2021;24(7):1687–97.
Manderbacka K, Lundberg O. Examining points of reference of self-rated health among Swedish oldest old. Arch Gerontol Geriatr. 1996;23(1):47–60.
Vasheghani-Farahani A, Tahmasbi M, Asheri H, Ashraf H, Nedjat S, Kordi R. The Persian, last 7-day, long form of the International Physical Activity Questionnaire: translation and validation study. Asian J Sports Med. 2011;2(2):106–16.
Ainsworth B, Herrmann S, Meckes N, Bassett D, Tudor-Locke C, Greer J, Vezina J, Whitt-Glover M, Leon A. 2011 Compendium of Physical activities: a second update of codes and MET values. Med Sci Sports Exerc. 2011;43:1575–81.
Physical status. The use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser. 1995;854:1–452.
Google Scholar
Barba C, Cavalli-Sforza T, Cutter J, Darnton-Hill I, Deurenberg P, Yap M, Gill T, James P, Ko G, Miu AH, et al. Appropriate body Mass Index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363:157–63.
Article Google Scholar
World Health Organisation. Waist Circumference and Waist-hip Ratio: Report of a WHO Expert Consultation, [ http://www.who.int/nutrition/publications/obesity/WHO_report_waistcircumference_and_waisthip_ratio/en/ ].
Ashwell M, Gibson S. Waist-to-height ratio as an indicator of ‘early health risk’: simpler and more predictive than using a ‘matrix’ based on BMI and waist circumference. BMJ Open. 2016;6(3):e010159.
Spengler S, Mess F, Schmocker E, Woll A. Longitudinal associations of health-related behavior patterns in adolescence with change of weight status and self-rated health over a period of 6 years: results of the MoMo longitudinal study. BMC Pediatr. 2014;14:242.
Barrios-Vicedo R, Navarrete-Muñoz EM, García de la Hera M, González-Palacios S, Valera-Gran D, Checa-Sevilla JF, Gimenez-Monzo D, Vioque J. [A lower adherence to Mediterranean diet is associated with a poorer self-rated health in university population]. Nutr Hosp. 2014;31(2):785–92.
PubMed Google Scholar
Oftedal S, Rayward AT, Fenton S, Duncan MJ. Sleep, diet, activity, and incident poor self-rated health: a population-based cohort study. Health Psychol. 2021;40(4):252–62.
Cheng G, Yan Y. Sociodemographic, health-related, and social predictors of subjective well-being among Chinese oldest-old: a national community-based cohort study. BMC Geriatr. 2021;21(1):124.
Meyer OL, Castro-Schilo L, Aguilar-Gaxiola S. Determinants of mental health and self-rated health: a model of socioeconomic status, neighborhood safety, and physical activity. Am J Public Health. 2014;104(9):1734–41.
Download references
Acknowledgements
Special thanks go to all those who participated in this study.
This manuscript has been granted by the Tehran University of Medical Sciences (Grant No: 57728).
Author information
Authors and affiliations.
Department of Community Nutrition, School of Nutritional Sciences and Dietetics, Tehran University of Medical Sciences (TUMS), No 44, Hojjat-dost Alley, Naderi St., Keshavarz Blvd, 14167-53955, Tehran, 14155/6117, Iran
Bahareh Jabbarzadeh-Ganjeh & Sakineh Shab-Bidar
Department of Clinical Nutrition, School of Nutritional Sciences and Dietetics, Tehran University of Medical Sciences (TUMS), 14167-53955, Tehran, Iran
Kurosh Djafarian
Sports Medicine Research Center, Neuroscience Institute, Tehran University of Medical Sciences (TUMS), Tehran, Iran
Sakineh Shab-Bidar
You can also search for this author in PubMed Google Scholar
Contributions
B.J-G and S.S-B contributed to the conception/design of the research; B.J-G contributed to the analysis, interpretation of the data, and drafting the first version of the manuscript; S.S-B and K.DJ critically revised the manuscript; and S.S-B agree to be fully accountable for ensuring the integrity and accuracy of the work. All authors read and approved the final manuscript.
Corresponding author
Correspondence to Sakineh Shab-Bidar .
Ethics declarations
Ethics approval and consent to participate.
The sample collection was made possible by the coordination of the Health Bureau of the Municipality of Tehran and the cooperation of the health care centers of Tehran. The study was approved by the ethical committee of the Tehran University of Medical Sciences (Ethics No. IR.TUMS.MEDICINE.REC.1401.604). All participants signed an informed consent form to participate statement.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Jabbarzadeh-Ganjeh, B., Djafarian, K. & Shab-Bidar, S. Association of healthy eating index and self-rated health in adults living in Tehran: a cross-sectional study. BMC Public Health 24 , 1106 (2024). https://doi.org/10.1186/s12889-024-18568-w
Download citation
Received : 02 November 2023
Accepted : 11 April 2024
Published : 22 April 2024
DOI : https://doi.org/10.1186/s12889-024-18568-w
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Self-assessment
- Self-rated health
BMC Public Health
ISSN: 1471-2458
- Submission enquiries: [email protected]
- General enquiries: [email protected]
- Open access
- Published: 22 April 2024
Perioperative serum syndecan-1 concentrations in patients who underwent cardiovascular surgery with cardiopulmonary bypass and its association with the occurrence of postoperative acute kidney injury: a retrospective observational study
- Atsushi Miyazaki 1 ,
- Mai Hokka 1 ,
- Norihiko Obata 1 &
- Satoshi Mizobuchi 1
BMC Anesthesiology volume 24 , Article number: 154 ( 2024 ) Cite this article
78 Accesses
Metrics details
Various factors can cause vascular endothelial damage during cardiovascular surgery (CVS) with cardiopulmonary bypass (CPB), which has been suggested to be associated with postoperative complications. However, few studies have specifically investigated the relationship between the degree of vascular endothelial damage and postoperative acute kidney injury (pAKI).
The objectives of this study were to measure perioperative serum syndecan-1 concentrations in patients who underwent CVS with CPB, evaluate their trends, and determine their association with pAKI.
This was a descriptive and case‒control study conducted at the National University Hospital. Adult patients who underwent CVS with CPB at a national university hospital between March 15, 2016, and August 31, 2020, were included. Patients who were undergoing preoperative dialysis, had preoperative serum creatinine concentrations greater than 2.0 mg dl −1 , who were undergoing surgery involving the descending aorta were excluded. The perioperative serum syndecan-1 concentration was measured, and its association with pAKI was investigated.
Fifty-two patients were included. pAKI occurred in 18 (34.6%) of those patients. The serum syndecan-1 concentration increased after CPB initiation and exhibited bimodal peak values. The serum syndecan-1 concentration at all time points was significantly elevated compared to that after the induction of anesthesia. The serum syndecan-1 concentration at 30 min after weaning from CPB and on postoperative day 1 was associated with the occurrence of pAKI (OR = 1.10 [1.01 to 1.21], P = 0.03]; OR = 1.16 [1.01 to 1.34], P = 0.04]; and the cutoff values of the serum syndecan-1 concentration that resulted in pAKI were 101.0 ng ml −1 (sensitivity = 0.71, specificity = 0.62, area under the curve (AUC) = 0.67 (0.51 to 0.83)) and 57.1 ng ml −1 (sensitivity = 0.82, specificity = 0.56, AUC = 0.71 (0.57 to 0.86)). Multivariate logistic regression analysis revealed that the serum syndecan-1 concentration on postoperative day 1 was associated with the occurrence of pAKI (OR = 1.02 [1.00 to 1.03]; P = 0.03).
The serum syndecan-1 concentration at all time points was significantly greater than that after the induction of anesthesia. The serum syndecan-1 concentration on postoperative day 1 was significantly associated with the occurrence of pAKI.
Trial registration
This study is not a clinical trial and is not registered with the registry.
Peer Review reports
Various postoperative complications can lead to increased mortality in patients receiving cardiovascular surgery (CVS) with cardiopulmonary bypass (CPB). Postoperative AKI (pAKI) is an important complication that occurs in 5–30% of patients undergoing CVS, and even small increases in serum creatinine concentrations have been reported to lead to increased mortality [ 1 ]. Recently, it has been suggested that management with goal-directed perfusion focusing on oxygen supply during CPB period may reduce the incidence of pAKI, but pAKI is multifactorial [ 2 ] and there is no established prevention protocol. Vascular endothelial damage is thought to be one of the causes of pAKI [ 3 , 4 , 5 ]. Rehm et al. reported that the vascular endothelium in patients undergoing CVS is easily destroyed due to inflammation induced by CPB, aortic occlusion, and ischemia–reperfusion injury [ 6 ]. In addition, it has been reported that the vascular endothelial glycocalyx, which is present on the surface of vascular endothelial cells, is fragile and sheds when subjected to invasive stresses such as CVS, leading to increased plasma concentrations of vascular endothelial glycocalyx components such as syndecan-1 [ 7 ]. Although previous studies have investigated the association between preoperative or postoperative serum syndecan-1 concentrations and pAKI, few studies have examined perioperative serum syndecan-1 levels and investigated the association with pAKI. In the present study, we hypothesized that the perioperative serum syndecan-1 concentration is associated with pAKI. The objectives of this study were to examine the perioperative trends in the serum syndecan-1 concentration in adult patients receiving CVS via CPB and to clarify the association between vascular endothelial damage and the occurrence of pAKI.
This was a single-center, retrospective, descriptive study performed to investigate the perioperative serum syndecan-1 concentration in patients who underwent CVS with CPB. This study was conducted using samples stored in a previous study [ 8 ].
Ethical approval for this study was provided by the Kobe University Graduate School of Medicine, Medical Ethics Committee (Chairperson Prof. Makoto Nakamura, approval number: B220044) on June 21, 2022.
A trained researcher collected the data and entered the information into a database. Data monitoring and source-data verification were conducted in accordance with a predefined plan. Due to the retrospective nature of the study, the need for informed consent was waived by the ethical committee. Instead, the researchers made appropriate disclosures about the study and provided the participants with the opportunity to refuse enrollment in the study.
Setting and participants
Adult patients who underwent CVS with CPB at a national university hospital between March 15, 2016, and August 31, 2020, were included in this study. Patients who were undergoing preoperative dialysis, had preoperative serum creatinine concentrations greater than 2.0 mg dl −1 , or who were undergoing surgery involving the descending aorta were excluded.
Patient characteristics
The following patient characteristics were obtained: age, sex, weight, height, ASA-PS, European System for Cardiac Operative Risk Evaluation II, presence of hypertension and diabetes mellitus, preoperative left ventricular ejection fraction (LVEF), and estimated glomerular filtration rate (eGFR). Surgical information, including operation time, aortic cross-clamp time, duration of CPB, type of procedure, and amount of transfusion during surgery, was also obtained.
Measurements of the serum syndecan-1 concentration
Serum syndecan-1 concentrations were measured at the following six time points: (T1) after induction of anesthesia, (T2) 1 h after initiation of CPB, (T3) 2 h after initiation of CPB, (T4) 30 min after weaning from CPB, (T5) 2 h after weaning from CPB, and (T6) postoperative day 1 (Fig. 1 ). The serum syndecan-1 concentration was measured using an enzyme-linked immunosorbent assay (ELISA) kit (Human CD138 ELISA Kit, Diaclone SAS, France). To prevent observer bias, the serum syndecan-1 concentration was measured by a third party not involved in the study.

Serum syndecan-1 concentration was measured at each time point. The serum syndecan-1 concentration was measured at the following 6 time points: T1) after anesthesia induction, T2) 1 h after initiation of CPB, T3) 2 h after initiation of CPB, T4) 30 min after weaning from CPB, T5) 2 h after weaning from CPB, and T6) on postoperative day 1
Anesthesia methods
Anesthesia was administered by the anesthesiologist in charge. At the facility where this study was conducted, 500 mg of methylprednisolone was administered before starting CPB. Heparin was used as an anticoagulant to control the activated clotting time for more than 400 s, and protamine was administered as a heparin antagonist when hemostasis was confirmed after weaning from CPB. The choice of the type and amount of transfusion and inotropic agent also depended on the anesthesiologist in charge.
CPB management
Several trained perfusionists controlled the circulatory dynamics during CPB period.
During the CPB procedure, the cardiac index was managed with the target of 2.4–2.6 L/min/m 2 , and oxygen delivery (DO 2 ) and oxygen consumption (VO 2 ) were monitored as needed.
Study outcomes
The primary outcome was the change in the perioperative serum syndecan-1 concentration. The secondary outcome was the association between the perioperative serum syndecan-1 concentration and pAKI incidence. The diagnosis of pAKI was based on the Kidney Disease Improving Global Outcomes classification system. Although AKI was defined as an increase in the serum creatinine concentration and a decrease in urine output, the authors decided not to adopt the criterion of urine output for the definition of AKI in the present study to avoid the influence of the use of a diuretic drug in patients.
Statistical analysis
All variables are expressed as medians 〔IQRs〕 or means ± SDs. First, the perioperative serum syndecan-1 concentrations were graphically plotted for all patients, and the serum syndecan-1 concentration at each measurement point were compared to that at T1. Comparisons between each measurement point were performed using the Mann‒Whitney U test. The patients were then divided into groups according to the presence or absence of pAKI, and the perioperative serum syndecan-1 concentration was graphically plotted for each group and compared at each time point. Comparisons between two groups were performed using the Mann‒Whitney U test. If the CPB duration was less than 2 h, the serum syndecan-1 concentration at T3 was not measured, and statistical analysis was performed only for those who had data.
A single regression analysis was performed to examine the association between serum syndecan-1 (syndecan-1/10) concentrations and pAKI at each time point. At the time points at which significant differences were detected in the single regression analysis, receiver operating characteristic (ROC) curve analysis was performed to estimate the cutoff value.
The χ2 test was used to analyze whether a serum syndecan-1 concentration above or below the cutoff value had an effect on the occurrence of pAKI.
Finally, multivariate logistic regression analysis was performed to evaluate the association between the serum syndecan-1 concentration and pAKI incidence. No statistical analysis for sample size determination was performed in this study, and a P value < 0.05 was considered to indicate a statistically significant difference. Statistical analysis was performed using SigmaPlot 14.5 (SYSTAT software, CA, United States).
Fifty-two patients who underwent CVS with CPB were included. pAKI occurred in 18 (34.6%) of those patients. Stage 1 and Stage 2 were 15 and 3, respectively.
Patient demographic characteristics
Table 1 shows a comparison of the demographic data of the patients with and without pAKI. There were more male patients with pAKI than female patients ( P = 0.01), and patients with AKI had a lower preoperative eGFR ( P = 0.02) than did those without pAKI. There were no significant differences between the two groups with respect to the other demographic parameters.
Changes in the serum syndecan-1 concentration
Figure 2 shows the perioperative changes in the serum syndecan-1 concentration. Six patients with a CPB duration of less than 2 h did not have a serum syndecan-1 measurement at T3. It began to increase with the initiation of CPB and then reached a bimodal peak value. The serum syndecan-1 concentration at all time points was significantly elevated compared to that at T1.

Perioperative serum syndecan-1 concentration. Shows the perioperative serum syndecan-1 concentrations at each time point. Serum syndecan-1 concentrations at all time points were significantly elevated compared to those at T1. * P < 0.05
Comparison of the serum syndecan-1 concentration between patients with and without pAKI
Figure 3 shows a comparison of perioperative serum syndecan-1 concentrations between patients with and without pAKI. Before and after weaning from CPB, the serum syndecan-1 concentration was not significantly different between the two groups, whereas there was a significant difference at T6 (patients with pAKI 97.1 〔73.5 to 127.2〕 ng ml −1 and patients without pAKI 53.3 〔38.7 to 74.4〕 ng ml −1 ( P < 0.01)). Table 2 shows the ORs and 95% CIs from the single logistic regressions of pAKI occurrence according to the serum syndecan-1 concentration at each time point. Serum syndecan-1 concentrations at T4 and T6 were associated with an increased risk of pAKI (T4: OR = 1.10 [1.01 to 1.21, P = 0.03]; T6: OR = 1.16 [1.01 to 1.34, P = 0.04]). To calculate the cutoff value for the occurrence of pAKI, ROC analysis was performed for the serum syndecan-1 concentrations at T4 and T6. The estimated cutoff value was 101.0 ng ml −1 (sensitivity: 0.71; specificity: 0.62; area under the curve (AUC) = 0.67 (0.51 to 0.83)) at T4 and 57.1 ng ml −1 (sensitivity: 0.82; specificity: 0.56; AUC = 0.71 (0.57 to 0.86)) at T6 (Fig. 4 ). To analyze whether this cutoff value was significantly associated with the development of AKI, a χ2 test was performed. The cutoff value at T4 was not significantly associated with the occurrence of pAKI (χ2 (1) = 0.34, P = 0.56), whereas the cutoff value at T6 was significantly associated with the occurrence of pAKI (χ2 (1) = 4.55, P = 0.03). Finally, to evaluate the association between the serum syndecan-1 concentration at T6 and the occurrence of pAKI, multivariable logistic regression was conducted to control for the potentially confounding effects that are thought to be associated with pAKI (age, CPB duration, preoperative estimated glomerular filtration rate (eGFR)) and the serum syndecan-1 concentration at T6. Table 3 shows the ORs and 95% CIs from logistic regressions of pAKI occurrence adjusted for patient and setting characteristics, as described above. A high serum syndecan-1 concentration at T6 was associated with the occurrence of pAKI (OR = 1.02 (1.00 to 1.03), P = 0.03).

Comparisons of perioperative serum syndecan-1 concentrations in patients with and without pAKI. Shows a comparison of the perioperative serum syndecan-1 concentrations between patients with and without pAKI at the 6 time points. The white box plots indicate values for patients without pAKI, and the black box plots indicate values for patients with pAKI. * P < 0.05

ROC curves of the serum syndecan-1 concentration at T4 and T6 for the prediction of pAKI. The black line represents the ROC curve for T4, and the red line represents that for T6
In this study, we investigated the perioperative serum syndecan-1 concentration in patients who underwent CVS with CPB as an indicator of vascular endothelial damage and evaluated its impact on pAKI. The serum syndecan-1 concentration began to increase after the initiation of CPB and then exhibited a bimodal peak. Serum syndecan-1 concentrations at all time points were significantly elevated compared to those at T1. Simple linear regression analysis revealed that the serum syndecan-1 concentration at T4 and T6 influenced the occurrence of pAKI. The estimated cutoff values were 101.0 ng ml −1 and 57.1 ng ml −1 , respectively. The cutoff value of the serum syndecan-1 concentration at T6 was also shown to independently influence pAKI occurrence according to the χ2 test. The results of logistic regression analysis adjusted for covariates thought to be associated with the occurrence of pAKI also indicated that the serum syndecan-1 concentration at T6 was associated with pAKI.
The glycocalyx is a complex consisting of a core protein that penetrates vascular endothelial cells, glycosaminoglycans, hyaluronic acid, and other sugar chains [ 1 ]. The vascular endothelial glycocalyx has various physiological functions, including regulating vascular permeability, regulating leukocyte migration, and inhibiting thrombosis [ 9 , 10 ]. Syndecan-1 is a core protein of the glycocalyx. When the glycocalyx is disrupted and detached from the vascular endothelium, the blood concentration of syndecan-1 increases, indirectly providing an estimate of the degree of glycocalyx disruption [ 11 ].
Several studies have shown that various factors associated with CVS, such as sympathetic hyperactivity, ischemia–reperfusion injury, induction of inflammatory conditions, and volume overload, can cause vascular endothelial cell injury [ 12 , 13 , 14 ]. Bruegger et al. measured the intraoperative serum syndecan-1 concentration in patients who underwent on-pump or off-pump coronary artery bypass grafting (CABG). In the on-pump CABG group, the serum syndecan-1 concentration increased twofold above the baseline level at the time of aortic occlusion release and further increased at weaning from CPB. On the other hand, a significant increase in the serum syndecan-1 concentration was also observed in the off-pump CABG group at the end of central anastomosis [ 15 ]. Rehm et al. showed trends in the serum syndecan-1 concentration during ascending aortic replacement surgery involving CPB and abdominal aortic replacement surgery involving aortic occlusion. The serum syndecan-1 concentration increased by 65-fold above the preoperative level 2 min before weaning from CPB during ascending aortic replacement surgery and increased 15-fold above the preoperative level 15 min after the withdrawal of aortic occlusion during abdominal aortic replacement surgery [ 16 ]. He et al. measured the perioperative serum syndecan-1 concentration in patients who underwent CVS with CPB. The serum syndecan-1 concentration began to increase within 10 min after CPB initiation and peaked when the aortic occlusion was released [ 17 ]. In previous studies, the serum syndecan-1 concentration during CPB peaked at the time of weaning from CPB and then rapidly declined due to rapid metabolism from the kidneys [ 5 ]. In contrast, in the present study, the serum syndecan-1 concentration temporarily decreased at 30 min after weaning from CPB and then increased again. There are several possible reasons for this discrepancy. First, in the present study, the duration of CPB and aortic occlusion was longer than that in previous studies, and the longer duration of CPB and aortic occlusion may have resulted in greater damage to the vascular endothelium. Second, massive infusions have been reported to cause glycocalyx disorders by promoting the release of ANP [ 13 , 14 ]. Although the present study had insufficient data on blood transfusions after weaning from CPB, excessive infusion may be associated with glycocalyx disorders.
In the present study, there was a significant difference in the serum syndecan-1 concentration between the pAKI group and non pAKI group at T6. Univariate analysis revealed that serum syndecan-1 concentrations at T4 and T6 were associated with pAKI. Several studies have investigated the relationship between vascular endothelial damage and pAKI in patients with CVS. Saqib H. Qureshi et al. used porcine models to compare a group undergoing surgery with CPB and a group undergoing sham surgery to examine the effects of CPB on renal dysfunction, and they analyzed the effects of CPB on renal vascular endothelial cells using immunofluorescence probing. In their study, there was a significant reduction in creatinine clearance in Porcinis patients who underwent surgery with CPB. In addition, immunofluorescence probing revealed a significant decrease in glycosaminoglycan, a component of the glycocalyx, in renal vascular endothelial cells from porcine patients who underwent surgery with CPB compared to those who underwent a sham operation [ 3 ]. Several studies have also been conducted on humans. De Melo Bezerra Cavalcante et al. reported an association between early postoperative serum syndecan-1 concentrations and pAKI in children undergoing CVS. Their results showed that a decrease in the serum syndecan-1 concentration within 2 h after surgery was associated with the occurrence of pAKI. They also reported that the cutoff value of the serum syndecan-1 concentration that predicts the development of severe AKI (KDIGO stage 2 or 3) was 66.4 ng mL −1 [ 4 ]. Kim et al. measured the serum syndecan-1 concentration at the induction of anesthesia and at weaning from CPB in patients undergoing valvular surgery and analyzed the association between the serum syndecan-1 concentration and pAKI incidence. They found that a serum syndecan-1 concentration > 90 ng ml −1 at induction of anesthesia was associated with an increased risk of pAKI [ 5 ]. While these studies have shown an association between preoperative or postoperative serum syndecan-1 concentrations and the occurrence of pAKI, little is known about the association between serum syndecan-1 concentrations measured throughout the perioperative period and the occurrence of pAKI. The present study differs from previous studies in that the perioperative serum syndecan-1 concentration was frequently measured to determine the trends and associations of these changes with the occurrence of pAKI.
This study has several limitations. First, since this was a small, single-center study, it is not clear whether this is true for all races, and further data validation in patients with the same background is needed to determine whether the cutoff values derived from this study are correct. Second, patients with preexisting renal dysfunction (serum creatinine level ≥ 2 mg dl −1 ) were excluded from the study. This may also explain why no difference in the baseline serum syndecan-1 concentration was found . However, whether the results of the present study apply to patients with chronic renal failure is unknown and requires further investigation. Third,
The trends in the perioperative serum syndecan-1 concentration and its association with the occurrence of pAKI in patients undergoing CVS with CPB were investigated. The serum syndecan-1 concentration began to increase after the initiation of CPB and then exhibited a bimodal peak. The serum syndecan-1 concentration at all time points was significantly elevated compared to that after the induction of anesthesia. The serum syndecan-1 concentration on postoperative day 1 was associated with the occurrence of pAKI. The estimated cutoff value was 57.1 ng ml −1 (sensitivity = 0.82, specificity = 0.56, AUC = 0.71 (0.57 to 0.86)). Multivariate analysis revealed that the serum syndecan-1 concentration on postoperative day 1 was associated with the occurrence of pAKI.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
Cardiovascular surgery
Cardiopulmonary bypass
Postoperative acute kidney injury
European System for Cardiac Operative Risk Evaluation II
Estimated glomerular filtration rate
Left ventricular ejection fraction
Red cell concentrate
Flesh frozen plasma
Lassnigg A, Schmidlin D, Mouhieddine M, Bachmann LM, Druml W, Bauer P, Hiesmayr M. Minimal changes of serum creatinine predict prognosis in patients after cardiothoracic surgery: a prospective cohort study. J Am Soc Nephrol. 2004;15(6):1597–605.
Article CAS PubMed Google Scholar
O’Neal JB, Shaw AD. Billings FTt: Acute kidney injury following cardiac surgery: current understanding and future directions. Crit Care. 2016;20(1):187.
Article PubMed PubMed Central Google Scholar
Qureshi SH, Patel NN, Murphy GJ. Vascular endothelial cell changes in postcardiac surgery acute kidney injury. Am J Physiol Renal Physiol. 2018;314(5):F726-f735.
de Melo Bezerra Cavalcante CT,. Castelo Branco KM, Pinto Júnior VC, Meneses GC, de Oliveira Neves FM, de Souza NM, Penaforte KL, Martins AM, Libório AB: Syndecan-1 improves severe acute kidney injury prediction after pediatric cardiac surgery. J Thorac Cardiovasc Surg. 2016;152(1):178-186.e172.
Article PubMed Google Scholar
Kim HB, Soh S, Kwak YL, Bae JC, Kang SH, Song JW. High Preoperative Serum Syndecan-1, a Marker of Endothelial Glycocalyx Degradation, and Severe Acute Kidney Injury after Valvular Heart Surgery. J Clin Med. 2020;9(6):1803.
Article CAS PubMed PubMed Central Google Scholar
Rehm M, Bruegger D, Christ F, Conzen P, Thiel M, Jacob M, Chappell D, Stoeckelhuber M, Welsch U, Reichart B, et al. Shedding of the endothelial glycocalyx in patients undergoing major vascular surgery with global and regional ischemia. Circulation. 2007;116(17):1896–906.
Suzuki K, Okada H, Sumi K, Tomita H, Kobayashi R, Ishihara T, Kakino Y, Yoshiyama N, Yasuda R, Kitagawa Y, et al. Serum syndecan-1 reflects organ dysfunction in critically ill patients. Sci Rep. 2021;11(1):8864.
Okada H, Yoshida S, Hara A, Ogura S, Tomita H. Vascular endothelial injury exacerbates coronavirus disease 2019: The role of endothelial glycocalyx protection. Microcirculation. 2021;28(3):e12654.
Chelazzi C, Villa G, Mancinelli P, De Gaudio AR, Adembri C. Glycocalyx and sepsis-induced alterations in vascular permeability. Crit Care. 2015;19(1):26.
Pillinger NL, Kam P. Endothelial glycocalyx: basic science and clinical implications. Anaesth Intensive Care. 2017;45(3):295–307.
Suzuki K, Okada H, Takemura G, Takada C, Kuroda A, Yano H, Zaikokuji R, Morishita K, Tomita H, Oda K, et al. Neutrophil Elastase Damages the Pulmonary Endothelial Glycocalyx in Lipopolysaccharide-Induced Experimental Endotoxemia. Am J Pathol. 2019;189(8):1526–35.
Chappell D, Bruegger D, Potzel J, Jacob M, Brettner F, Vogeser M, Conzen P, Becker BF, Rehm M. Hypervolemia increases release of atrial natriuretic peptide and shedding of the endothelial glycocalyx. Crit Care. 2014;18(5):538.
Robich M, Ryzhov S, Kacer D, Palmeri M, Peterson SM, Quinn RD, Carter D, Sheppard F, Hayes T, Sawyer DB, et al. Prolonged Cardiopulmonary Bypass is Associated With Endothelial Glycocalyx Degradation. J Surg Res. 2020;251:287–95.
Myers GJ, Wegner J. Endothelial Glycocalyx and Cardiopulmonary Bypass. J Extra Corpor Technol. 2017;49(3):174–81.
Bruegger D, Rehm M, Abicht J, Paul JO, Stoeckelhuber M, Pfirrmann M, Reichart B, Becker BF, Christ F. Shedding of the endothelial glycocalyx during cardiac surgery: on-pump versus off-pump coronary artery bypass graft surgery. J Thorac Cardiovasc Surg. 2009;138(6):1445–7.
He G, Gao Y, Feng L, Wu Q, Gao W, Lin L, Wang W. Correlation Between Wall Shear Stress and Acute Degradation of the Endothelial Glycocalyx During Cardiopulmonary Bypass. J Cardiovasc Transl Res. 2020;13(6):1024–32.
Download references
Acknowledgements
We would like to express our gratitude to Dr. Moritoki Egi, the professor of the Department of Anesthesia, Kyoto University Hospital, for his support from the conceptual stage in carrying out this study and to Miho Kimura, a researcher in the Division of Anesthesiology, Department of Surgery Related, Kobe University Graduate School of Medicine, for her assistance with the syndecan-1 measurements.
This work was supported by JSPS KAKENHI (grant number 20K17781).
Author information
Authors and affiliations.
Division of Anesthesiology, Department of Surgery Related, Kobe University Graduate School of Medicine, 7-5-2 Kusunoki Cho, Chuo-Ku, Kobe, Hyogo, 650-0017, Japan
Atsushi Miyazaki, Mai Hokka, Norihiko Obata & Satoshi Mizobuchi
You can also search for this author in PubMed Google Scholar
Contributions
AM performed the statistical analysis and drafted the work. MH substantively revised the work and was a major contributor to the writing of the manuscript. NO has interpreted the data. SM made substantial contributions to the conception of the study. All the authors read and approved the final manuscript.
Corresponding author
Correspondence to Mai Hokka .
Ethics declarations
Ethics approval and consent to participate.
Ethical approval for this study was provided by the Ethical Committee on June 21, 2022. Due to the retrospective nature of the study, the need for informed consent was waived by the ethical committee.
The name of ethics committee: Kobe University Graduate School of Medicine, Medical Ethics Committee (Chairperson Prof. Makoto Nakamura).
Approval number: no. B220044.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Miyazaki, A., Hokka, M., Obata, N. et al. Perioperative serum syndecan-1 concentrations in patients who underwent cardiovascular surgery with cardiopulmonary bypass and its association with the occurrence of postoperative acute kidney injury: a retrospective observational study. BMC Anesthesiol 24 , 154 (2024). https://doi.org/10.1186/s12871-024-02546-1
Download citation
Received : 08 February 2024
Accepted : 17 April 2024
Published : 22 April 2024
DOI : https://doi.org/10.1186/s12871-024-02546-1
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Endothelial injury
- Acute kidney injury
BMC Anesthesiology
ISSN: 1471-2253
- Submission enquiries: [email protected]
- General enquiries: [email protected]
SYSTEMATIC REVIEW article
Correlation analysis between low birth weight and impaired glucose tolerance in children: a systematic review and meta-analysis provisionally accepted.

- 1 Heping Hospital Affiliated to Changzhi Medical College, China
- 2 Guangzhou Red Cross Hospital, China
The final, formatted version of the article will be published soon.
Background: A potential association between the onset of diabetes and normal birth weight (NBW) has been discovered. Diverse conclusions and study methodologies exist regarding the connection between low birth weight (LBW) and impaired glucose tolerance in children, underscoring the need for further robust research. Our institution is embarking on this study to thoroughly examine the association between LBW and impaired glucose tolerance in children.We conducted searches on Cochrane Library, ScienceDirect, EMBASE, PubMed, China National Knowledge Infrastructure (CNKI), Chinese Biomedical Literature data (CBM) online database, VIP full-text Database, and Wanfang Database to identify correlation analyses or case-control studies investigating the relationship between LBW and abnormal glucose tolerance in children. The search spanned from January 2010 to September 2023. The quality of observational studies was evaluated using the Newcastle-Ottawa Scale (NOS) tool. Data synthesis was performed using the statistical software RevMan 5.3 for meta-analysis.Results: Based on the preferred reporting items for systematic reviews and metaanalysis (PRISMA) guidelines, we finally included 10 clinical control studies consisting of a total of 2971 cases. There wasn't considerably change in blood sugar levels among LBW, NBW and high birth weight (HBW) infants (P>0.05). There was no significant difference in insulin levels between LBW infants and NBW infants (P>0.05). The HOMA-IR of LBW infants was considerably higher than that of NBW infants (P<0.05). The risk of abnormal glucose tolerance in LBW infants was 0.42 times higher than that in NBW and HBW infants [Fisher's Z = 0.42, 95% CI = (0.09,0.75), P=0.01].LBW is associated with an increased risk of abnormal glucose tolerance, as indicated by elevated HOMA-IR level in LBW infants compared to NBW and HBW pediatric population. Further research is needed to confirm and expand upon these findings to better understand the complex relationship between LBW and impaired glucose tolerance in children.
Keywords: Newborn, low birth weight, Abnormal glucose tolerance, diabetes, Meta-analysis
Received: 27 Dec 2023; Accepted: 23 Apr 2024.
Copyright: © 2024 Ma, Lian, Mo and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY) . The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
* Correspondence: Mx. Youfang Wang, Guangzhou Red Cross Hospital, Guangzhou, China
People also looked at
IMAGES
VIDEO
COMMENTS
Cohort studies and case-control studies are two primary types of observational studies that aid in evaluating associations between diseases and exposures. In this review article, we describe these study designs, methodological issues, and provide examples from the plastic surgery literature. Keywords: observational studies, case-control study ...
We may approach this study by 2 longitudinal designs: Prospective: we follow the individuals in the future to know who will develop the disease. Retrospective: we look to the past to know who developed the disease (e.g. using medical records) This design is the strongest among the observational studies. For example - to find out the relative ...
The case study group has a particular attribute while the control group does not. The two groups are then compared, to see if the case group exhibits a particular characteristic more than the control group. ... The key difference between observational studies and experiments is that a properly conducted observational study will never attempt to ...
Cohort, cross sectional, and case-control studies are collectively referred to as observational studies. Observational studies are often the only practicable method of answering questions of aetiology, the natural history and treatment of rare conditions and instances where a randomised controlled trial might be unethical.
Introduction. Case-control and cohort studies are observational studies that lie near the middle of the hierarchy of evidence. These types of studies, along with randomised controlled trials, constitute analytical studies, whereas case reports and case series define descriptive studies (1). Although these studies are not ranked as highly as ...
Cohort, cross sectional, and case-control studies are collectively referred to as observational studies. Often these studies are the only practicable method of studying various problems, for example, studies of aetiology, instances where a randomised controlled trial might be unethical, or if the condition to be studied is rare. Cohort studies are used to study incidence, causes, and prognosis.
A specific method used to strengthen observational studies (the "restricted cohort" design 9) adapts principles of the design of randomized, controlled trials to the design of an observational ...
Observational studies Cohort studies, case control studies and cross sectional studies are all types of observational studies. Cohort studies. ... Another issue is the difference between association and cause. Just because there is an association between a factor and a disease, it doesn't mean that the factor causes the disease. ...
Case Studies & Observation Studies. A case study is a detailed study of a particular person, group or organisation. Focus is placed on the case study because the basic facts tend to help us understand a wider scientific truth. On the other hand they can also be used to challenge an accepted theory and so prompt scientists to change their thinking.
Observational studies are used for assessing the mean levels, the natural variation, and the structure of variables, as well as for determining the strength of the association between variables and - in the case of longitudinal studies - the temporal direction of the association between variables. Overview
Unravel the differences between observational and experimental studies. Dive into the intricacies of each method and discover their unique applications in research. 5927 Webb Rd Tampa FL 33615 (813) 249-9100. ... Case-Control Studies: Case-control studies, on the other hand, involve the comparison of individuals with a particular condition or ...
Actually, the term is "Sample Survey" and you may search online for it. I think the difference lies in the aim of the three types of studies, sample surveys want to get data for a parameter while observational studies and experiments want to convert some data into information, i.e., correlation and causation respectively.
Observational studies can be prospective or retrospective studies.On the other hand, randomized experiments must be prospective studies.. The choice between an observational study vs experiment hinges on your research objectives, the context in which you're working, available time and resources, and your ability to assign subjects to the experimental groups and control other variables.
Attrition refers to participants leaving a study. It always happens to some extent—for example, in randomized controlled trials for medical research. Differential attrition occurs when attrition or dropout rates differ systematically between the intervention and the control group.As a result, the characteristics of the participants who drop out differ from the characteristics of those who ...
The differences in design between the two types of study were as follows: the dose of nifedipine in the observational study was 30 to 60 mg, as compared with 30 to 50 mg in the randomized ...
Still, the correlations between fatigue severity and neuropsychological tests were more prominent in the case of MS. There were no differences in the severity of depression among groups.
This retrospective observational case-control study was conducted at Asan Medical Center, a tertiary referral center in Seoul, South Korea. ... A Student's t-test and Chi-squared test were used to evaluate the demographic and ocular differences between the groups depending on the variable types. Univariate and multivariable linear ...
From a prospective cohort study consisting of 96 participants, which aimed to investigate risk factors and injuries over an eleven-month athletics season [], a subsample of 53 elite athletics competitors (26 males (M), 27 females (F)) aged 22.2 ± 2.8 years, were selected for inclusion in this study.The majority of these athletes were part of the Swedish national team and regularly ...
Background Although there are some data regarding the COVID-19 vaccine and in in vitro fertilization (IVF) treatments, its potential impact in terms of serum immunoglobulin G (IgG) levels has not been evaluated prospectively. This study aimed to assess the effect of COVID-19 vaccine and IgG levels on IVF outcomes. Methods This observational, cohort study was conducted at a referral IVF unit ...
In the case of DPP4Is, the difference between the regions was lower than that of the other two drug groups; the max/min ratio was 1.70 in 2021, and a clear geographical gradient was not observed. ... M. et al. Trends and regional differences in antidiabetic medication use: a nationwide retrospective observational study. Diabetol Metab Syndr 16 ...
Molar root canal treatment (RCT) is challenging and requires training and specific skills. Rotary instrumentation (RI) reduces the time needed for instrumentation but may increase the risk of certain procedural errors. The aims of this study were to evaluate the quality of molar RCTs provided by undergraduate students, to compare the prevalence of procedural errors following manual and RI, and ...
Self-rated health (SRH) has been identified in many studies as a valid predictor of mortality and healthcare utilization. There is limited research on SRH and dietary intake. This study aimed to investigate the association between healthy eating index (HEI) and SRH in adults living in Tehran. This cross-sectional study was carried out among 850 adult men and women aged 20-59 years who ...
Background Various factors can cause vascular endothelial damage during cardiovascular surgery (CVS) with cardiopulmonary bypass (CPB), which has been suggested to be associated with postoperative complications. However, few studies have specifically investigated the relationship between the degree of vascular endothelial damage and postoperative acute kidney injury (pAKI). The objectives of ...
Background: A potential association between the onset of diabetes and normal birth weight (NBW) has been discovered. Diverse conclusions and study methodologies exist regarding the connection between low birth weight (LBW) and impaired glucose tolerance in children, underscoring the need for further robust research. Our institution is embarking on this study to thoroughly examine the ...