- Warning Signs and Symptoms
- Mental Health Conditions
- Common with Mental Illness
- Mental Health By the Numbers
- Individuals with Mental Illness
- Family Members and Caregivers
- Kids, Teens and Young Adults
- Veterans & Active Duty
- Identity and Cultural Dimensions
- Frontline Professionals
- Mental Health Education
- Support Groups
- NAMI HelpLine
- Publications & Reports
- Podcasts and Webinars
- Video Resource Library
- Justice Library
- Find Your Local NAMI
- Find a NAMIWalks
- Attend the NAMI National Convention
- Fundraise Your Way
- Create a Memorial Fundraiser
- Pledge to Be StigmaFree
- Awareness Events
- Share Your Story
- Partner with Us
- Advocate for Change
- Policy Priorities
- NAMI Advocacy Actions
- Policy Platform
- Crisis Intervention
- State Fact Sheets
- Public Policy Reports
- Your Journey

Youth and Young Adult Resources
Mental health conditions typically begin during childhood, adolescence or young adulthood. Here you will find additional information intended to help provide young people, educators, parents and caregivers with the resources they need. From a free downloadable coloring and activity book to a teen mental heath education presentation, to a guide for navigating college with a mental health condition, this page has resources for all young people. It also has handy information for parents, caregivers, and educators, like a one-pager on how to start a conversation about mental health and an example week of wellness activities that can be used at home.
For Young People
Meet Little Monster Coloring & Activity Book
Created by NAMI Washington, Meet Little Monster is a mental health coloring and activity book that provides children with a tool for helping express and explore their feelings in a fun, creative and empowering way. Available for download at no-cost in multiple languages. Learn More
Teens and Young Adults
Commitment Planner
A resource to help students balance their school, work and personal time to help their mental well-being! Download Resource Download Resource in Spanish
Finding A Trusted Adult
Reaching out about mental health can be or feel overwhelming, embarrassing or just hard. Use this guide to help you choose someone to confide. Download Resource Download Resource in Spanish
Getting the Right Start
A one-pager that makes taking the first steps to asking for help less overwhelming Download Resource
How to Help a Friend
A one-pager that gives suggestions on how to support a friend struggling with a mental health condition Download Resource
How Young Adults Can Seek Help
A video on where and how you can find the help and support you need for a mental health condition. Watch Video
How Teens Can Ask for Help
A video on who to reach out to and ways to put your thoughts and feelings into words to receive help for a mental health condition. Watch Video
NAMI On Campus Club
NAMI On Campus clubs are student-led, student-run mental health clubs for colleges and high schools. Learn more on how you can become a part of the national movement and make meaningful change on your campus. Download Resource Download Resource in Spanish Learn More
NAMI Say It Out Loud
Created by young people for young people, NAMI Say It Out Loud is a free online card game that will bring you closer to your friends through conversation prompts about life, relationships, and mental health. Play Now
NAMI Teen & Young Adult Resource Directory
NAMI HelpLine volunteers and staff have compiled this directory of outstanding resources to help teens and young adults identify resources to meet their mental health needs. If you or someone you know are in need, use this directory as a guide to help navigate through your mental health journey. Download Resource Directory NAMI does not endorse the resources included in the NAMI TYA HelpLine Resource Directory, and NAMI is not responsible for the content of or service provided by any of these resources.
Teen and Young Adult Mental Health Resources
A set of social media graphics to start a conversation with your community about mental health check-ins, mental health game plans and our four-day gratitude challenge. Download Resource Download Resource in Spanish Download Resource Graphics
Time Management
Use these tips to balance your school, work and personal time to help your mental well-being! Download Resource Download Resource in Spanish
College Students
Language Matters
A one-pager that helps individuals understand the importance of words when talking about mental health conditions and suicide Download Resource
Making A Mental Health Plan For College Students
In this video, learn how to prepare for a mental health emergency, including how to safely share medical information with someone you trust. Watch Video
Mental Health College Guide
Created in partnership with The JED Foundation, the College Guide is a one stop online resource to help young adults navigate the many situations encountered when in this new and exciting environment Learn More
Positive Coping Skills
Do you have a mental health toolkit? In this video, NAMI volunteer Britt shares what positive coping skills are and how to develop a mental health toolkit so that we don’t fall into negative coping strategies. Additionally, she discusses what specific skills help her cope. Watch Video
Setting Boundaries
Setting healthy limits, or boundaries, in our lives allows us to take care of our health and well-being. In this resource, we’ll cover different types of boundaries, how to set them and ways to communicate to others what you will and will not allow to protect yourself and take charge of your life. Download Resource Download Resource in Spanish
Social Media
Social media can be a great way to connect with friends, family and your community. Learn how to engage safely and protect your mental health. Download Resource Download Resource in Spanish
External Resources
National Institute of Mental Health (NIMH)
Digital Shareables on Child and Adolescent Mental Health
Resources from Alliance for a Healthier Generation
- Quality Time in No Time: Quick and Simple Ways to Make Family Time More Meaningful (Collaboration with Blue Star Families)
- Ways to Keep Active Together (Collaboration with President’s Council on Sports, Fitness & Nutrition, GoNoodle®️, and Griffin Middle School)
- How to Foster Self-Awareness when Challenging Emotions Arise (Collaboration with AAPI Youth Rising and Act to Change))
For Educators
Classroom Mental Health Contract
An activity guide to help students develop an understanding of mental health and identify supports available for them inside the classroom and at school. Download Resource Download Resource in Spanish
Five Questions for School Staff to Ask When Preparing for An Active Shooter Drill
Resources for building a trauma-informed active shooter drill in schools. Download Resource Download Resource in Spanish
A one-pager that helps individuals understand the importance of words when talking about mental health conditions and suicide. Download Resource
Mental Health & Wellness Moments for Educators
An activity guide for educators to incorporate daily wellness activities in the classroom to enhance the emotional well-being of their students. Download Resource Download Resource in Spanish
Mindfulness
Often, in school, students can find it hard to focus or can be impacted by events around them. You can use these exercises to bring students back into the moment. Download for Elementary Download for Middle & High Download Resource in Spanish
NAMI Ending the Silence
NAMI Ending the Silence is an engaging presentation that helps middle and high school aged youth learn about the warning signs of mental health conditions and what steps to take if you or a loved one are showing symptoms of a mental health condition. Learn More
NAMI Ending the Silence is offered in-person by NAMI affiliates across the country and is also now available online when an in-person presentation is not available.
School Mental Health Resource Poster
School Mental Health Resource Poster (black and white)Teachers can help students access vital mental health resources easily and confidentially with this convenient poster. Students can tear away important mental health resource information or scan the QR code to save contacts directly into their phones. NAMI recommends pre-cutting the tear aways at the bottom and tearing off the first one to relieve the pressure of any student being the first to take one. Download Resource Download in Black and White
Supporting Back to School Wellness
A one-pager with a few tips for teachers on how to make students’ transition back to the classroom a little bit easier during these uncertain times. Download Resource
The Three C’s for Educators
A one-pager with tips for educators on supporting their student’s emotional and mental well-being during the transition back to school and throughout the school year! Download Resource Download Resource in Spanish
Three Keys For a Successful Back-to-School Transition
Resources for educators to create a safe and supportive classroom. Download Resource Download Resource in Spanish
For Parents and Caregivers
10 Questions on a Tuesday
An activity guide for parents and guardians to discuss mental health and well-being with their children in the home and develop supportive practical strategies. Download Resource Download Resource in Spanish
Bullying Warning Signs
Bullying is a concern with children of all ages. Know how to spot the warning signs and how to start a conversation with your child about bullying. Download Resource Download Resource in Spanish
Creating Positive Change & Back to School Mental Health Tips
A nationwide iHeartRadio special, hosted by Ryan Gorman that includes Barbara Solish, director of youth and young adult initiatives at NAMI, discussing resources and help available for children, teens and young adults faced with the hardship of the pandemic and remote learning. The NAMI segment starts at minute marker 14:47. Listen Now
Crisis & Relapse Plan
Fill out this template to help your family and support team in the event of a crisis or relapse. Download Resource Download Resource in Spanish
Finding Mental Health Care for Your Child
A video that describes what to do and where to go for help when your child shows symptom of a mental health condition Watch Video
How To Be A Trusted Adult
An activity guide for parents and caregivers to explain who is a “trusted adult” and tips on how to become one. Download Resource Download Resource in Spanish
NAMI Basics
NAMI Basics is a six-session education program for parents, caregivers and other family who provide care for youth (ages 22 and younger) who are experiencing mental health symptoms. This program is free to participants, 99% of whom say they would recommend the program to others. NAMI Basics is available both in person and online through NAMI Basics OnDemand . Learn More
Suicide Warning Signs
Learn the warning signs, learn how to start a conversation and know what to do in a mental health crisis. Download Resource Download Resource in Spanish
The Three C’s for Parents and Guardians
A one-pager with tips for parents on supporting their children’s emotional and mental well-being during the challenging transition back to the classroom and throughout the school year! Download Resource Download Resource in Spanish
Week of Wellness for Parents/Caregivers and their Children
An activity guide for parents and caregivers to incorporate daily wellness activities at home to enhance the emotional well-being of their children. Download Resource Download Resource in Spanish

For Child Welfare Youth, Families and Staff
Behavior Is Communication: A Resource for Child Welfare Support Staff
We created this resource guide to better connect you with the young people you work with. Download Resource Download Resource in Spanish
Building Peer Relationships for Youth and Young Adults in the Child Welfare System
We created this guide to help anyone navigating trauma feel less alone. Here’s how you can safely begin to seek community. Download Resource Download Resource in Spanish
The Child Welfare System: A Guide to Trauma for Caregivers
We created this resource as a guide to help you reflect, re-establish and rebuild healing relationships with your child experiencing trauma as part of their experience in foster care. Download Resource Download Resource in Spanish
Statistics and Research
2020 Mental Health by the Number
A one-pager with data on the effects of the COVID-19 pandemic on youth and young adult. Download Resource
New CDC data illuminate youth mental health threats during the COVID-19 pandemic
CDC’s first nationally representative survey of high school students during the pandemic can inform effective programs. View Resource
Poll of Teen Mental Health from Teens Themselves (2022)
A poll conducted by Ipsos on behalf of NAMI finds that most teens are comfortable talking about mental health, but often don’t start the conversation. They also want schools to play a big role in their mental health, and they trust the information they get there, but feel like schools are not doing enough. Download Resource
Poll of Parents Amid the COVID-19 Pandemic (2021)
A poll conducted by Ipsos on behalf of NAMI finds that an overwhelming number of parents support mental health education in schools and “mental health days” for their children. Download Resource
Treatment For Suicidal Ideation, Self-Harm, And Suicide Attempts Among Youth
A guide that provides interventions to treat for suicidal ideation, self-harm and suicide attempts among youth. It provides research on implementation and examples of the ways that these recommendations can be implemented. View Resource
Youth Risk Behavior Survey: Data Summary and Trends Report 2009-2019
The Youth Risk Behavior Survey Data Summary & Trends Report: 2009–2019 provides the most recent surveillance data on health behaviors and experiences among high school students in the US related to four priority areas associated with sexually transmitted diseases (STDs), including HIV, and unintended teen pregnancy: sexual behavior, high-risk substance use, experiencing violence, and mental health and suicide. View Resource
Blogs and Videos
College Mental Health Blogs
Teen Mental Health Blogs
#Notalone Conversation: Heading Back to School
Sherman Gillums joins Ananya Venkatachalam (student), Shobhana Radhakrishnan (mom), and Jamie Meisinger (teacher) to discuss heading back to school after a year of at-home learning. This conversation opens the dialogue to realize the mental health challenges and opportunities for students, teachers and parents. Watch Video
What is PTSD?
Learn what PTSD (posttraumatic stress disorder) is, its causes, symptoms and treatment options. Watch Video

Know the warning signs of mental illness

Learn more about common mental health conditions
NAMI HelpLine is available M-F, 10 a.m. – 10 p.m. ET. Call 800-950-6264 , text “helpline” to 62640 , or chat online. In a crisis, call or text 988 (24/7).
Tips for Presenting to Young Audiences

It was my first year in business and I was 20-minutes into delivering a one-hour presentation skills seminar when it was becoming painfully clear that I was losing my audience fast. With this particular group, the early warning signs were all there…
It started with some subtle multi-tasking activity followed by a pronounced loss of eye contact by a few individuals at first and then half the group. If you’ve ever had that experience you know that you only have a couple of options at that point. You can try to pump up the energy level and occasionally re-energize an audience; but, let’s face it, the odds are pretty slim. Or you can always start summarizing, cut your loses and go for a well-scripted close. At least there’s some hope that your audience will, at a minimum, hear a few crisp closing points and an interesting story to tie it all together. On that particular day, I didn’t have a chance to do either. The bell rang at precisely 11:22 and Cheryl Bailey’s PowerPoint class darted for the door and I was left standing there (unplugging my projector and laptop) wondering what the heck just happened. It was my first time presenting to a group of kids and since then I’ve had to revise my technique considerably for this unique audience.
Lest you think these opportunities are pretty rare, you’d be surprised. Recently a client of mine was asked to be a keynote speaker for an audience of 300 high-achiever type high school kids. He had a track history of turning around troubled companies and had spent the last three years creating a nationally recognized direct marketing powerhouse from a once struggling east coast printing company. As we scripted his one-hour address, we came across the writings of Dr. Kenneth McFarland, an International Speaker’s Hall of Fame Award recipient and a strong advocate for the importance of sharing our very best thoughts with the youth of America. R.S Warn captured some of them in a paper called, ‘When Asked to Speak’. If you ever think you may be speaking to a group of kids (or perhaps are just wondering how to get through to your own), you will find these insights helpful as you attempt to communicate with today’s toughest audience.
Have the Right Frame of Mind
Speakers should approach a young audience with one very important understanding – young people are genuine. Young audiences openly express feelings where adults often pretend. When young people don’t like what’s being said, they will never act like they do. They are not naturally rude: they just refuse to pretend. This instant and honest feedback is a sterling quality in young audiences, a quality that some speakers avoid like the plague.
Ignore Their Masks
Shallowness, insincerity and callousness are masks young people wear, but rarely indicate who they really are. Our youth will appear untouched on the surface while deeply stirred by stories with human and emotional elements. They will also rally around basic ideals faster than the average adult audience. They do want to build a better world and are grateful for any relevant insights you may provide.
Make It Come Alive
A common error made by business speakers is the attempt to breathe life into a dead script (theirs or someone else’s). Unless your heartfelt feelings are involved, it is impossible to bring life to the words of another. Young people are not concerned with factual details of a letter-perfect manuscript, what they need to know is that the person standing before them is real. Hiding behind a script is a very fast way to lose them. The more of yourself you weave into the fabric of your speech the more “alive” it will become for them. When looking for ways to drive home a point, look for what you thought, what you found, what you felt, what you did and how you now feel. Inexperienced speakers, breaking every known rule of speech, have touched young people deeply by speaking from their heart.
Know You’re On Stage
This audience is sizing you up from the moment you arrive. When required to sit on stage or at a head table, know that everything you do either “adds to” or “detracts from” the value of the program. Pay full attention to the other speakers on the program as well. When this is not done, it tends to discredit the value of what’s being said. Kids can spot disrespect quickly and it will only impact their perception of you.
The True Power is in Simplicity
True power from the platform lies in using simple language to express meaningful ideas. Words are mental brush strokes we use to paint pictures in the minds of others. Uncommon and difficult words tend to leave people, especially youth, confused and insulted. A speaker overly impressed with a large vocabulary and insistent on demonstrating six syllable words is not a speaker at all, only a person who fills a room with confusing noise. (Noise that young people will always add to in very short order.)
Audience Participation
Audience participation helps hold the attention of young people. The younger the audience, the more important this device becomes. It can be as simple as a show of hands and as involved as your time, talent and ability contributed before and after the event. A participation device needs to tie directly with a major point in your message, however. Where this is not done, your audience becomes sidetracked. When asking group questions from youth, you can expect questions that adults would never ask. (How much do you make? How many hours do you work? Have you ever fired anyone?) Whatever the question, they must be handled as an important question and treated with respect.
Never Talk Down
They may lack wisdom that comes with maturity, but the average high school audience of today is better informed than they’ve ever been before. Young people watch the evening news and are often more in tune with worldwide problems than some adults. Any speaker who stands before them with an attitude of being all wise will lose this audience in the first 60-seconds. Our young people encounter so much condescending speech in their daily lives that they naturally assume any adult who steps before them will deliver the same. You need to break that perception quickly.
Never Attempt to Be One of Them
The only way you can become like a child again is to become senile and these young people know it. When you earn their respect, they will accept you as an adult, but they will never accept you as one of them. Any attempt to be one of them, just one of the gang, will backfire in your face. Everything you do, your dress, actions and words should aim to project an image of an adult, the type of adult they may want to become.
I’ve only hit the highlights from Dr.McFarland’s insights and I’ve thrown in a few of my own. From these pearls of wisdom, one thing is clear, the need to be genuine is never as important as it is with youthful audiences. What kids are looking for is often very different than what we may think. As the father of some great kids, I found some basic wisdom here as well. We rarely understand at the time how our words impact young hearts and minds. And as indifferent as they may seem at times, they desperately want to find adults in their lives who they can look up to and model.
Young people may be one of today’s toughest audiences, but there will never be any more important.
Written by Jim Endicott
Recommended Pages

Hi, I’m from Singapore and I frequently give talks on estate planning. Just last week, my audience was a group of financial advisers mostly in their mid to late 20s. As a 60-year old seasoned presenter, I appeared at the talk without preparing how to I should be presenting to a young audience. I went through my usual “humorous” examples that I’ve used on a mature audience, used technical terms that could have been avoided and tried to sound more animated than usual. Well as you can imagine, half of them started yawning and playing with their cell phones after 10 minutes. I wish I had come across your excellent article before! Thank you for a very welcome wake up call!
- All Templates
- Persuasive Speech Topics
- Informative
- Architecture
- Celebration
- Educational
- Engineering
- Food and Drink
- Subtle Waves Template
- Business world map
- Filmstrip with Countdown
- Blue Bubbles
- Corporate 2
- Vector flowers template
- Editable PowerPoint newspapers
- Hands Template
- Red blood cells slide
- Circles Template on white
- Maps of America
- Light Streaks Business Template
- Zen stones template
- Heartbeat Template
- Web icons template
VentureLab Blog » Entrepreneurship Education Articles
11 Public Speaking Tips for Youth (and Adults!)
- December 6, 2021
Public speaking is an essential skill for entrepreneurship and beyond, but for many, it’s a source of anxiety. However, with consistent practice and applying specific techniques, anyone can become more confident sharing their ideas with any audience!
We’ve compiled a list of public speaking tips that can help both youth and adults become more confident, persuasive speakers.
Public Speaking Tip 1: Composure
Even professional public speakers get nervous! It’s normal to be anxious or worried and have lots of adrenaline flowing. Take two deep breaths. Practice what you’ll say in your head and go for it! Watch Sage master his composure (and remember to stop and breathe at 30 seconds) to deliver a wonderful pitch:
Public Speaking Tip 2: Body Language
Body language can make a big difference in how your message is perceived. Sit/stand up straight. Use your hands as you talk (but not too much) and avoid crossing your arms. Maintain eye contact with your audience to establish connection, trust, and show confidence .
Public Speaking Tip 3: Speed
Pay attention to how quickly or slowly you are speaking. Effective speakers talk at a pace that makes it easy for the audience to understand what they’re saying. Consider recording yourself and listening back to your speech; you may be surprised by how fast you talk!
Effective speakers talk at a pace that makes it easy for the audience to understand. As you practice, try recording yourself and listening back to your speech; you may be surprised by how fast you talk! Tweet this
Public Speaking Tip 4: Volume
Pay attention to how loud or soft you are speaking. Effective speakers talk at a volume that makes it easy for the audience to hear what they’re saying but avoid shouting. It’s okay to vary your volume , too. (See Tip 5!)
Public Speaking Tip 5: Emphasis
Pay attention to what words you are emphasizing when you speak. Effective speakers draw attention to important words and phrases, which makes your speech more interesting and compelling! Be sure to slow down and emphasize your business name.
Public Speaking Tip 6: Pausing
Pay attention to when you are taking a break to pause. Effective speakers take time to collect their thoughts and leave room for moments of quiet. It’s always okay to stop and take a breath as you need it, too.
Effective speakers take time to collect their thoughts and leave room for moments of quiet. It's always okay to stop and take a breath as you need it, too. Tweet this
Public Speaking Tip 7: Active Listening
Effective speakers are also active listeners! Face the speaker and make eye contact, nod, and smile when appropriate to acknowledge what is being said. Resist the urge to interrupt!
Public Speaking Tip 8: Practice, Practice, Practice!
The best way to get used to implementing all of the public speaking tips above? Practice! This doesn’t have to be formal. Record yourself practicing on your phone or laptop, then watch it back and consider how you’ve applied the tips. Practice in front of family, friends, or the mirror! The more you practice, the easier public speaking becomes.
Public Speaking Tips for Virtual Presentations
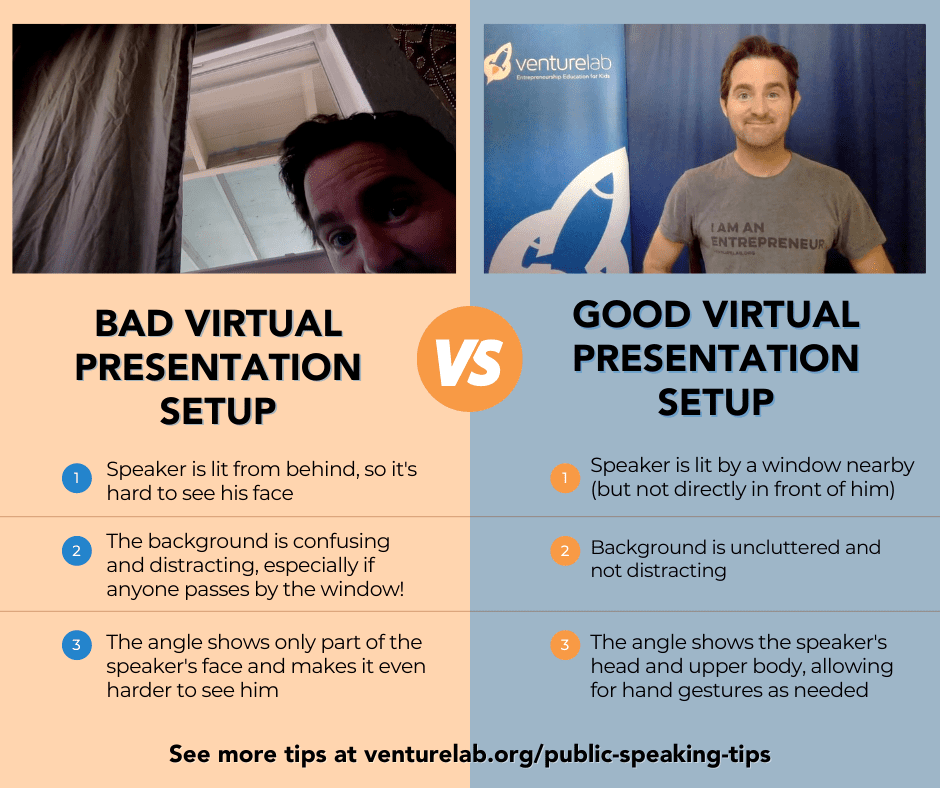
Virtual Public Speaking Tip 1: Background
Pay attention to what is going on in your background. Effective speakers create a background setting that isn’t distracting . Even a plain wall can work as a perfect setting for viewers to focus on you and not your background!
Virtual Public Speaking Tip 2: Lighting
Poor lighting can make it hard for others to work on your message! Position yourself near a window or other light source so that your face is clearly lit. Avoid sitting with your back to a window, which can cause your image to become too dark to see. Test your lighting ahead of virtual presentations so you’re ready when it’s time!
See an example of a fantastic pitch with great lighting (and camera positioning):
Virtual Public Speaking Tip 3: Camera Positioning
Pay attention to what parts of you appear on screen. Make sure your entire face can be seen. (If you can, include your shoulders, too!) Elevate your device so the camera is eye level. Putting your laptop on top of a few books can do the trick.
Help your youth practice public speaking!
Looking for more youth entrepreneurship.
Sign up for our monthly resource email to receive activities, tips, and more right to your inbox. It’s easy and free!
Related blogs:

Printable Entrepreneurial Mindset Cards

3 Reasons to Bring Entrepreneurship to Summer Learning

VentureLab’s May 2023 Youth Pitch Event Recap and Replay

Three strategies to make your classroom entrepreneurial AND run smoothly

STARBASE Robins Summer Camps brings STEM and entrepreneurship to life for Georgia youth

The Impact of Youth Entrepreneurship Education in Houston with VentureLab and BakerRipley
Recent posts, ready, set, startup was a success, how to plan youth entrepreneurship events for success, venturelab celebrates national mentorship month with a spotlight on spark 2023 graduates, related posts.

We're on a mission to create the next generation of diverse innovators and changemakers by making entrepreneurship education accessible to ALL youth.
Get involved.
© COPYRIGHT 2024 VENTURELAB, A 501 (C)(3) NON-PROFIT | Website developed by iNNOV8 Place | Powered by Electric Oak | Privacy Policy | License Agreement
Pin It on Pinterest

An official website of the United States government
The .gov means it's official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- Browse Titles
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Committee on Improving the Health, Safety, and Well-Being of Young Adults; Board on Children, Youth, and Families; Institute of Medicine; National Research Council; Bonnie RJ, Stroud C, Breiner H, editors. Investing in the Health and Well-Being of Young Adults. Washington (DC): National Academies Press (US); 2015 Jan 27.

Investing in the Health and Well-Being of Young Adults.
- Hardcopy Version at National Academies Press
2 Young Adults in the 21st Century
This chapter provides a foundation for the remainder of the report. It summarizes current knowledge regarding young adulthood as a critical developmental period in the life course; highlights historical patterns and recent trends in the social and economic transitions of young adults in the United States; reviews data on the health status of the current cohort of young adults; briefly summarizes the literature on diversity and the effects of bias and discrimination on young adults' health and well-being; presents the committee's key findings and their implications; and enunciates several key principles to guide future action in assembling data, designing research, and formulating programs and policies pertaining to the health, safety, and well-being of young adults. Many of the topics summarized in this chapter are discussed in greater depth in subsequent chapters.
- BASIC PATTERNS OF DEVELOPMENT
Biologically and psychologically, young adulthood is fundamentally a period of maturation and change, although the degree of change may seem less striking than the changes that occurred during childhood and adolescence. As just one example, the physical changes of the transition from childhood into adolescence are transformative, with bodies growing in dramatic bursts and taking on secondary sex characteristics as puberty unfolds. As young people move from adolescence into adulthood, physical changes continue to occur, but they are more gradual. Individuals begin the steady weight gain that will characterize adulthood, but these changes are not as discontinuous as they are at the beginning of adolescence ( Cole, 2003 ; Zagorsky and Smith, 2011 ).
In some ways, the tendency for the developmental change that happens during young adulthood to be gradual instead of dramatic may have led to the devaluation of young adulthood as a critical developmental period, but that developmental change should be not be underestimated. It is integral to transforming children and adolescents into adults. The psychological and brain development that occurs during young adulthood illustrates this point.
Psychological Development
Over the past two decades, research has elucidated some of the key features of adolescent development that have made this period of the life course unique and worthy of attention. These insights, in turn, have helped shape policy in major ways. These adolescent processes, and the increasing scientific and public attention they have received, provide a reference point for understanding the developmental importance of young adulthood.
In general, adolescence is a complex period characterized by substantial cognitive and emotional changes grounded in the unfolding development of the brain, as well as behavioral changes associated with basic psychosocial developmental tasks. In particular, adolescents are faced with the task of individuating from their parents while maintaining family connectedness to facilitate the development of the identities they will take into adulthood. At the same time, the overactive motivational/emotional system of their brain can contribute to suboptimal decision making ( Crosnoe and Johnson, 2011 ). As a result, many adolescents tend to be strongly oriented toward and sensitive to peers, responsive to their immediate environments, limited in self-control, and disinclined to focus on long-term consequences, all of which lead to compromised decision-making skills in emotionally charged situations ( Galván et al., 2006 ; Steinberg et al., 2008 ). This combination of characteristics is implicated in the heightened rates of risky behaviors and accidental death among adolescents (and young adults) relative to childhood and later stages of life, and awareness of these issues has reshaped policy responses to adolescent behavior in general and crime in particular (as described in the National Research Council [2013] report on juvenile justice).
Clearly, much social, emotional, and cognitive maturation needs to occur before adolescents are capable of taking on adult responsibilities and their many behavioral risks decline to adult-like levels. The ongoing development that occurs during young adulthood is what marks the transition from adolescence to adulthood. Again, this development is not necessarily discontinuous (such as the notable surge in risk taking that occurs during the transition from childhood into adolescence), but instead, it takes a more gradual and linear form, less obvious perhaps but no less important. Although findings from studies that directly compare adolescents and young adults on various cognitive tests and decision-making tasks are by no means uniform, the available research documents the slow and steady progress in self-regulation and related psychological capacities that takes place as adolescents transition into their 20s (see Cauffman et al., 2010 ). Compared with adolescents, young adults
- take longer to consider difficult problems before deciding on a course of action,
- are less influenced by the lure of rewards associated with behavior,
- are more sensitive to the potential costs associated with behavior, and
- have better developed impulse control.
In other words, the differences between adolescents and adults are stark, and the years between 18 and 26 are when young people develop psychologically in ways that bridge these differences. This development reflects many things, including the opportunities young people have to take on new roles and responsibilities and changes in their social contexts. It also reflects the similar gradual development of their brains.
Brain Development
The process of structural and functional maturation of the brain through adolescence to adulthood has garnered a great deal of attention, as neurobiological processes are believed to stabilize before declining with age. Maturation is of particular interest given the role of plasticity in affording opportunities for specialization, but also posing risks for abnormal development. Developmental neuroscientists, however, have traditionally assumed that adulthood is reached by age 18—hence the predominance of neurodevelopmental studies that compare children (under age 12) and adolescents (approximately 12-17) with adults (18-21 or extending and averaging through the mid-20s to the 30s). This approach has revealed many immaturities during the adolescent period, but much less is known about young adulthood. Discussions recently have emerged of the possibility of a prolonged brain maturational trajectory through young adulthood, as described below. Although the most significant qualitative changes in brain maturation have been found to occur from childhood to adolescence, emerging evidence does suggest that specialization of brain processes continues into the 30s, supporting both cognitive and motivational systems.
The primary mechanisms underlying brain maturation through adolescence into adulthood are synaptic pruning, myelination, and neurochemical changes. Synaptic pruning refers to the programmed elimination of synaptic connections between neurons believed to support specialization of brain processes based on experience. After a proliferation of synaptic connections through childhood, when the gray matter thickens, a decline in synaptic connections occurs through adolescence ( Petanjek et al., 2011 ) and is believed to contribute to the thinning of gray matter that proceeds through adolescence ( Gogtay et al., 2004 ). Magnetic resonance imaging (MRI) studies, which provide in vivo measurements of gray matter thickness, have focused predominantly on immaturities during adolescence and have considered adulthood to be established by the early 20s ( Gogtay et al., 2004 ). MRI studies that sample a wider age range, however, indicate a prolonged period of gray matter thinning of prefrontal cortex that persists through the third decade of life ( Sowell et al., 2003 ; see also Figure 2-1 ). Similar maturational trajectories have been observed in human postmortem studies that indicate a continued decrease in synaptic connections in the prefrontal cortex into the 30s ( Petanjek et al., 2011 ). The prefrontal cortex is the region that supports abstract reasoning and planning. Through its extensive connectivity throughout the brain, it also supports executive function, providing control and modulation of behavior ( Fuster, 2008 ). It plays a major role in decision making, and its maturation is believed to support cognitive development ( Fuster, 2002 ; Luna, 2009 ).
Continued maturation of prefrontal cortex through young adulthood evidenced from (A) in vivo MRI results showing thinning of cortical gray matter in prefrontal cortex and (B) postmortem evidence showing continued loss of synapses in prefrontal cortex (more...)
Notably, despite continued specialization in the prefrontal cortex through the 20s, its engagement during executive tasks can appear adult-like as early as adolescence. Functional MRI (fMRI) studies of executive control through adolescence report both greater and lesser engagement of lateral prefrontal regions known to play a primary role in executive function ( Luna et al., 2010 ). A recent longitudinal study was able to characterize developmental changes in core cognitive components of the ability to suppress impulsive responses by measuring the ability to stop a reflexive eye movement ( Ordaz et al., 2013 ). Results suggest a decrease in prefrontal engagement through childhood stabilizing by adolescence. However, recruitment of the anterior cingulate cortex, a medial prefrontal region that is distinct from other prefrontal regions in supporting performance monitoring and error processing, increases during executive function processing through adolescence and young adulthood ( Ordaz et al., 2013 ). These results suggest that processes distinct from prefrontal executive function that support monitoring behavior underlie cognitive development and continue to mature through young adulthood. The implication is that by young adulthood, prefrontal executive processes are at adult levels, but processes involved in monitoring behavior are still improving, which may affect decision making.
In addition to the maturation of prefrontal systems that support executive function, motivational and emotional brain systems in limbic areas show a protracted development through adolescence and young adulthood. The striatum is a limbic region rich in dopaminergic innervation. Dopamine is the neurotransmitter that supports motivation and reward processing ( Cools, 2008 ). Through its connectivity with prefrontal systems, it provides motivational modulation of behavior. MRI studies indicate that the striatum peaks in gray matter growth at an even later time than cortical regions through adolescence ( Raznahan et al., 2014 ; Sowell et al., 1999 ; Wierenga et al., 2014 ). In addition, animal studies suggest a peak in the availability of dopamine, believed to play a role in increased sensation seeking beginning in adolescence ( Padmanabhan and Luna, 2013 ; Spear, 2000 ; Wahlstrom et al., 2010 ). fMRI studies typically show a peak of increased recruitment of the striatum during monetary reward tasks in adolescence that decreases through young adulthood ( Galván et al., 2006 ; Geier et al., 2010 ; van Leijenhorst et al., 2010 ). In particular, the presence of peers has significant salience in adolescence, engaging the reward circuitry to affect decision making ( Chein et al., 2011 ). The trajectory of changes in reward processing through young adulthood, however, has not been directly investigated and in fact some studies have used young adults to represent all adults ( van Leijenhorst et al., 2010 ). It is possible that developmental declines in striatal activity in response to rewards may be lower in young adulthood than in adolescence but still be greater than in later adulthood. Similarly, the amygdala, which supports emotional processing, has a peak in gray matter growth in the teen years, with a subsequent decrease in volume ( Greimel et al., 2013 ; Scherf et al., 2013 ). The amygdala shows greater functional reactivity to emotional stimuli in adolescence ( Blakemore, 2008 ; Hare et al., 2008 ), which may persist through young adulthood. Animal studies indicate that white matter fibers between the amygdala and cortex continue to increase into young adulthood ( Cunningham et al., 2002 ). Despite this increase in structural connectivity, however, human neuroimaging indicates decreased functional connectivity into young adulthood, suggesting developmental increases in regulatory development with regard to the effects of emotion processing on behavior ( Gee et al., 2013 ).
In parallel with decreases in gray matter in prefrontal and striatal regions are increases in white matter brain connectivity, which supports the ability for prefrontal executive systems to modulate reward and emotional processing. Postmortem studies indicate continued myelination—insulating of white matter connections—through adolescence and adulthood throughout cortical regions, including prefrontal systems ( Lebel et al., 2008 ). Diffusion tensor imaging, which measures the integrity of white matter connections in vivo, indicates a hierarchical maturation of white matter, with tracts connecting cortical and limbic regions showing protracted development through adulthood ( Lebel et al., 2008 ; Simmonds et al., 2013 ). During childhood to adolescence, a peak in white matter growth occurs throughout the brain, with continued growth of tracts as they reach cortical and limbic gray matter in young adulthood ( Simmonds et al., 2013 ). Last to mature are the cingulum and uncinate fasciculus, which provide connectivity between cortical and limbic regions. The cingulum integrates dorsal frontal cognitive (e.g., anterior cingulate supporting performance monitoring) and limbic regions supporting emotion processing that continue to mature through the early 20s ( Simmonds et al., 2013 ). The uncinate fasciculus, which integrates ventral frontal cortical (e.g., orbitofrontal cortex supporting motivation), amygdala (supporting emotion), hippocampus (supporting memory), and temporal cortical regions that form a circuit underlying socioemotional processing, continues to mature through the 20s ( Simmonds et al., 2013 ). During young adulthood, therefore, connectivity that supports socioemotional processing is still immature but developing compared with later adulthood.
Within these maturation processes are unique gender differences that emerge in adolescence, are believed to be associated with earlier puberty in girls than in boys, and continue to dissociate through adulthood ( Dorn et al., 2006 ; Ordaz and Luna, 2012 ). Young men have larger total brain volume, females show earlier cortical thinning and maturation of white matter integrity ( Lenroot et al., 2007 ; Simmonds et al., 2013 ), and males show greater change in limbic regions ( Giedd et al., 1997 ; Raznahan et al., 2014 ). These differences are believed to underlie gender differences in the emergence of different psychopathologies, including female predominance of depression and male predominance of antisocial personality disorders.
Taken together, the evidence demonstrates continuing maturation of limbic systems supporting motivation and reward processing and prefrontal executive systems. It has been proposed that the relative balance of maturation of motivational systems and prefrontal executive processing underlies the adolescent sensation seeking already discussed ( Ernst et al., 2006 ; Smith et al., 2013 ; Somerville and Casey, 2010 ). In young adulthood, this imbalance diminishes but is still present. Brain systems supporting motivational and socioemotional processing are still maturing in young adulthood, influencing a more developed prefrontal executive system capable of more sophisticated and effective planning and resulting in unique influences on decision making, such as adaptive choices or risk-taking behavior. Overactive motivational systems may drive adult-like access to cognitive systems, resulting in planned responses that are driven by short-term rewards. Indeed, greater sensation seeking often persists into the mid-20s. This profile of decision making may also affect the attention given to choices regarding health, profession, and relationships, which are addressed in this and later chapters.
The Developmental Bottom Line
Overall, critical developmental processes clearly occur during young adulthood. Initial findings suggest that mature aspects of executive functioning are paired with continuing increased motivational/emotional influences affecting decision making. Still, more work is needed to fully understand young adulthood as a biologically and psychologically distinct and critical period of development and to relate these neurological changes to behavioral and social changes that typically occur during this period. Although these processes of maturation may sometimes appear as limitations on optimal decision making in young adulthood, the enhanced motivational processing that also occurs during this period plays an important adaptive role in supporting optimal learning and the ability and impetus to explore the environment and novel experiences.
- HISTORICAL PATTERNS OF SOCIAL ROLES AND ACTIVITIES
The important psychological development experienced by young adults has not changed dramatically across generations, but their social functioning has ( Steinberg, 2013 ). Social and behavioral scientists frequently discuss such social functioning in terms of five major role transitions of young adulthood—leaving home, completing school, entering the workforce, forming a romantic partnership, and transitioning into or moving toward parenthood ( Schulenberg and Schoon, 2012 ; Shanahan, 2000 ). The focus on these social roles as the benchmark against which young adults from diverse segments of the population are compared can be critiqued as classist, ethnocentric, and heteronormative. These critiques certainly need to be acknowledged, but these role transitions do provide a useful structure for organizing the present discussion of young adulthood in the United States, especially if the significant diversity in these transitions among U.S. youth—both historically and in the contemporary era—is highlighted.
Two basic concepts—the timing and the sequencing of role acquisition—capture how the transition to these adult roles is taking more time and becoming more unpredictable ( Settersten and Ray, 2010 ).
First, the timing of role acquisition in young adulthood is changing. In the long view, today's U.S. young adults are taking less time to undergo these role transitions relative to young adults in the distant past. Relative to more recent cohorts, however, they are taking more time. The timing of role acquisition is affected by, among other things, economic development and state investments that impose various signifiers of life transitions, such as legal rules on when youth are granted various privileges and allowed to enter certain statuses or, alternatively, when they age out of services or other protections ( Modell et al., 1976 ; Shanahan, 2000 ).
Second, the sequencing of role acquisition (i.e., the order in which various roles are assumed) also is changing. Configurations of young adult statuses may change across cohorts. Recently, more diverse combinations of statuses have led to a “disordering” of the transition into adulthood, a term that seems pejorative but is not bad or good per se. The sequence of the roles assumed in the transition to adulthood increasingly is shaped by individual choices and actions rather than social structures. As discussed below, for example, young people partner and parent in different sequences because they have the freedom to do so now that the social stigma of nonmarital childbearing has diminished, and because economic or policy factors make various sequences more appealing and feasible than they used to be ( Fussell and Furstenberg, 2005 ; Lichter et al., 2002 ; Rindfuss et al., 1987 ).
Family Roles
For many young adults, a major event is leaving the parental home to reside independently or with others of the same age. In some ways, leaving home is a rite of passage, which is why one main topic of interest concerning modern young adults in general and young adults during the Great Recession in particular is “boomerang” children—young adults who leave home to live independently but come back to reside with their parents ( Stone et al., 2013 ). In truth, young adults living with their parents 1 in moderate to large numbers is not a new phenomenon in the United States or in other industrialized societies, and doing so is not inherently problematic or beneficial. In the United States, 32 percent of young adults aged 18-31 lived at home with their parent(s) in 1968, in 1981 31 percent did, and in 2012 36 percent did ( Fry, 2013 ). How people assess young adults living with their parents instead of with peers or alone often reflects how they perceive (or misperceive) the past, including their own personal histories ( Settersten and Ray, 2010 ; Stone et al., 2013 ).
Beyond leaving the parental home, many other noteworthy family events occur in the lives of today's young adults. In assessing the historical relevance of these contemporary patterns, one must keep in mind the importance of the comparison point. As with leaving home, contemporary young adult behaviors and statuses often seem so striking because they are viewed in the context of the post–World War II era, especially the 1950s. This era, however, was something of a historical outlier. What is going on today with young adults—especially in relation to family roles and responsibilities—appears to be less divergent, although still divergent, when compared against the full scope of the 20th century ( Coontz, 2000 ).
Partnership and parenting are the core of family formation in the United States (see Chapter 3 ). How partnership is defined and how it connects to parenting have both evolved considerably in recent decades. Traditionally, partnership was defined in formal (i.e., legal) terms as marriage, especially among the white middle class. Today, partnership in young adulthood is most often viewed as a sequence from cohabitation—living with a romantic partner—to marriage (a transition from an informal to a formal partnership widely recognized by laws) or just as cohabitation itself. While most young Americans see cohabitation as a precursor to marriage, this has not always been the case. Many immigrant families from Latin America, for example, have a long tradition of cohabitation as a form of marriage, but the practice of cohabitation as a step toward marriage is new for most groups ( Cherlin, 2009 ).
Figure 2-2 shows the percentages of young adults having engaged in at least one of three family formation behaviors—cohabitation, marriage, and parenting—by age 25 by gender, race/ethnicity, and level of education (high school or college graduate). In total, just under two-thirds of young adults have made at least one of these three family role transitions by age 25 ( Payne, 2011 ). This proportion, however, fluctuates across the population. A larger proportion of women than men have made at least one of these role transitions (69 percent versus 53 percent), and family formation is less common among young adults who are white (59 percent) than among those who are not (66 percent for African Americans and 64 percent for Latino/as). There is also an educational gradient to family formation in young adulthood, with family role transitions becoming less common as educational attainment rises. Indeed, college graduates are the only segment of the population in which less than a majority of young adults have made at least one of the three family role transitions. Of these three transitions, the most common is cohabitation (47 percent), followed by becoming a parent (34 percent) and marrying (27 percent) ( Payne, 2011 ).
Percentage of young adults in the United States with at least one family formation behavior by age 25. NOTE: The dotted line represents the overall sample average (61 percent). SOURCE: National Longitudinal Study of Youth 1997 (see Payne, 2011).
One important caveat to keep in mind when considering these family formation patterns is that historically, tracking the family formation behaviors of lesbian, gay, bisexual, and transgender (LGBT) people has been exceedingly difficult. Because sexual relations between people of the same gender were outlawed in many states until recently, identifying the LGBT population was a challenge. Only within the past decade have same-sex couples been legally allowed to marry, and they may do so even now only within a minority of states (although the number is growing quickly). Thus, many LGBT young adults would have been classified as cohabiting in the past simply because they were legally barred from marrying. Moreover, innovations in reproduction technology and changes in adoption laws (domestically and internationally) have enabled these young adults to become parents without having to engage in an opposite-sex partnership before entering a same-sex partnership—long the most common path to parenthood for gays and lesbians. In states where same-sex marriage is legally recognized, same-sex parents are demonstrating patterns of union formation (and dissolution) similar to those of opposite-sex parents ( Hunter, 2012 ; Parke, 2013 ; Seltzer, 2000 ).
In terms of timing, family formation is clearly showing signs of becoming a longer-term process. In short, young adults are taking more years to partner and become parents than they did in the past, especially compared with the last half of the 20th century. Today, the median age at first marriage—the age by which half of the population has married—is just under 27 for women, a nearly 5-year increase over the past 30 years and extending beyond the 18-26 age range used to define young adulthood in this report ( Arroyo et al., 2013 ). A similar trend has occurred among men, although their median age at marriage has consistently been a year or so higher than that of women. This trend often is discussed in terms of “delay,” but it is better thought of as part of the prolonged family formation process overall. As Americans live longer, they take more time to reach life-course milestones such as marriage. The transition to parenthood also tends to occur later in the life course, although the increase in median age at first birth over the last three decades has been less pronounced than the increase in median age at first marriage—about 3 years rather than 6 and just within our focal 18-26 age range ( Arroyo et al., 2013 ).
These differences in the magnitude of the age increase in major family role transitions also speak to sequencing, or the growing tendency for transitions to cluster in heterogeneous ways. For most of American history (especially among the white middle class), marriage preceded parenthood. Yet the lesser increase in age at first birth compared with age at first marriage resulted in the two trends eventually converging (in 1991, to be precise). Since that point, median age at first marriage has been older than median age at first birth ( Arroyo et al., 2013 ). The sequence (or order) of these transitions has become less predictable.
Breaking down partnerships into cohabitation and marriage when discussing major family role transitions of young adulthood also reveals evidence of changing sequencing. In line with the increasing prevalence of cohabitation in the population at large, the proportion of young adults who have cohabited by the age of 25 (47 percent) is higher than the proportion of young adults who have married (27 percent) ( Payne, 2011 ). Three-fifths of all young adults who are married cohabited first, lending credence to the idea that cohabitation is now the modal pathway to marriage. Furthermore, one-third of young adults with children became parents before marrying or cohabiting. Just as with overall family formation patterns, these specific family patterns differ by gender, race/ethnicity, and educational attainment. For example, marriage without cohabitation is more common among whites and college graduates, but becoming a parent without partnering is far less common in these same two groups ( Payne, 2011 ).
Overall, young adults (including LGBT young adults) in the United States are taking more time before entering into family roles that have long defined adulthood compared with their parents and grandparents, and they are sequencing these roles in multiple ways. This is particularly true for youth from white middle-class backgrounds.
Socioeconomic Roles
The transition from student to worker is a defining feature of young adulthood, given that Americans widely view financial independence from parents as a marker of becoming an adult. Yet young people are taking longer to become financially independent, and their school-work pathways are becoming more complex ( Settersten and Ray, 2010 ). As with family formation, changes have been occurring in the timing and sequencing of the socioeconomic aspects of young adult role transitions. Chapter 4 gives a detailed accounting of how young people are faring in the educational system and in the labor market, but we highlight a few patterns in school-to-work transitions here in the context of the overall importance of studying young adults today.
Beginning with education, more young adults than in the past have been entering higher education in recent decades, but they are participating in higher education in many different ways and following diverse pathways ( Fischer and Hout, 2006 ; Goldin and Katz, 2008 ; Patrick et al., 2013 ). According to data from the National Longitudinal Study of Youth, in the United States, 59 percent of young adults have enrolled in some form of higher education by the time they reach age 25 ( Payne, 2012 ). The overwhelming majority enrolled right after leaving high school, around age 18. Of those who enrolled, 33 percent enrolled in 2-year colleges and 44 percent in 4-year colleges and universities, with the remainder enrolling in both ( Payne, 2012 ).
Of course, enrollment is not the same as graduation. The reality is that many young adults who enroll in higher education fail to earn a degree, at least while they are still young adults. Indeed, rates of completion of higher education in the United States have declined even as rates of enrollment have increased ( Bailey and Dynarski, 2011 ; Bound et al., 2010 ), at least in part because enrollment rates have risen over time among those with less academic preparation in the K-12 years.
As with family role transitions, higher education patterns vary considerably across diverse segments of the population ( Brock, 2010 ). Enrollment rates in both 2- and 4-year colleges are higher for women than for men and for whites than for nonwhites ( Holzer and Dunlop, 2013 ; Payne, 2012 ). In fact, enrollment figures are at about 50 percent for African American and Latino/a young adults by the time they reach age 25 (compared with the population figure of 59 percent noted above), with even greater gender differences within these groups ( Payne, 2012 ). The starkest disparities across these groups appear in graduation rates from 4-year colleges and universities, with women earning more bachelor's degrees than men and whites earning more bachelor's degrees than minorities ( Payne, 2012 ). There are also growing disparities in educational attainment between young adults from poor and middle/upper-income families.
Thus, modal or average patterns of higher education enrollment and completion during young adulthood typically subsume a great deal of heterogeneity. This heterogeneity is clearly evident in the growing immigrant population, as many first- and second-generation immigrants have rates of college enrollment and graduation higher than those of the general population, while other immigrant groups (e.g., unauthorized immigrants, the children of Mexican immigrants) are significantly underrepresented in higher education ( Baum and Flores, 2011 ).
Turning to employment, the increased enrollment of young adults in higher education has had a major impact on employment rates, as educational commitments often preclude substantial work commitments. Yet even taking into account the substitution of education for employment in the late teens and early 20s, a key feature of the employment status of young adults is unemployment, or being out of work when one wants to be working. Indeed, the unemployment rate for the under-25 population is twice that of the general population ( Dennett and Modestino, 2013 ). This elevated unemployment among young adults is not altogether new; they have always struggled more than older adults to find and hold onto jobs. Still, this age-related disparity in unemployment has been growing in recent decades, and it has become especially marked since the start of the Great Recession in late 2007. Across all education levels and school enrollment statuses, young adult unemployment has increased significantly in the last several years relative to pre-recession years ( Dennett and Modestino, 2013 ). Furthermore, among those who obtain jobs, many earn considerably less than similar demographic groups did in the past.
Another school-work scenario is “idleness”—when young adults are neither enrolled in higher education nor employed for pay. Many idle young adults are not just unemployed but have dropped out of the labor force altogether, sometimes for very long periods of time, in response to the lower wages and benefits now available to those with high school or less education, especially among young men ( Dennett and Modestino, 2013 ). As discussed in Chapter 4 , rates of idleness and labor force nonparticipation tend to be higher (and are becoming more so) for young African American men, who have been hit harder than other groups by broad changes in the economy and the labor market ( Dennett and Modestino, 2013 ). Their lack of employment activity often becomes reinforced over time if they have a criminal record or if they are in arrears on child support they have been ordered to pay as noncustodial parents.
The sequencing of education and employment in young adulthood also is changing in important ways. A traditional school-work path was college enrollment and graduation in the late teens and early 20s, followed by full-time entry into the labor market in the mid-20s (with some pursuing more education and pushing back full-time employment). This primarily unidirectional path is related to higher economic returns throughout adulthood. Another traditional path was bypassing higher education altogether to enter the labor market directly after secondary schooling, a path related to higher earnings than those of other young adults in the short term but lower earnings in the long term.
In the contemporary economic climate of stagnant or lower real wages and generally higher costs of financing education (despite the rising availability of federal Pell grants to help low-income students pay for college), more young adults are trying to participate in higher education and employment at the same time or moving back and forth between the two. These mixed or bidirectional paths—which tend to be more common among young adults from more socioeconomically disadvantaged backgrounds—are one of several explanations for the lower odds of completing higher education among low-income or minority students ( Bernhardt et al., 2001 ; Goldin and Katz, 2008 ).
Overall, young adults in the United States are attempting to gain more education, and more education improves employment prospects during young adulthood and beyond (not to mention affecting many nonemployment outcomes, such as civic engagement; see Chapters 4 and 5 ). Yet an unstable economic context and the high immediate costs of financing higher education mean that the process of gaining human capital to improve future job prospects and realize other benefits of education is not so simple, especially for some young adults from more disadvantaged socioeconomic and racial/ethnic groups.
Young adults' successes or failures in education and employment are integrally linked to their health. In general, the more educated a young adult becomes, the healthier she or he will be in adulthood, whereas lower educational attainment and occupational success is associated with poor health status, and involuntary loss of employment can have a negative impact on both physical and behavioral health. But the causal direction is also reversed in many cases: young adults with disabilities and chronic health conditions may find it significantly more difficult to obtain higher education and employment.
- SOCIAL/ECONOMIC CHANGES AND THE REFASHIONING OF YOUNG ADULTHOOD
General physical and psychological development and the transition to major family and socioeconomic roles are personal experiences of individual young adults. Yet how these developmental and social processes unfold—and their timing and sequencing—is shaped by broader societal and historical forces ( Shanahan, 2000 ). In other words, what is happening among young adults today reflects the larger context in which they find themselves, through no choice or fault of their own.
First, the U.S. economy has undergone substantial restructuring over the last several decades in ways that have radically altered the landscape of risk and opportunity in young adulthood. The traditional manufacturing and blue-collar sectors of the economy have shrunk, while the information and service sectors have grown. Even within these sectors, earnings inequality has increased dramatically, both across and within occupational categories. There are now broad strata of secure and stable professional and managerial jobs with benefits at the top of the labor market, and broad strata of insecure and unstable jobs with low wages and virtually no employer-provided benefits at the bottom (although these low wages can often be supplemented by a range of tax credits and publicly provided health care and child care benefits). The middle of the earnings distribution has diminished somewhat, however, especially in the production and clerical job categories that used to be accessible to high school graduates (and even dropouts in the manufacturing and blue-collar sectors).
As a result, the returns to higher education—how much more one earns over a lifetime by getting a college or graduate degree—have risen to historic levels, especially in specialized fields that support high-growth sectors of the economy. Increasingly, the way to achieve a middle-class level of earnings is to develop human capital by staying in school longer. A high school diploma, which used to be a ticket to the middle class, does not support mobility as it did in the past ( Bernhardt et al., 2001 ; Goldin and Katz, 2008 ; Schneider, 2007 ); most jobs now require at least some postsecondary education or training, if not a bachelor's degree or higher. At the same time that the benefits of college enrollment have increased, however, the financial costs of enrolling (and staying enrolled) also have increased, as discussed in Chapter 4 . Moreover, more students attend college without sufficient academic preparation and with very little knowledge or information about the world of colleges and universities. As a result, higher education is more economically necessary but also more difficult to attain for many young adults than in past decades.
Second, these socioeconomic changes have been accompanied by evolving norms and values regarding when young adults are expected to become independent of their parents and begin families of their own ( Johnson et al., 2011 ; Roisman et al., 2004 ). Observers of modern social trends have noted that contemporary parents believe that their active parenting role extends further into their children's life courses than was the case for parents in the past ( Fingerman et al., 2012 ). This new conceptualization of active and involved parenting as something that filters into children's 20s (and beyond) is often referred to as “helicopter” parenting ( Fingerman et al., 2012 ). At the same time, Americans are less likely to view the early 20s as an appropriate time for family formation, especially having children, and young adults themselves tend to view marriage as unsuitable for this period of life ( Teachman et al., 2000 ). Although this change in age norms has been most pronounced among the white middle class, it has pervaded diverse segments of the population in a process of cultural diffusion. Of course, changing age norms reflect changing behaviors (i.e., ideas about appropriate ages for a family transition change as people start making that transition at later ages), but age norms also shape how people view family transitions and, therefore, when they feel ready to make them ( Cherlin, 2009 ; Teachman et al., 2000 ).
These macro-level trends are, of course, related. For example, the rising returns to and costs of higher education and the insecurity of the labor market for new workers mean that young people often concentrate on school and work in their late teens and early 20s rather than committing to a partner or starting a family. In this way, the economic changes that shape schooling and work alter age norms about family formation. This impact appears to be greater for marriage than for cohabitation or parenting, as many young adults have high economic standards for entering marriage that do not apply to these other family transitions ( Edin and Kefalas, 2005 ; McLanahan, 2004 ). An economic consequence becomes a cultural influence. As discussed in Chapter 3 , these trends are also raising questions about parental obligations to provide financial support for education and other costs during this transitional period.
Overall, young adults now focus more on socioeconomic attainment than on family formation, which is lengthening the time to financial independence and keeping them tied to their families of origin. For youth from socioeconomically advantaged backgrounds, this period can then become a time of freedom and exploration. For youth from more disadvantaged backgrounds, there is a higher potential for stagnation, with supposed freedoms masking scarcer opportunities and cultural norms and economic realities not always being well aligned ( Arnett, 2004 ; Furstenberg, 2010 ). Both the timing and sequencing of young adult experiences, therefore, reflect the macro-level contexts in which young people are embedded and are closely connected to where they came from and where they are going.
A third important component of social change with implications for social roles and how they interact involves the advances in information technology in recent years. This technological revolution has reshaped American society as a whole and has been acutely felt among and driven by young adults. According to national data from the Pew Research Center, virtually all young adults use the Internet on a fairly regular basis, and nearly all have cell phones and use social media ( Lenhart, 2013 ). Moreover, racial/ethnic and socioeconomic disparities in rates of usage are not large. In fact, information technology and social media pervade most aspects of daily life among most young adults ( Lenhart, 2013 ). They are a central feature of school and work activities, keep young adults in closer contact with their parents compared with prior generations, allow young adults to greatly expand the reach of their social networks, serve as an increasingly popular venue for dating and union formation, provide new ways to increase health care access (and to improve health care delivery and facilitate the monitoring of personal health), and serve as a new context for political socialization and civic engagement ( Chan-Olmsted et al., 2013 ; Clark, 2012 ; Kreager et al., 2014 ; Turkle, 2011 ; Wegrzyn, 2014 ). Indeed, young adults are driving much of the innovation and growth of social media ( Lenhart, 2013 ). Consider a recent Harvard Business Review analysis ( Frick, 2014 ), which reports that the modal age of founders of billion-dollar Silicon Valley startups is 20-24. Thus, young adults are both consumers and creators of the new media, and the ways in which they move toward, take on, and function within adult roles are changing as a result—a theme that is revisited repeatedly in subsequent chapters.
- THE HEALTH OF YOUNG ADULTS
Thus far, the general developmental processes of young adulthood (unique in the life course if not historically specific) and the social activities and roles of young adulthood (unique in the life course and historically specific) have been discussed separately, but in reality, they are intertwined. One way to see this intertwining is to consider the health and health behaviors of young adults, which have physical, psychological, social, and structural underpinnings ( Johnson et al., 2011 ).
Developmentally, young adults are continuing to accrue and refine cognitive skills and psychological competencies for mature decision making and self-regulation, and they face fewer natural threats to physical health compared with older adults. As a result, they should engage in less risky behavior than adolescents and be in better health than older adults, both of which are true to some extent. Socially, however, they tend to live more outside the purview of their parents relative to adolescents, and they are less governed by their family's lifestyle and health habits—with less parental monitoring of sleep, curfews, peer relations, physical activity, and diet ( Harris et al., 2005 ). At the same time, compared with older adults, they are less likely to participate in work and family roles that serve as strong social controls on risk taking. And they often have less access to quality health care than younger adolescents or older adults. Consequently, some of the health advantages of young adulthood relative to adolescence or older adulthood may be undermined, and the period of vulnerability often associated with adolescence may be lengthened ( Harris et al., 2006 ; Neinstein, 2013 ; Schulenberg and Maggs, 2002 ).
Health Behavior
Table 2-1 shows the top 10 causes of death among young adults in the United States. The top five are related in part to lifestyles, behaviors, and risk taking, especially the top three (injury, homicide, and suicide). The same is true of many other causes of death just below the top five, such as HIV. In this way, young adulthood has been described as a transitional period between behavioral causes of death in adolescence and health-related causes of death in later adulthood ( Neinstein, 2013 ).
Leading Causes of Death in the United States (per 100,000 population), Ages 12-34.
Looking more closely at the top two causes of death, rates of unintentional injury and homicide are higher among young adults—especially males—than among any other age group ( CDC, 2012 ). Motor vehicle crashes account for the largest percentage of unintentional injuries, and young adults face the highest risk. Compared with those aged 26-34, young adults aged 18-25 are more likely to die or be injured in a motor vehicle crash and have more motor vehicle crash–related hospitalizations and emergency room visits ( CDC, 2012 ). Young adults also are at greatest risk of injury due to firearms; young adult males have 10 times the risk of such an injury compared with young adult females ( CDC, 2012 ).
With respect to basic health behaviors, Harris and colleagues (2006) tracked the health and health behavior of adolescents during their transition to young adulthood using National Longitudinal Study of Adolescent Health (Add Health) data. They examined 20 of the leading health indicators recognized in Healthy People 2010 —the national public health agenda—as most critical to the development of healthy young people and tracked these indicators for the same cohort of individuals beginning when they were aged 12-18 until they were aged 19-26. Although there were some positives, the dominant pattern was declining health, seen most clearly in health behaviors and related health statuses. As these individuals entered their early and mid-20s, they were less likely to exercise, eat breakfast, and get regular physical checkups and dental checkups, and they were more likely to east fast food, contract sexually transmitted diseases, smoke cigarettes, binge drink, and use marijuana and hard drugs ( Harris et al., 2006 ).
Substance use among young adults warrants special attention. The steady increase in substance use that begins in adolescence peaks during the young adult years ( Johnston et al., 2014 ). Unlike many of the trends discussed in this report, this escalation of substance use tends to be as high or higher among middle-class whites relative to other groups ( Johnston et al., 2014 ). Young adult rates and trajectories of substance use show considerable historical variation, reflecting cohort and period effects over the past 30 years ( Johnston et al., 2014 ). Of particular concern, the rate of increase in use of alcohol and marijuana during this time period has become more rapid for more recent cohorts ( Jager et al., 2013 ). At the same time, the general declines in substance use that characterize the rest of adulthood also tend to start in young adulthood; both sets of changes are associated with social role changes during this period ( Bachman et al., 2001 ; Schulenberg and Maggs, 2002 ). Alcohol use and especially binge drinking generally peak in the early 20s before declining, a trajectory that is especially pronounced among college students (as discussed in Chapter 4 ); depending on the historical period, marijuana use tends to peak somewhat earlier ( Johnston et al., 2014 ). Also depending on the historical period, annual and 30-day cigarette use tends to peak in the middle 20s and then decline; daily cigarette use, however, continues to increase with age across the 20s ( Johnston et al., 2014 ). Thus, young adult health behavior is risky in many ways but also suggests a nascent positive trend. Another way of looking at these patterns is that young adulthood may be the last gasp of many of the behavioral risks of the early life course.
Along with these health risk behaviors, young adults also engage in health-promoting behaviors. For example, young adults (aged 18-24) are more likely than any other age group of adults to meet the recommended guidelines for physical activity (30 percent, compared with 24 percent of those aged 25-44 and 18 percent of those aged 45-54) (see HHS, 2011 ). In other words, young adulthood is a mix of positives and negatives when it comes to health behavior. Given that young adult health behavior is likely a foundation for lifelong health trajectories, these patterns are one important lens for understanding that young adulthood is a critical developmental period.
Health Conditions
Because young adults tend to be in better health than older adults, they are often thought to be in good health, but this is not necessarily true. Evidence suggests that the health status of young adults in the United States varies considerably. For example, overall obesity rates increase through adulthood, rising from 23 percent in those aged 20-24; to 35 percent among those in their late 20s, 30s, and early 40s; and to more than 40 percent at older ages ( Harris, 2010 ). That being said, the rate among young adults is strikingly high (about one-quarter of the age group) and appears to be rising. In Add Health, a longitudinal study, obesity rates more than tripled from 11 percent in adolescence in 1995 to 37 percent by young adulthood in 2008 ( Harris, 2010 ). Research documenting the emergence of the obesity epidemic has found that rising body mass indexes and obesity prevalence first occurred in the 1990s (particularly among adolescents and somewhat among children) ( Lee et al., 2010 , 2011 ), so current cohorts of young adults are entering adulthood with much higher obesity rates relative to previous cohorts of young adults and are the first generation to experience dramatically rising obesity rates in childhood and adolescence and they carry this health burden into adulthood. Importantly, the rate of increase in obesity across the age transition has been found to vary by educational experiences and expectations ( Clarke et al., 2013 ).
In terms of obesity-related conditions, more than one in four young adults aged 24-32 in Add Health had hypertension, 69 percent were prehypertensive, 7 percent had diabetes, and 27 percent were prediabetic with impaired glucose tolerance or hyperglycemia ( Gooding et al., 2014 ; Nguyen et al., 2011 , 2014 ). Hypertension and diabetes are known risk factors for stroke, and the data reveal troubling increases in hospitalization for and prevalence of stroke among young adults over the past decade ( George et al., 2011 ; National Center for Health Statistics, 2011 ). Alarmingly, because many of these conditions (e.g., high blood pressure, hyperglycemia) are asymptomatic and young adults typically are not exposed to routine screening systems or may not see a health care provider regularly, they often are unaware of ongoing and permanent damage caused by chronic conditions. The levels of these health conditions suggest a higher than previously anticipated risk of cardiovascular disease in an age group often characterized as unburdened by chronic disease ( Gordon-Larsen et al., 2004 , 2010 ; Nguyen et al., 2011 ; Whitsel et al., 2011 , 2012 ). Overall, the current generation of young adults appears to be at the forefront of the obesity epidemic and is vulnerable to experiencing its comorbid consequences.
Mental health among young adults also is cause for concern. Along with substance use, mental health disorders are the greatest source of disability among young adults in the United States. Indeed, nearly two-thirds of the burden of disability in young adults is associated with either mental health or substance use disorders ( Davis, 2013 ), and by age 29, more than half of all individuals have experienced such a disorder ( Kessler et al., 2005 ). The onset of the most serious mental health conditions—psychotic disorders—typically occurs in young adulthood ( Seidman, 2013 ). Likewise, depression increasingly becomes a concern in young adulthood, as do suicidal thoughts, attempts, and deaths (recall the high placement of suicide in Table 2-1 ). Compared with those aged 25-34, young adults aged 18-25 have higher rates of serious psychological distress, and they are more likely to think about, plan for, and attempt suicide ( SAMHSA, 2009 ). Compared with adolescents, young adults also are more likely to complete suicide ( SAMHSA, 2009 ). Yet only a quarter of young adults with these experiences receive treatment or services, and they are more likely than older adults and adolescents to drop out of or discontinue treatment ( SAMHSA, 2009 ). In many ways, they get lost within a health care system that treats them like adults even though they have special needs relative to other adults ( Davis, 2013 ). That the specific mental health needs of young adults (relative to adolescents or all adults) rarely are studied on their own impedes the ability to serve this population.
In sum, the transition into adulthood is a critical period in health—despite the wide heterogeneity of experiences, health tends to worsen during this period and the higher levels of poor health in young adulthood tend to set the trajectories into adulthood with important consequences for future health ( Harris, 2010 ). During the exploratory years of this transition, young adults as a group continue risk taking and poor (although improving) decision making that expose them to such health risks as unintended injury, unprotected sex, violence, binge drinking, motor vehicle accidents, suicide, and poor diet and nutrition, with potential adult consequences of liver and neurological disease, cardiac impairment, and stroke, as well as mortality ( Clark et al., 2001 ; Johnston et al., 2014 ). As young adulthood comes to a close, there tend to be general improvements in health behavior.
The majority of young adults' health problems are preventable. The Affordable Care Act and other recent efforts to increase young adult health care coverage at the state level provide opportunities to enhance preventive care for young adults. However, efforts to provide them with preventive care are complicated by the lack of preventive guidelines for this age group and the fact that navigating the health care system during the transition from pediatric to adult providers is confusing and difficult, especially for those with behavioral health problems or a chronic disease (see Chapter 7 ).
Poor health in young adults has numerous negative impacts on individuals and on society at large. Beyond such obvious impacts as health care costs, it adversely affects national security, as reflected in the recruitment of military personnel. For example, estimates indicate that 12 percent of all age-eligible men and 35 percent of all age-eligible women were unable to meet U.S. Army standards for weight-to-height ratio and percent body fat in 2007-2008 ( Cawley and Maclean, 2012 ). Furthermore, the Department of Defense reported that between 2006 and 2011, 62,000 individuals who arrived for military training failed their entrance physical because of their weight ( Cutler and Miller, 2013 ).
Health Disparities
The health of young adults varies by race, ethnicity, sex, sexual identity, age, disability, education, socioeconomic position, and geographic location ( Hudson et al., 2013 ; Mulye et al., 2009 ). Certain populations of young adults have higher rates of such risky behaviors as unhealthy eating, lack of physical activity, unprotected sexual activity, substance use, and unsafe driving. In addition, major gender differences exist, as well as considerable ethnic and racial disparities, with non-Hispanic black and American Indian/non-Hispanic Alaska Native young adults faring worse in many areas ( Park et al., 2014 ). There are also gaps in knowledge about the health of certain groups, such as LGBT young adults and young adults living in poverty (for an overview of similar gaps in adolescent data, see Knopf et al., 2007 ). At the same time, it is important to note that the differences go both ways. Among young adults, for instance, black males have a higher homicide rate than white males (100.3 versus 11.4 homicides per 100,000) ( Smith and Cooper, 2013 ), but black males have a lower rate of illicit substance use than white males from early adolescence to young adulthood ( Chen and Jacobson, 2012 ).
- DIVERSITY AND THE EFFECTS OF BIAS AND DISCRIMINATION ON YOUNG ADULTS' HEALTH AND WELL-BEING
The United States today is in the midst of “an explosion of diversity” (William Frey, quoted in Ohlemacher, 2006 , p. 1). Based on the 2010 census count, one of every three Americans is a person of color ( U.S. Census Bureau, 2010 ). If these demographic patterns continue, non-Hispanic European Americans will cease to be a majority population in the United States before 2050, and there will be no racial or ethnic majority ( U.S. Census Bureau, 2012 ). These dramatic shifts in the “vanguard of America's new racial and ethnic diversity” are most evident in the booming population of minority youth ( Johnson and Lichter, 2012 , p. 32) and are likely, over time, to have a profound effect on the attitudes and experiences of adolescents and young adults as they are growing up, forming their group identities, and envisioning their place in the national community. Indeed, changes in the experiences of future cohorts of young adults will provide a useful measure of the extent to which coming of age in an increasingly diverse society affects the development of racial and ethnic identity, intergroup relations, and evolving conceptions of national identity.
In the meantime, however, many people of color continue to encounter systematic prejudice and discrimination that restrict opportunity and reduce well-being in pervasive ways and that contribute to the disparities in health and well-being of young adults documented throughout this report. Further, resistance to immigration in some parts of the country has heightened concerns about bias and discrimination based on ethnicity and religion ( Cauce et al., 2011 ; Kim et al., 2013 ). Effects of bias and discrimination on health and well-being, as well as factors that protect or buffer young people against these effects, are briefly summarized here, considered throughout the report, and explored in greater depth in Appendix B .
The experience of being exposed to biased and discriminatory behavior has been characterized as a pervasive and normative stressor in the lives of people of color ( García Coll et al., 1996 ). A 2013 national survey of adults by the Pew Research Center (2013a , b ) indicates that 88 percent of non-Hispanic blacks and 57 percent of non-Hispanic whites believe that blacks are subject to “some”/“a lot” of discrimination in the United States. Among all adults, 73 percent say that Muslim Americans are subject to “some”/“a lot” of discrimination, while 65 percent hold this view of Hispanics.
Experiencing bias and discrimination has been linked to poorer outcomes in education and employment, worse physical and psychological outcomes, and acculturation stress. For example, African Americans and Hispanics are overrepresented among high school dropouts, and the associations between early school leaving and young adults' future outcomes, including joblessness, have been well established (see Chapter 4 of this report). Among the many interrelated family, social, and economic factors that contribute to educational disadvantage for minorities, it is widely acknowledged that the differential treatment of minority children in school classification and discipline policies plays a significant role ( Alfaro et al., 2009 ; NRC, 2013 ; U.S. Department of Education and National Center for Education Statistics, 2014 ). Several systematic reviews ( Lee et al., 2009 ; Priest et al., 2013 ; Williams and Williams-Morris, 2000 ; Williams et al., 2003 ) have found strong associations between racial discrimination and mental health outcomes among all racial/ethnic groups. A recent meta-analytic review of experimental and correlational studies concludes that perceiving pervasive instances of discrimination negatively affects psychological well-being across a wide range of measures ( Schmitt et al., 2014 ). Persistent exposure to race-related stress increases “allostatic load,” and the accompanying heightened physiological responses are significant predictors of chronic diseases ( Karlamangla et al., 2006 ).
Current patterns of discrimination are associated with structural factors (e.g., economic and/or residential segregation, institutional racism) that restrict opportunity and affect well-being in pervasive ways. However, it is also important to recognize that disadvantaged cultural groups have developed productive, adaptive means of coping with their deprivations and that individual resilience and family strengths play important roles in supporting the healthy development of ethnic minority young adults even in the face of societal stressors ( García Coll et al., 1996 ). Several studies have identified factors that buffer, protect against, or reduce the impact of racism and discriminatory experiences on individuals ( Luthar, 2006 ). These factors include social support, connections, feelings of belonging, and cultural socialization. For more detailed discussion, see Appendix B .
- KEY FINDINGS AND IMPLICATIONS
The committee's key findings and their implications for the health, safety, and well-being of young adults are summarized below and discussed in greater detail in subsequent chapters of this report. Attention to these findings is intended to achieve progress toward ensuring the following key outcomes for young adults, with a particular focus on those young adults who are economically disadvantaged or otherwise marginalized:
- employment,
- housing stability,
- healthy relationships and connections to responsible adults,
- civic engagement and community involvement, and
- effective parenting.
1. Young adulthood is a critical developmental period
Like childhood and adolescence, young adulthood is a developmentally distinct period of the life course that can sensibly be viewed as a critical window of development with a strong effect on long-term trajectories. It is a time when individuals face significant challenges and are expected to assume new responsibilities and obligations. Success or failure in navigating these paths can set young adults on a course that will strongly affect the future trajectories of their adult lives. Early developmental and social trajectories may be reinforced or reversed, early risks may accumulate or be counteracted, new experiences can be turning points or sources of stagnation or thriving, and developmental tasks not completed may constitute a significant setback for the future.
Developmentally, young adulthood is a time of both opportunity and risk. The process of maturation is not suddenly completed when a young person turns 18. The brain is still maturing, and strengths and vulnerabilities continue to emerge. Thus, young adults continue to be strongly responsive to education and training and to incentives to create and contribute. Mistakes and failures can be reversed, and timely preventive interventions can reduce risks and ameliorate the consequences of injuries or disorders.
2. The world has changed in ways that place greater demands on young adults
Although the normal course of physiological and biological development of young adults probably has not changed in generations, the world in which they live has changed greatly. Today's young adults live in a more global and networked world, marked by increased knowledge and information transfer, heightened risks, fairly low social mobility, and greater inequality. Economic restructuring, advances in information and communication technologies, and changes in the labor market have radically altered the landscape of risk and opportunity in young adulthood. Demands are higher, and there is less latitude for failure. Much of the burden of a restructured economy has been borne by the current cohort of America's young adults. Developmentally speaking, young people are resilient and adaptable, but many young adults are struggling to find a path to employment, economic security, and well-being.
3. Young adults today follow less predictable pathways compared with young adults in previous generations
Beginning in the 1970s, several well-established patterns of social and economic transition that once defined young adulthood have been altered. In previous generations, the path for most young adults was predictable: graduate from high school, enter college or the workforce, leave home, find a spouse, and start a family ( Fussell, 2002 ). While there were always exceptions, these established milestones provided structure and direction for young adults as they assumed adult responsibilities. Today, those pathways are considerably less predictable, often extended, and sometimes significantly more challenging, as the following examples illustrate:
- The cost of college has grown substantially, and many students have difficulty financing the investment or repaying the debt, yet prospects for well-paying jobs for high school graduates without some postsecondary credential are slim. Although many young adults enter college, dropout rates are high, and the number of years needed to finish degree programs has risen.
- Well-compensated entry-level jobs are becoming more difficult to find, even for young college graduates, and especially in the aftermath of the Great Recession. Many companies do not provide health insurance or other nonsalary economic benefits. Low earnings plague many young workers because they lack skills needed for higher-paying knowledge-based jobs, increasing numbers of the jobs available to them are part time, and institutions that have traditionally protected less-educated workers have been weakened.
- The estimate of a recent study is that 6.7 million youth and young adults aged 16-24—about 17 percent of the population in this age range—are neither in school nor working ( Belfield and Levin, 2012 ). The rates are highest among African Americans and those aged 20-24, almost all of whom have left high school.
- Partnership and parenting patterns have shifted substantially. Many educated young adults live together for many years before marrying and having children, while many less-educated young adults have children outside of marriage before gaining the skills and income to support them. In addition, rapidly changing laws on same-sex marriage are providing new opportunities for family formation among LGBT young adults.
- The high cost of living independently has encouraged many young adults to move back into their parents' home, a pattern well documented among the “millennial” generation. 2
4. Inequality can be magnified during the young adult years
The disruption of established social and economic pathways has presented more choices and opportunities for some young adults while creating more barriers for others. The young adult population has diverse strengths, needs, social supports, and financial resources. Many young adults quickly assume typical adult roles, although perhaps tenuously and continuing to need institutional support. Others reach the end of this period without assuming any adult roles and having few prospects, suggesting a lack of opportunities, experiences, skills, and/or maturity. These divergent trajectories reflect not only differences in psychological, social, and physical capacities but also differential opportunities rooted in economic and social inequality. Persistent prejudice and discrimination limit opportunities and mobility for racial, ethnic, and religious minorities, as well as individuals with disabilities and divergent sexual preferences, and can also have an adverse impact on health (see Appendix B ).
In addition, marginalized young adults—such as those aging out of foster care, those in the justice system, those with disabilities, young parents, and children of low-income immigrants—are much less likely than other young adults to experience a successful transition to adulthood, although some of these young people ultimately fare very well as adults, and their hopes and aspirations are similar to those of their peers who have not been marginalized. Meeting the needs of marginalized groups not only improves their lives but also has the potential to help them become fully contributing members of society. In the absence of deliberate remedial action, however, this period of development is likely to magnify inequality, with lasting effects throughout adulthood.
5. Young adults connect generations
As the children of prior generations and the parents of future generations, young adults are deeply embedded in family systems both at the level of individual families and at the population level. As a result, young adult experiences are shaped by the advantages and disadvantages their parents bring to their lives, and these experiences become the contexts for the parenting of their own children. The simultaneous proximity of young adults to being dependent children of parents and parents of dependent children creates both risks and opportunities.
6. Young adults are at the forefront of social change
U.S. history is a story of sweeping economic, demographic, social, and technological changes, and young adults have long been at the leading edge of these changes. People in this age group tend to be highly interested in the broader world, their place in it, and how they can and do make a difference. They are greatly affected by global economic change, tend to be less conflicted than older adults about divisive cultural debates concerning behavioral norms and values, and are early adopters of new technologies—digital and social media being the most salient current example. They also are the leading edge of “an explosion of diversity” (William Frey, quoted in Ohlemacher, 2006 , p. 1) that will change the face of the nation, which, if current demographic trends continue, will have no racial or ethnic majority by 2050. As a result, adults who conduct research and design policies in any one era cannot simply extrapolate their own young adult experiences to those of the current cohort of young adults.
7. Young adults are surprisingly unhealthy
Young adulthood is a critical period for protecting health, not just during the transitional years but over the life course. Despite some positives, however, the dominant pattern among young adults today is declining health, seen most clearly in health behaviors and related health statuses such as the following:
- As adolescents age into their early and mid-20s, they are less likely to eat breakfast, exercise, and get regular physical and dental checkups, and more likely to eat fast food, contract sexually transmitted diseases, smoke cigarettes, use marijuana and hard drugs, and binge drink.
- In many areas of risky behavior, young adults show a worse health profile than both adolescents and older adults. Thus, young adulthood is when many risky behaviors peak, but it is also the time when involvement in risky behaviors begins to decline. Across this time period are many opportunities for prevention and early intervention.
- Early adulthood is a time of heightened psychological vulnerability and onset of serious mental health disorders, a problem compounded by failure to recognize illness or to seek treatment.
- The current generation of young adults appears to be at the forefront of the obesity epidemic and is more vulnerable than previous generations to obesity-related health consequences in later years.
The higher levels of poor health in young adulthood have important consequences for future health, educational attainment, and economic well-being. Rapid technological changes, economic challenges, and a prolonged transition to adulthood appear to be contributing to the health problems of young adults by increasing their stress and sedentary habits while making them less likely to participate in work and family roles that serve as strong social controls on risk taking. Therefore, these worrisome trends in young adult health can be expected to continue or worsen.
- PRINCIPLES TO GUIDE ACTION
Young adults are different from both adolescents and older adults, yet they often are combined with one or the other in statistical reporting and research design, as well as in policy and program classification. As a result, not enough is known about the special strengths and vulnerabilities of this population, as well as the ways in which socioeconomic and demographic disparities during this period of the life course contribute to disparities in the population at large. Likewise, little is known about the relative importance of young adulthood and other periods of the life course for long-term health and well-being. Furthermore, because of historical changes in how young adults live and what is expected of them, one cannot easily extrapolate from past research or policy traditions to today. An active, productive, and resilient population of young adults will benefit not only these young people but all members of U.S. society and the nation as a whole. Using the above findings and implications as a foundation, we offer corresponding principles to guide action that will help achieve this goal and that structure the discussion in the chapters to follow. Subsequent chapters provide an in-depth discussion of policies and programs in key domains for young adults' health and well-being, along with specific recommendations for key actors.
Principle 1: Pay specific attention to young adults in research and policy
Given the critical nature of young adulthood within the life course, it needs to be studied on its own rather than as an extension of adolescence or as a fungible period of adulthood. At the same time, long-term studies that embed this period within the life course are needed to elucidate both the independent and interconnected roles of young adult experiences in long-term life-course outcomes. Young adults often are cut off from child/adolescent services they may still need and are treated the same as older adults in adult services. Policy makers should ensure that outcomes are measured specifically for young adults and that programs take account of relevant differences between young and older adults.
Principle 2: Create economic opportunities for young adults
A shrinking number of well-paying jobs for young adults without a college education, the cost of higher education, and the prolonged period of transition to adult roles, exacerbated by economic volatility, pose an underlying threat to young adults' healthy adjustment and functioning. Taking action to improve prospects for social mobility can address the fundamental risks these young people face in modern society, risks that themselves have implications for the overall stability and progress of the nation.
Principle 3: Allow flexibility in policies and programs for young adults
Given the absence of clear normative pathways during this period of the life course, the transitions and subsequent trajectories of young adults depend on both the individual characteristics of young adults and the environments in which they are embedded. Thus, efforts to serve this population through policies and programs need to be tailored to the various subpopulations of young adults, defined not just developmentally but also demographically and socioeconomically. Age alone during this period of life should not necessarily define needs and dictate programming. Flexibility is needed in defining eligibility criteria and program requirements.
Principle 4: Invest in the least advantaged young adults
The prolonged period of educational attainment, together with its increasing costs, poses substantial burdens for the vast majority of families. But these challenges are especially daunting for the least advantaged families and the most marginalized young adults. Both research and policy should focus not just on increasing absolute levels of health, educational attainment, or other desired outcomes for young adults as a group, but also on making the investments needed to increase the productivity, health, and well-being of the many who are being left behind, as well as rectifying persistent racial and ethnic disparities.
Principle 5: Use multigenerational strategies to support young adults and their children
Multigenerational investments and interventions are a promising trend in policy and practice that needs to receive greater attention. Supporting the human capital and workforce development of young parents is likely an investment in the long-term developmental trajectories of their children, and programs focused on the early health and education of young children provide an opportunity to reach their parents, many of whom are young adults. Targeting the connections between generations, therefore, offers two ways to serve young adults, with ripple effects over time.
Principle 6: Empower and engage young adults in policies and programs
Young adults need to be at the table when decisions that affect them are being made, both because they deserve to be involved and because their input will contribute to better decision making. Their interest in such involvement is likely to be strong given their expanding perspective on the world. The influence of social media on young adult development and functioning is not yet fully understood, and the potential for social media to facilitate the implementation of policies and programs, especially in public health and health care, has not been fully tapped. Both research and policy agendas need to integrate social media and related information technologies. Because young adults typically are more expert in social media than many researchers and policy makers, the incorporation of social media into these agendas would be an example of the broader value of giving young adults a voice in the process.
Principle 7: Invest in preventive approaches to improve the health of young adults
Traditionally, the nation's health system has underemphasized preventive health services for young adults. Young adults' lack of health care insurance coverage often precludes them from seeking health care services, including the provision of preventive screening and services, although this gap has been somewhat alleviated by the Affordable Care Act and Medicaid expansion in some states. The role of families in ensuring continuity with a health care provider that offers preventive services also is diluted as young adults age out of their pediatrician's practice. Yet many of the risk behaviors in which young adults engage can be addressed by population-based interventions, as well as earlier screening and referrals, for example, for clinical and behavioral interventions. The Affordable Care Act, as one example, incorporates preventive health services as part of health insurance coverage. Given the act's emphasis on preventive services in such areas as reproductive health, substance abuse, and mental health, which reflect many of the health care needs of young adults, those young adults who enroll can clearly benefit from this newly available care.
The stability and progress of society at large depend on how any cohort of young adults fares as a whole. The same can be said of each cohort of children and adolescents, of course, but it is the transition to adulthood that reflects the end of trial periods and the beginning of more consequential actions. Young adults' successful transition to independent and healthy adulthood, entry into the workforce, continued productivity, and successful parenting can help ensure the security and well-being of the nation. A healthy and productive generation of young adults nurtures the next generation and provides the worker replacement needed to support the retiring generation.
Focusing on the health and well-being of the current cohort of young adults (those becoming adults in the first third of the 21st century) is especially important because of the powerful (and perhaps transformative) economic and social forces now at work. One is the rapidly increasing “elder dependency ratio” (i.e., the ratio of individuals in the population aged 65 and older to the working-age population). This ratio has been increasing rapidly in all advanced industrial countries while the fertility rate has been declining, leaving the current cohort of working-age adults to support increasing numbers of retiring elders. In the United States, the elder dependency ratio increased from about 1 elder to 10 workers (0.1) in 1950 to 0.2 in 2000 and is expected to increase to 0.35 by 2050 ( Fussell, 2002 ). This demographic shift led Elizabeth Fussell to call for renegotiating the “intergenerational contract” to couple building human capital through collective investments in young adults with increasing the age of eligibility for retirement support ( Fussell, 2002 ). A similar collective renegotiation may already be occurring, explicitly or implicitly, when parents invest in education and support for young adults well into their 20s.
Another transformative social and economic change now under way is the substantial increase in immigration to the United States. This trend has helped replenish the workforce and attenuate the rise in the elder dependency ratio (which is expected to increase, on average, to about 0.45 in other developed countries by 2050) while also changing the very face of U.S. society ( Fussell, 2002 ). This dramatic change is likely, over time, to have a profound effect on attitudes and experiences of adolescents and young adults as they are growing up, forming group identities, and envisioning their place in the national community. Indeed, changes in the experiences of future cohorts of young adults will provide a useful measure of the extent to which coming of age in an increasingly diverse society affects intergroup relations and evolving conceptions of national identity.
In sum, healthy, productive, and skilled young adults are critical for the nation's workforce, global competitiveness, public safety, and national security. Providing more of the educational, economic, social, and health supports needed by all young adults—particularly those whose background and characteristics put them at risk of experiencing the greatest struggles—will ensure equal opportunity, erase disparities, and enable more young adults to successfully embrace adult roles as healthy workers, parents, and citizens.
- Alfaro EC, Umaña-Taylor AJ, Gonzales-Backen MA, Bámaca MY, Zeiders KH. Latino adolescents' academic success: The role of discrimination, academic motivation, and gender. Journal of Adolescence. 2009; 32 (4):941–962. [ PubMed : 18973937 ]
- Arnett JJ. Emerging adulthood: The winding road from the late teens through the twenties. New York: Oxford University Press; 2004. [ PubMed : 10842426 ]
- Arroyo J, Payne KK, Brown SL, Manning WD. Crossover in median age at first marriage and first birth: Thirty years of change. Bowling Green, OH: National Center for Family and Marriage Research; 2013.
- Bachman JG, O'Malley PM, Schulenberg JE, Johnston LD, Bryant AL, Merline AC. The decline of substance use in young adulthood: Changes in social activities, roles, and beliefs. New York: Psychology Press; 2001.
- Bailey MJ, Dynarski SM. Gains and gaps: Changing inequality in U.S. college entry and completion. Cambridge, MA: National Bureau of Economic Research; 2011.
- Baum S, Flores S. Higher education and children in immigrant families. The Future of Children. 2011; 21 :171–193. [ PubMed : 21465860 ]
- Belfield C, Levin H. The economics of investing in opportunity youth. New York: Civic Enterprises; 2012.
- Bernhardt A, Morris M, Handcock MS, Scott MA. Divergent paths: Economic mobility in the new American labor market. New York: Russell Sage Foundation; 2001.
- Blakemore SJ. The social brain in adolescence. Nature Reviews Neuroscience. 2008; 9 (4):267–277. [ PubMed : 18354399 ]
- Bound J, Lovenheim MF, Turner S. Why have college completion rates declined? An analysis of changing student preparation and collegiate resources. American Economic Journal-Applied Economics. 2010; 2 (3):129–157. [ PMC free article : PMC3140225 ] [ PubMed : 21785668 ]
- Brock T. Young adults and higher education: Barriers and breakthroughs to success. The Future of Children. 2010; 20 (1):109–132. [ PubMed : 20364624 ]
- Cauce AM, Cruz R, Corona M, Conger R. Health disparities in youth and families. New York: Springer; 2011. pp. 13–32. (The face of the future: Risk and resilience in minority youth). [ PMC free article : PMC3714209 ] [ PubMed : 21166303 ]
- Cauffman E, Shulman EP, Steinberg L, Claus E, Banich MT, Graham S, Woolard J. Age differences in affective decision making as indexed by performance on the Iowa gambling task. Developmental Psychology. 2010; 46 (1):193–207. [ PubMed : 20053017 ]
- Cawley J, Maclean JC. Unfit for service: The implications of rising obesity for U.S. military recruitment. Health Economics. 2012; 21 (11):1348–1366. [ PubMed : 21971919 ]
- CDC (Centers for Disease Control and Prevention). Nonfatal injury report, 2001-2012. 2012. [July 22, 2014]. http://webappa .cdc.gov /sasweb/ncipc/nfirates2001.html .
- Chan-Olmsted S, Rim H, Zerba A. Mobile news adoption among young adults: Examining the roles of perceptions, news consumption, and media usage. Journalism & Mass Communication Quarterly. 2013; 90 :126–147.
- Chein J, Albert D, O'Brien L, Uckert K, Steinberg L. Peers increase adolescent risk taking by enhancing activity in the brain's reward circuitry. Developmental Science. 2011; 14 (2):F1–F10. [ PMC free article : PMC3075496 ] [ PubMed : 21499511 ]
- Chen P, Jacobson KC. Developmental trajectories of substance use from early adolescence to young adulthood: Gender and racial/ethnic differences. Journal of Adolescent Health. 2012; 50 (2):154–163. [ PMC free article : PMC3264901 ] [ PubMed : 22265111 ]
- Cherlin AJ. The marriage-go-round. New York: Random House LLC; 2009.
- Clark DB, Lynch KG, Donovan JE, Block GD. Health problems in adolescents with alcohol use disorders: Self-report, liver injury, and physical examination findings and correlates. Alcoholism-Clinical and Experimental Research. 2001; 25 (9):1350–1359. [ PubMed : 11584156 ]
- Clark LS. The parent app: Understanding families in the digital age. New York: Oxford University Press; 2012.
- Clarke PJ, O'Malley PM, Schulenberg JE, Lee H, Colabianchi N, Johnston LD. College expectations in high school mitigate weight gain over early adulthood: Findings from a national study of American youth. Obesity. 2013; 21 (7):1321–1327. [ PMC free article : PMC3742647 ] [ PubMed : 23666817 ]
- Cole TJ. The secular trend in human physical growth: A biological view. Economics & Human Biology. 2003; 1 (2):161–168. [ PubMed : 15463971 ]
- Cools R. Role of dopamine in the motivational and cognitive control of behavior. The Neuroscientist. 2008; 14 (4):381–395. [ PubMed : 18660464 ]
- Coontz S. Historical perspectives on family studies. Journal of Marriage and Family. 2000; 62 (2):283–297.
- Crosnoe R, Johnson MK. Research on adolescence in the twenty-first century. Annual Review of Sociology. 2011; 37 :439–460. [ PMC free article : PMC5695926 ] [ PubMed : 29167597 ]
- Cunningham MG, Bhattacharyya S, Benes FM. Amygdalo-cortical sprouting continues into early adulthood: Implications for the development of normal and abnormal function during adolescence. Journal of Comparative Neurology. 2002; 453 (2):116–130. [ PubMed : 12373778 ]
- Cutler T, Miller GA. Retired military generals: Recruits dismissed for obesity cost $1.1 billion a year. 2013. [August 21, 2014]. http://www .mlive.com/news/index .ssf/2013 /09/retired_military_generals_recr.html .
- Davis M. Young adult mental health; Presentation at IOM/NRC Workshop on Improving the Health, Safety, and Well-Being of Young Adults; Washington, DC. 2013. [October 10, 2014]. http://www .iom.edu/~ /media/Files/Activity%20Files /Children/ImprovingYoungAdultsHealth /Davis%20Presentation.pdf .
- Dennett J, Modestino AS. Uncertain futures? Youth attachment to the labor market in the United States and New England. Boston, MA: New England Public Policy Center; 2013.
- Dorn LD, Dahl RE, Woodward HR, Biro F. Defining the boundaries of early adolescence: A user's guide to assessing pubertal status and pubertal timing in research with adolescents. Applied Developmental Science. 2006; 10 (1):30–56.
- Edin K, Kefalas M. Promises I can keep: Why poor women put motherhood before marriage. Oakland: University of California Press; 2005.
- Ernst M, Pine DS, Hardin M. Triadic model of the neurobiology of motivated behavior in adolescence. Psychological Medicine. 2006; 36 (3):299–312. [ PMC free article : PMC2733162 ] [ PubMed : 16472412 ]
- Fingerman KL, Cheng YP, Wesselmann ED, Zarit S, Furstenberg F, Birditt KS. Helicopter parents and landing pad kids: Intense parental support of grown children. Journal of Marriage and Family. 2012; 74 (4):880–896. [ PMC free article : PMC4553417 ] [ PubMed : 26336323 ]
- Fischer CS, Hout M. Century of difference: How America changed in the last one hundred years. New York: Russell Sage Foundation; 2006.
- Frick W. Harvard Business Review. Apr 3, 2014. (How old are Silicon Valley's top founders? Here's the data).
- Fry R. A rising share of young adults live in their parents' home. Philadelphia, PA: Pew Research Center; 2013.
- Furstenberg FF Jr. On a new schedule: Transitions to adulthood and family change. The Future of Children. 2010; 20 (1):67–87. [ PubMed : 20364622 ]
- Fussell E. The future of adolescent experience: Societal trends and the transition to adulthood. Mortimer J, Larson R, editors. New York: Cambridge University Press; 2002. pp. 18–51. (Youth in aging societies).
- Fussell E, Furstenberg F. On the frontier of adulthood: Theory, research, and public policy. Settersten R, Frustenberg F, Rumbaut R, editors. Chicago, IL: University of Chicago Press; 2005. pp. 29–75. (The transition to adulthood during the 20th century: Race, nativity and gender).
- Fuster JM. Frontal lobe and cognitive development. Journal of Neurocytology. 2002; 31 (3-5):373–385. [ PubMed : 12815254 ]
- Fuster JM. The prefrontal cortex. 4th. Oxford, UK: Elsevier Ltd; 2008.
- Galván A, Hare TA, Parra CE, Penn J, Voss H, Glover G, Casey B. Earlier development of the accumbens relative to orbitofrontal cortex might underlie risk-taking behavior in adolescents. The Journal of Neuroscience. 2006; 26 (25):6885–6892. [ PMC free article : PMC6673830 ] [ PubMed : 16793895 ]
- García Coll C, Lamberty G, Jenkins R, McAdoo HP, Crnic K, Wasik BH, Vázquez García H. An integrative model for the study of developmental competencies in minority children. Child Development. 1996; 67 (5):1891–1914. [ PubMed : 9022222 ]
- Gee DG, Humphreys KL, Flannery J, Goff B, Telzer EH, Shapiro M, Hare TA, Bookheimer SY, Tottenham N. A developmental shift from positive to negative connectivity in human amygdala-prefrontal circuitry. Journal of Neuroscience. 2013; 33 (10):4584–4593. [ PMC free article : PMC3670947 ] [ PubMed : 23467374 ]
- Geier C, Terwilliger R, Teslovich T, Velanova K, Luna B. Immaturities in reward processing and its influence on inhibitory control in adolescence. Cerebral Cortex. 2010; 20 (7):1613–1629. [ PMC free article : PMC2882823 ] [ PubMed : 19875675 ]
- George MG, Tong X, Kuklina EV, Labarthe DR. Trends in stroke hospitalizations and associated risk factors among children and young adults, 1995-2008. Annals of Neurology. 2011; 70 (5):713–721. [ PubMed : 21898534 ]
- Giedd JN, Castellanos FX, Rajapakse JC, Vaituzis AC, Rapoport JL. Sexual dimorphism of the developing human brain. Progress in Neuro-Psychopharmacology and Biological Psychiatry. 1997; 21 (8):1185–1201. [ PubMed : 9460086 ]
- Gogtay N, Giedd JN, Lusk L, Hayashi KM, Greenstein D, Vaituzis AC, Nugent TF, Herman DH, Clasen LS, Toga AW. Dynamic mapping of human cortical development during childhood through early adulthood. Proceedings of the National Academy of Sciences of the United States of America. 2004; 101 (21):8174–8179. [ PMC free article : PMC419576 ] [ PubMed : 15148381 ]
- Goldin CD, Katz LF. The race between education and technology. Cambridge, MA: Belknap Press of Harvard University Press; 2008.
- Gooding HC, McGinty S, Richmond TK, Gillman MW, Field AE. Hypertension awareness and control among young adults in the National Longitudinal Study of Adolescent Health. Journal of General Internal Medicine. 2014; 29 (8):1098–1104. [ PMC free article : PMC4099443 ] [ PubMed : 24577758 ]
- Gordon-Larsen P, Adair LS, Nelson MC, Popkin BM. Five-year obesity incidence in the transition period between adolescence and adulthood: The National Longitudinal Study of Adolescent Health. American Journal of Clinical Nutrition. 2004; 80 (3):569–575. [ PubMed : 15321794 ]
- Gordon-Larsen P, The NS, Adair LS. Longitudinal trends in obesity in the United States from adolescence to the third decade of life. Obesity (Silver Spring). 2010; 18 (9):1801–1804. [ PMC free article : PMC2929301 ] [ PubMed : 20035278 ]
- Greimel E, Nehrkorn B, Schulte-Rüther M, Fink GR, Nickl-Jockschat T, Herpertz-Dahlmann B, Konrad K, Eickhoff SB. Changes in grey matter development in autism spectrum disorder. Brain Structure and Function. 2013; 218 (4):929–942. [ PMC free article : PMC3695319 ] [ PubMed : 22777602 ]
- Hare TA, Tottenham N, Galván A, Voss HU, Glover GH, Casey BJ. Biological substrates of emotional reactivity and regulation in adolescence during an emotional go-nogo task. Biological Psychiatry. 2008; 63 (10):927–34. [ PMC free article : PMC2664095 ] [ PubMed : 18452757 ]
- Harris KM. An integrative approach to health. Demography. 2010; 47 (1):1–22. [ PMC free article : PMC3000007 ] [ PubMed : 20355681 ]
- Harris KM, King RB, Gordon-Larsen P. What do children need to flourish. New York: Springer; 2005. pp. 111–132. (Healthy habits among adolescents: Sleep, exercise, diet, and body image).
- Harris KM, Gordon-Larsen P, Chantala K, Udry JR. Longitudinal trends in race/ethnic disparities in leading health indicators from adolescence to young adulthood. Archives of Pediatrics & Adolescent Medicine. 2006; 160 (1):74–81. [ PubMed : 16389215 ]
- HHS (U.S. Department of Health and Human Services). Healthy people 2020. 2011. [July 22, 2014]. http://www .healthypeople .gov/2020/default.aspx .
- Holzer HJ, Dunlop E. Just the facts, ma'am: Postsecondary education and labor market outcomes in the US. Bonn, Germany: IZA (Institute for the Study of Labor; 2013.
- Hudson DL, Puterman E, Bibbins-Domingo K, Matthews KA, Adler NE. Race, life course socioeconomic position, racial discrimination, depressive symptoms and self-rated health. Social Science & Medicine. 2013; 97 :7–14. [ PubMed : 24161083 ]
- Hunter ND. Introduction: The future impact of same-sex marriage: More questions than answers. Georgetown Law Journal. 2012; 100 (6):1855–1879.
- Jager J, Schulenberg JE, O'Malley PM, Bachman JG. Historical variation in drug use trajectories across the transition to adulthood: The trend toward lower intercepts and steeper, ascending slopes. Development and Psychopathology. 2013; 25 (2):527–543. [ PMC free article : PMC3641689 ] [ PubMed : 23627961 ]
- Johnson KM, Lichter DT. International handbook of rural demography. Kulcsár LJ, Curtis KJ, editors. The Netherlands: Springer; 2012. pp. 17–34. (Rural natural increase in the new century: America's third demographic transition).
- Johnson MK, Crosnoe R, Elder GH. Insights on adolescence from a life course perspective. Journal of Research on Adolescence. 2011; 21 (1):273–280. [ PMC free article : PMC3072576 ] [ PubMed : 21483644 ]
- Johnston LD, O'Malley PM, Bachman JG, Schulenberg JE, Miech RA. Ann Arbor: Institute for Social Research, University of Michigan; Monitoring the future national survey results on drug use, 1975-2013. Volume II: College students and adults ages 19-50. 2014
- Karlamangla AS, Singer BH, Seeman TE. Reduction in allostatic load in older adults is associated with lower all-cause mortality risk: MacArthur studies of successful aging. Psychosomatic Medicine. 2006; 68 (3):500–507. [ PubMed : 16738085 ]
- Kessler RC, Chiu WT, Demler O, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the national comorbidity survey replication. Archives of General Psychiatry. 2005; 62 (6):617–627. [ PMC free article : PMC2847357 ] [ PubMed : 15939839 ]
- Kim SY, Chen Q, Wang Y, Shen Y, Orozco-Lapray D. Longitudinal linkages among parent-child acculturation discrepancy, parenting, parent-child sense of alienation, and adolescent adjustment in Chinese immigrant families. Developmental Psychology. 2013; 49 (5):900–912. [ PMC free article : PMC3514557 ] [ PubMed : 22799587 ]
- Knopf DK, Park MJ, Brindis CD, Mulye TP, Irwin CE Jr. What gets measured gets done: Assessing data availability for adolescent populations. Maternal and Child Health Journal. 2007; 11 (4):335–345. [ PubMed : 17308967 ]
- Kreager DA, Cavanagh SE, Yen J, Yu M. Where have all the good men gone? Gendered interactions in online dating. Journal of Marriage and Family. 2014; 76 (2):387–410. [ PMC free article : PMC4043335 ] [ PubMed : 24910472 ]
- Lebel C, Walker L, Leemans A, Phillips L, Beaulieu C. Microstructural maturation of the human brain from childhood to adulthood. NeuroImage. 2008; 40 (3):1044–1055. [ PubMed : 18295509 ]
- Lee H, Lee D, Guo G, Harris KM. Trends in body mass index in adolescence and young adulthood in the United States: 1959-2002. Journal of Adolescent Health. 2011; 49 (6):601–608. [ PMC free article : PMC3228354 ] [ PubMed : 22098770 ]
- Lee JM, Pilli S, Gebremariam A, Keirns CC, Davis MM, Vijan S, Freed GL, Herman WH, Gurney JG. Getting heavier, younger: Trajectories of obesity over the life course. International Journal of Obesity. 2010; 34 (4):614–623. [ PMC free article : PMC2926791 ] [ PubMed : 19949415 ]
- Lee S, Juon HS, Martinez G, Hsu CE, Robinson ES, Bawa J, Ma GX. Model minority at risk: Expressed needs of mental health by Asian American young adults. Journal of Community Health. 2009; 34 (2):144–152. [ PMC free article : PMC3296234 ] [ PubMed : 18931893 ]
- Lenhart A. Young adults, mobile phones and social media: Technology and the transition to adulthood; Presentation at IOM/NRC Workshop on Improving the Health, Safety, and Well-Being of Young Adults; Washington, DC. 2013. [October 10, 2014]. http://www .iom.edu/~ /media/Files/Activity%20Files /Children/ImprovingYoungAdultsHealth /Lenhart%20Presentation.pdf .
- Lenroot RK, Gogtay N, Greenstein DK, Wells EM, Wallace GL, Clasen LS, Blumenthal JD, Lerch J, Zijdenbos AP, Evans AC. Sexual dimorphism of brain developmental trajectories during childhood and adolescence. NeuroImage. 2007; 36 (4):1065–1073. [ PMC free article : PMC2040300 ] [ PubMed : 17513132 ]
- Lichter DT, McLaughlin DK, Ribar DC. Economic restructuring and the retreat from marriage. Social Science Research. 2002; 31 (2):230–256.
- Luna B. Developmental changes in cognitive control through adolescence. Advances in Child Development and Behavior. 2009; 37 :233–278. [ PMC free article : PMC2782527 ] [ PubMed : 19673164 ]
- Luna B, Padmanabhan A, O'Hearn K. What has fMRI told us about the development of cognitive control through adolescence. Brain and Cognition. 2010; 72 (1):101–113. [ PMC free article : PMC2815087 ] [ PubMed : 19765880 ]
- Luthar SS. Cicchetti D, Cohen DJ, editors. Developmental psychopathology. 2nd. Hoboken, NJ: Wiley; 2006. pp. 739–795. (Resilience in development: A synthesis of research across five decades).
- McLanahan S. Diverging destinies: How children are faring under the second demographic transition. Demography. 2004; 41 (4):607–627. [ PubMed : 15622946 ]
- Modell J, Furstenberg FF, Hershberg T. Social-change and transitions to adulthood in historical-perspective. Journal of Family History. 1976; 1 (1):7–32.
- Mulye TP, Park MJ, Nelson CD, Adams SH, Irwin CE Jr, Brindis CD. Trends in adolescent and young adult health in the United States. Journal of Adolescent Health. 2009; 45 (1):8–24. [ PubMed : 19541245 ]
- National Center for Health Statistics. Health, United States, 2011. Washington, DC: U.S. Government Printing Office; 2011.
- Neinstein L. The new adolescents: An analysis of health conditions, behaviors, risks and access to services among young adults. Los Angeles: University of Southern California; 2013.
- Nguyen QC, Tabor JW, Entzel PP, Lau Y, Suchindran C, Hussey JM, Halpern CT, Harris KM, Whitsel EA. Discordance in national estimates of hypertension among young adults. Epidemiology. 2011; 22 (4):532–541. [ PMC free article : PMC3109249 ] [ PubMed : 21610501 ]
- Nguyen QC, Whitsel EA, Tabor JW, Cuthbertson CC, Wener MH, Potter AJ, Halpern CT, Killeya-Jones LA, Hussey JM, Suchindran C, Harris KM. Annals of Epidemiology. 2014. [October 22, 2014]. (Blood spot-based measures of glucose homeostasis and diabetes prevalence in a nationally representative population of young U.S. adults). (published online ahead of print). http://dx .doi.org/10 .1016/j.annepidem.2014.09.010 . [ PMC free article : PMC4255475 ] [ PubMed : 25444890 ]
- NRC (National Research Council). Reforming juvenile justice: A developmental approach. Washington, DC: The National Academies Press; 2013.
- Ohlemacher S. Diversity grows in 49 of 50 states. 2006. [October 16, 2014]. (Associated Press). http://seattletimes .com /html/nationworld /2003199276_diversity15.html .
- Ordaz S, Luna B. Sex differences in physiological reactivity to acute psychosocial stress in adolescence. Psychoneuroendocrinology. 2012; 37 (8):1135–1157. [ PMC free article : PMC3472630 ] [ PubMed : 22281210 ]
- Ordaz SJ, Foran W, Velanova K, Luna B. Longitudinal growth curves of brain function underlying inhibitory control through adolescence. Journal of Neuroscience. 2013; 33 (46):18109–18124. [ PMC free article : PMC3828464 ] [ PubMed : 24227721 ]
- Padmanabhan A, Luna B. Developmental imaging genetics: Linking dopamine function to adolescent behavior. Brain and Cognition. 2013; 89 (0):27–38. [ PMC free article : PMC4226044 ] [ PubMed : 24139694 ]
- Park MJ, Scott JT, Adams SH, Brindis CD, Irwin CE Jr. Adolescent and young adult health in the United States in the past decade: Little improvement and young adults remain worse off than adolescents. Journal of Adolescent Health. 2014; 55 (1):3–16. [ PubMed : 24815958 ]
- Parke RD. Future families: Diverse forms, rich possibilities. Hoboken, NJ: John Wiley & Sons; 2013.
- Patrick ME, Schulenberg JE, O'Malley PM. Youth & Society. 2013. pp. 1–23. (High school substance use as a predictor of college attendance, completion, and dropout: A national multicohort longitudinal study). [ PMC free article : PMC4847148 ] [ PubMed : 27134316 ]
- Payne K. FP-11-11. On the road to adulthood: Sequencing of family experiences. 2011. [July 22, 2014]. http://scholarworks .bgsu .edu/ncfmr_family_profiles/10 .
- Payne K. FP-12-04. School enrollment and completion. 2012. [July 22, 2014]. http://scholarworks .bgsu .edu/ncfmr_family_profiles/17 .
- Petanjek Z, Judaš M, Šimić G, Rašin MR, Uylings HB, Rakic P, Kostović I. Extraordinary neoteny of synaptic spines in the human prefrontal cortex. Proceedings of the National Academy of Sciences of the United States of America. 2011; 108 (32):13281–13286. [ PMC free article : PMC3156171 ] [ PubMed : 21788513 ]
- Pew Research Center. After Boston, little change in views of Islam and violence. Washington, DC: Pew Research Center; 2013a. [October 15, 2014]. http://www .people-press .org/2013/05/07/after-bostonlittle-change-in-views-of-islam-and-violence/
- Pew Research Center. For African Americans, discrimination is not dead. Washington, DC: Pew Research Center; 2013b. [September 26, 2014]. http://www .pewresearch .org/fact-tank/2013 /06/28/for-africanamericans-discrimination-is-not-dead/
- Priest N, Paradies Y, Trenerry B, Truong M, Karlsen S, Kelly Y. A systematic review of studies examining the relationship between reported racism and health and wellbeing for children and young people. Social Science & Medicine. 2013; 95 :115–127. [ PubMed : 23312306 ]
- Raznahan A, Shaw PW, Lerch JP, Clasen LS, Greenstein D, Berman R, Pipitone J, Chakravarty MM, Giedd JN. Longitudinal four-dimensional mapping of subcortical anatomy in human development. Proceedings of the National Academy of Sciences of the United States of America. 2014; 111 (4):1592–1597. [ PMC free article : PMC3910572 ] [ PubMed : 24474784 ]
- Rindfuss RR, Swicegood CG, Rosenfeld RA. Disorder in the life course—how common and does it matter. American Sociological Review. 1987; 52 (6):785–801.
- Roisman GI, Masten AS, Coatsworth JD, Tellegen A. Salient and emerging developmental tasks in the transition to adulthood. Child Development. 2004; 75 (1):123–133. [ PubMed : 15015679 ]
- SAMHSA (Substance Abuse and Mental Health Services Administration). Results from the 2008 National Survey on Drug Use and Health: National findings. Rockville, MD: SAMHSA; 2009.
- Scherf KS, Smyth JM, Delgado MR. The amygdala: An agent of change in adolescent neural networks. Hormones and Behavior. 2013; 64 (2):298–313. [ PMC free article : PMC3781589 ] [ PubMed : 23756154 ]
- Schmitt MS, Branscombe NR, Postmes T, Barcia A. The consequences of perceived discrimination for psychological well-being: A meta-analytic review. Psychological Bulletin. 2014; 140 :921–948. [ PubMed : 24547896 ]
- Schneider B. Forming a college-going community in U.S. public high schools. Lansing: Michigan State University; 2007.
- Schulenberg JE, Maggs JL. A developmental perspective on alcohol use and heavy drinking during adolescence and the transition to young adulthood. Journal of Studies on Alcohol. 2002; 14 :54–70. [ PubMed : 12022730 ]
- Schulenberg JE, Schoon I. The transition to adulthood across time and space: Overview of special section. Longitudinal and Life Course Studies. 2012; 3 (2):164–172. [ PMC free article : PMC4603838 ] [ PubMed : 26473017 ]
- Seidman LJ. Mental health—psychotic disorders; Presentation at IOM/NRC Workshop on Improving the Health, Safety, and Well-Being of Young Adults; Washington, DC. 2013. [October 10, 2014]. http://www .iom.edu/~ /media/Files/Activity%20Files /Children/ImprovingYoungAdultsHealth /Seidman%20Presentation.pdf .
- Seltzer JA. Families formed outside of marriage. Journal of Marriage and Family. 2000; 62 (4):1247–1268.
- Settersten RA, Ray B. Not quite adults: Why 20-somethings are choosing a slower path to adulthood, and why it's good for everyone. 1st. New York: Delacorte Press; 2010.
- Shanahan MJ. Pathways to adulthood in changing societies: Variability and mechanisms in life course perspective. Annual Review of Sociology. 2000; 26 :667–692.
- Simmonds D, Hallquist MN, Asato M, Luna B. Developmental stages and sex differences of white matter and behavioral development through adolescence: A longitudinal diffusion tensor imaging (DTI) study. NeuroImage. 2013; 92 :356–368. [ PMC free article : PMC4301413 ] [ PubMed : 24384150 ]
- Smith AR, Chein J, Steinberg L. Impact of socio-emotional context, brain development, and pubertal maturation on adolescent risk-taking. Hormones and Behavior. 2013; 64 (2):323–332. [ PMC free article : PMC3761223 ] [ PubMed : 23998675 ]
- Smith EL, Cooper A. Homicide in the U.S. known to law enforcement, 2011. Washington, DC: Bureau of Justice Statistics; 2013.
- Somerville LH, Casey B. Developmental neurobiology of cognitive control and motivational systems. Current Opinion in Neurobiology. 2010; 20 (2):236–241. [ PMC free article : PMC3014528 ] [ PubMed : 20167473 ]
- Sowell ER, Thompson PM, Holmes CJ, Jernigan TL, Toga AW. In vivo evidence for post-adolescent brain maturation in frontal and striatal regions. Nature Neuroscience. 1999; 2 (10):859–861. [ PubMed : 10491602 ]
- Sowell ER, Peterson BS, Thompson PM, Welcome SE, Henkenius AL, Toga AW. Mapping cortical change across the human life span. Nature Neuroscience. 2003; 6 (3):309–315. [ PubMed : 12548289 ]
- Spear LP. Neurobehavioral changes in adolescence. Current Directions in Psychological Science. 2000; 9 (4):111–114.
- Steinberg L. Psychological development in young adulthood; Presentation at IOM/NRC Workshop on Improving the Health, Safety, and Well-Being of Young Adults; Washington, DC. 2013.
- Steinberg L, Albert D, Cauffman E, Banich M, Graham S, Woolard J. Age differences in sensation seeking and impulsivity as indexed by behavior and self-report: Evidence for a dual systems model. Developmental Psychology. 2008; 44 :1764–1778. [ PubMed : 18999337 ]
- Stone J, Berrington A, Falkingham J. Gender, turning points, and boomerangs: Returning home in young adulthood in Great Britain. Demography. 2013; 51 :257–276. [ PubMed : 24186334 ]
- Teachman JD, Tedrow LM, Crowder KD. The changing demography of America's families. Journal of Marriage and Family. 2000; 62 (4):1234–1246.
- Turkle S. Together alone: Why we expect more from technology and less from each other. New York: Basic Books; 2011.
- U.S. Census Bureau. Foreign-born population in the United States, 2010. Washington, DC: U.S. Department of Commerce; 2010. [October 10, 2014]. http://www .census.gov /prod/2012pubs/acs-19.pdf .
- U.S. Census Bureau. 2012 national population projections. 2012. [October 16, 2014]. http://www .census.gov /population/projections /data/national/2012.html .
- U.S. Department of Education and National Center for Education Statistics. The condition of education 2014. 2014. [October 10, 2014]. (NCES 2014-083). http://nces .ed.gov/pubs2014/2014083.pdf .
- van Leijenhorst L, Moor BG, Op de Macks ZA, Rombouts SA, Westenberg PM, Crone EA. Adolescent risky decision-making: Neurocognitive development of reward and control regions. NeuroImage. 2010; 51 (1):345–355. [ PubMed : 20188198 ]
- Wahlstrom D, Collins P, White T, Luciana M. Developmental changes in dopamine neurotransmission in adolescence: Behavioral implications and issues in assessment. Brain and Cognition. 2010; 72 (1):146–159. [ PMC free article : PMC2815132 ] [ PubMed : 19944514 ]
- Wegrzyn C. Social media and information technology; Presentation at IOM/NRC Workshop on Improving the Health, Safety, and Well-Being of Young Adults: State Policies and Programs and Social Media and Information Technology; Washington, DC. 2014.
- Whitsel EA, Nguyen QC, Suchindran C, Hussey JM, Killeya-Jones LA, Tabor JW, Fitzgerald CS, Hallquist SP, Halpern CT, Harris KM. Value added quality, quantity, and diversity of national blood pressure data on young adults. Epidemiology. 2011; 22 (4):544–545.
- Whitsel EA, Nguyen QC, Suchindran C, Tabor JW, Cuthbertson CC, Wener MH, Potter AJ, Killeya-Jones L, Hussey JM, Halpern CT, Harris KM. Dried capillary whole blood spot-based hemoglobin A1c, fasting glucose, and diabetes prevalence in a nationally representative population of young U.S. adults: Add Health, wave IV. Circulation. 2012; 125 :AP010.
- Wierenga L, Langen M, Ambrosino S, van Dijk S, Oranje B, Durston S. Typical development of basal ganglia, hippocampus, amygdala and cerebellum from age 7 to 24. NeuroImage. 2014; 96 :67–72. [ PubMed : 24705201 ]
- Williams D, Williams-Morris R. Racism and mental health: The African American experience. Ethnicity and Health. 2000; 5 (3-4):243–268. [ PubMed : 11105267 ]
- Williams DR, Neighbors HW, Jackson JS. Racial/ethnic discrimination and health: Findings from community studies. American Journal of Public Health. 2003; 93 (2):200–208. [ PMC free article : PMC1447717 ] [ PubMed : 12554570 ]
- Zagorsky JL, Smith PK. The freshman 15: A critical time for obesity intervention or media myth. Social Science Quarterly. 2011; 92 (5):1389–1407.
Young adults may live with one or both parents.
A variety of age ranges are used to define the millennial generation. One example is those born between 1982 and 2003.
- Cite this Page Committee on Improving the Health, Safety, and Well-Being of Young Adults; Board on Children, Youth, and Families; Institute of Medicine; National Research Council; Bonnie RJ, Stroud C, Breiner H, editors. Investing in the Health and Well-Being of Young Adults. Washington (DC): National Academies Press (US); 2015 Jan 27. 2, Young Adults in the 21st Century.
- PDF version of this title (2.6M)
In this Page
Related information.
- PMC PubMed Central citations
- PubMed Links to PubMed
Recent Activity
- Young Adults in the 21st Century - Investing in the Health and Well-Being of You... Young Adults in the 21st Century - Investing in the Health and Well-Being of Young Adults
Your browsing activity is empty.
Activity recording is turned off.
Turn recording back on
Connect with NLM
National Library of Medicine 8600 Rockville Pike Bethesda, MD 20894
Web Policies FOIA HHS Vulnerability Disclosure
Help Accessibility Careers
- Our Staff & Board
- Opportunities
- The Conference
- Power Through Choices
Straight from our trainers, these presentation tips will set you up for a fabulous presentation
February 16, 2024
Y ou could say we’ve done this a few times. As a capacity-building organization, our staff are well versed in how to give an effective presentation. Here are some tips to help you design and facilitate effective presentations.
When preparing for your presentation:
Make it fun.
Be creative and authentic in your design, title, and description. A little humor never hurts!
Clearly identify the intended, appropriate audience.
It is important to identify who the presentation is for, so you can tailor the content of the presentation. Focusing your design on a specific audience makes the presentation feel relevant and relatable for the participants.
Write a catchy, creative title and a clear, detailed description.
Participants want to be able to make appropriate choices when planning their schedule, so they need to know who your presentation is for, what they are going to learn or be able to do, and why it is important to them.
Incorporate new ideas and the latest research.
Participants are attending your presentation to learn what is NEW! Make sure your content is relevant to what is happening today.
Time your presentation well and present an appropriate amount of content.
It’s tempting to pack too much content into a short session, but learners will feel more satisfied knowing something really well, rather than feeling rushed and unclear about a large amount of information. And be sure to allow time for questions.
Use adult learning principles.
Adult learning principles can help you understand how your audience learns, so that you can deliver your content in a way that will be most accessible. Remember—what you are saying matters as much as how you are saying it.
Avoid lectures.
People learn better when they feel involved and when content is processed through their own experience. Avoid telling participants information—instead, help them make discoveries themselves.
Break up the presentation with various learning strategies.
Active learning strategies help your participants get engaged and involved in your presentation. There are tons of active learning activities. Choose one (or a few) to incorporate into your presentation!
Use appealing visual aids.
If using PowerPoint or similar software, follow appropriate slide design principles . It’s helpful for learners to have a visual aid, but remember, the presentation is about you, not the slides, so do not make the slides a script for or the focus of the entire presentation.
Provide helpful materials, but don’t overwhelm your participants.
It can be useful for participants to have a tip sheet or a summary of some key information from the presentation, but too many materials can be overwhelming. Providing participants with all the information and notes can make them feel like they do not need to be engaged.
Prepare a detailed design, so another person could give the same presentation.
Maybe someone else in your organization wants to deliver the presentation again. A detailed design will make the presentation replicable, increasing organizational capacity. And of course, we never know what emergencies may pop up, so it’s important that another facilitator could easily follow your presentation design.
Run through your presentation in advance.
If possible, facilitate a pilot presentation. Practice, practice, practice! Get feedback from colleagues or friends.
From TED Talk-style presentations to panel discussions and more, we’re grateful to have had such amazing presenters at Heathy Teen Network conferences over the years!
PHOTO CREDIT: Gina Desiderio at Healthy Teen Network
When facilitating your presentation:
Keep it fun.
Same as with your design, be creative and authentic in your delivery…and humor always helps!
Leverage participants’ experiences.
Provide opportunities for discussion and sharing. If learners understand the relevance of the content to their own experiences, it can help them process and retain the information. Also, by sharing experiences, we can all learn from each other.
Save time for questions and feedback.
Allocate at least 10 minutes at the end of the presentation for a question-and-answer session and evaluation. Did you meet your objectives? The best way to improve is to get feedback from the participants! Save adequate time at the end for Q&A and evaluation.
Let them know how to follow up.
Provide information for further resources, as well as your contact information. Your participants may think of questions later, or need more information when it comes to applying your content. Make yourself and other resources available to them, so they can really apply their knowledge.
At Healthy Teen Network, w e believe every young person has the right to be who they are and love who they love . And we see you, the professionals and caring adults, helping them do this. We know you do your best when you're connected to great opportunities and resources. That's why we're here...to help make those connections and support you. Read more about us .

Quick Tips for Effective Presentations

Taking Care of Each Other at #HealthyTeen23

Seeds of Healing: A Community Garden Experience by Thrivology

Menstrual Dignity for Students Program to Receive 2023 Healthy Teen Network #StandingStrong Award

Marlen Ramirez to Receive 2023 Healthy Teen Network Outstanding Former Young Parent Award

Raphael House of Portland to Receive 2023 Healthy Teen Network Innovation Award

Journey with Us to Take Care and Take Action at #HealthyTeen23

Taking Time to Smell the Roses at #HealthyTeen23

Elevate Your Experience at #HealthyTeen23

That Just Gave Me Goosebumps! The Artistry Behind an Immersive, Emotional Encounter with Banned Books

Save the Date! May Is Sex Ed for All Month!

Sex Education Is Essential (Sex Ed for All Talking Points)

5 Queer Sex Ed Resources by and for Young People
Presentations for Teens & Young Adults
Elizabeth provides a variety of engaging PowerPoint presentations for students in junior high, high school, youth groups, and college. They can be given in either classroom or assembly settings.
Theology of Dance
Bleeding Hands, Weeping Stone
Why Reconciliation Rocks!
Why is Elizabeth, a convert, so on fire about the Sacrament of Reconciliation? Because God helped her understand the power and grace of this sacrament in an unforgettable way.
Lourdes: A Place of Miracles
Bernadette Soubirous was only fourteen years old when she encountered Our Lady. Her faith and determination to stand up for what she saw and heard in that grotto is an inspiring witness to young people everywhere.
Journey in Writing, Journey in Faith
All of us are on a journey, and all of us have a mission in building the Kingdom of God. Elizabeth shares some of her own journey and inspires young people in their journeys as well.
Receive my Newsletter
Is snow white or red?
About Elizabeth
- Register your Email
- Speaking Archive
Educating for democracy since 1945
- The Civic Outlook of Young Adults in America

- Civic Readiness Insights
- Gen Z Compared to National Baseline
- Politically Disengaged Gen Z
- Additional Research Materials
- Share to Twitter
- Share to Facebook
Download the executive summary and analysis of the survey results, including key findings and opportunities.
Press Release
View the press release and fact sheet about the survey results.
Get Updates
Be the first to hear about new civic learning research, tools, and opportunities.
The Institute for Citizens & Scholars believes today’s young adults are particularly poised to strengthen democracy. As we head into a Presidential election year and when more than 31 million 18–24-year-olds are shaping the future of our country, the time is now to unleash this generation’s civic potential.
Turning Warning Signs into Opportunities for Democracy
The Civic Outlook of Young Adults in America is a first-of-its-kind national survey of 18–24-year-old Americans that sheds light on their civic knowledge, civic engagement, and commitment to democracy. Part of our multi-year research initiative to measure holistic youth civic preparedness in America, Citizens & Scholars commissioned Citizen Data to conduct a poll that surveyed 4,008 young adults across the country.
Civic Knowledge
40% were able to correctly answer only one out of four civics questions
Civic Engagement
33% indicated no intention to participate civically in 2024, including voting
Civic Commitment
57% are dissatisfied with American democracy
The survey reveals a warning sign for American democracy. Americans aged 18 to 24 are dissatisfied with the political system and pessimistic about democracy, lack critical civic knowledge and trust in government institutions, and are less likely to vote in the 2024 election than the general population. However, there are grounds for optimism in this demographic. They exhibit a lower degree of ideological and partisan polarization, are proud to be American, reject political violence, and collectively prioritize democratic values.
The survey also confirms an important characteristic of young adults: their potential and motivation to play a vital role in strengthening democracy , but they must be engaged in a meaningful way. This will require talking to, learning from, and collaborating with Gen Z to understand what’s underneath the tensions present in these data on productive engagement and commitment to democracy.
Key Findings
How civically informed are young adults.
40% are able to correctly answer only one out of four standard civics questions. Only 4% answer all four questions right.
35% say they do not feel informed enough to participate politically.
How civically engaged are young adults?
33% of respondents indicate no intention to participate civically in 2024. This could include voting, political volunteerism, donating, event attendance, and digital content creation.
33% of respondents say they are not currently engaged in community activities, such as sports, hobbies, volunteerism, and faith groups.
48% of respondents intend to vote in the 2024 general election, significantly lower than the nationwide baseline of 68%.
How civically committed are young adults?
57% are dissatisfied with how the political system is functioning in the U.S.
40% are pessimistic about the future of our democracy compared to about a quarter who are somewhat or very optimistic.
52% report no trust at all or very little trust in government institutions.
51% oppose the use of violence to suppress dissent.
68% believe their vote matters.
70% are somewhat, very, or extremely proud to be American.
Where do young adults stand politically?
61% do not identify with either major political party. Of those, 29% identify as independent, nonpartisan, or other party, and 33% are unsure or do not identify politically in any way. Only 22% identify as Democrat and 17% as Republican.
51 % describe their ideology as at or near the ideological middle–moderate, somewhat conservative, or somewhat liberal. Only about one in four (27%) identifies as very conservative or very liberal.
66% state they are registered to vote.
This poll is a wake-up call. We urgently need to do more to civically prepare, activate, and support young adults. All of us must step up and play our part – from schools and employers to community and religious groups, from political parties and elected officials to parents and neighbors.

Key Opportunities
Gen z can help tackle polarization..
37% find conversations with those with different views to be interesting and informative. By contrast, 41% of Americans of all ages found such discussions to be stressful and frustrating.
51% opposed the use of violence to suppress dissent.
There is an opportunity to coalesce around shared values, as young adults say American democracy means equality (55%), justice (51%), and fairness (49%). They agree regardless of background, education, or ideology. Republicans and Democrats alike chose these values, and in the same order.
Schools won’t close the civic knowledge gap alone.
Given that 78% of young adults express trust in academic institutions, schools have a responsibility to play a leadership role in empowering young adults to help strengthen our democracy.
Community organizations, faith-based institutions, and employers should also help close the gap by incorporating foundational civic education into their programming.
Increasing civic knowledge could drive greater civic engagement.
80% of respondents who score high on civic knowledge plan to engage in at least one civic activity during 2024 versus 40% of low civic knowledge scorers.
Civic and community groups should work to engage the 33% of young adults who are not active in any community organizations.
Political parties and candidates can attract new supporters.
61% of young adults do not identify with either major political party. Only 22% identify as Democrat and 17% as Republican.
51% describe their ideology as at or near the ideological middle.
66% state they are registered to vote, but only 48% currently plan to vote in the next general election.
Explore the Survey Results

Analysis, Toplines & Crosstabs
Get access to the executive summary, key findings, toplines and crosstabs of the survey.

Youth Civic Readiness
Explore the strong correlation between increased civic knowledge with engagement and commitment in our democracy.

Gen Z’s Take: Election Year Voter Roundtable
Jessica Sutter sits down with two Gen Zers to get their thoughts on the findings of our survey.
Explore The Report
Stay engaged.
Join our mailing list to get resources, tools, perspectives, stories, and more from people working to cultivate the next generation of engaged citizens.
More Resources
Our Civic Learning Resource Hub is a one-stop-shop of the best reports, research, white papers, and other resources from around the civic space.
- Coronavirus updates
- Board of Directors
- Junior Board
- Youth Advisory Board
- Social Media
- Ways to Give Back
- Our Services
- Cost of Care
- Becoming Program
- Ask myHealth
- Birth Control
- Healthy Relationships
- STI Information
- Getting Tested
- Eating Disorders
- Drugs and Alcohol
- E-Cigarettes
- Community Resources
- Camp Middle School
Youth Presentations
- Parent Presentations
- Professional Development
- Appointments
- Search for: Search Button
myHealth for Teens & Young Adults’ education team is comprised of professional speakers that are knowledgeable about the issues teens and young adults face.
myHealth facilitates presentations in classrooms or any other community space. myHealth educators come out to schools, alternative learning centers, transition programs, juvenile detention centers, treatment facilities, dormitories, student groups, etc.
Our Presentations…
- are activity-based, provide resources and information on a variety of topics.
- use an evidence-informed, fact-based, medically accurate and trauma-informed approach to learning.
- are tailored to the unique needs of your students and serve to reinforce your site’s key messages.
- are typically 40-90 minutes in length. You can choose from one stand-alone presentation or pair a few together. We also offer psycho-educational youth development groups.
- are linked to MN Health Standards and Social and Emotional Learning Objectives.
- have a five-participant minimum.
Help us provide opportunities for young people to learn about their health, well-being and make educated decisions.
All topics are available as virtual presentations. We offer both synchronous (live) and asynchronous (pre-recorded).
Presentation Topics:
Click through the education topics to get a better idea of the presentations we offer. Should you choose to utilize myHealth’s presentations in your community, we will work with you to send a health educator from our team to facilitate the presentation to your youth.
Presentation Topics Key
- ES: Elementary School
- MS: Middle School
- HS: High School
Healthy Relationships (MS, HS, Transitions+, College)
Focusing primarily on romantic relationships, the lesson explores the differences between healthy and unhealthy relationships. Students can create their perfect partner and explore their values and needs. Students will identify traits that are important to them in a romantic relationship and learn to identify unhealthy traits in relationships. Students will learn about the cycle of abuse and how to advocate for themselves or someone else. This presentation provides resources on consent and bystander intervention.
Healthy Friendship (ES, MS, Transitions+)
The presentation explores the importance of healthy friendships and what it means to be a good friend. Students will identify what qualities are important to them in a friend, and behaviors that are healthy and unhealthy in friendships. Students will learn how to communicate effectively and navigate conflict in a respectful and safe manner.
Mental Health 101 (MS, HS Transitions+)
The presentation explores the importance of taking care of our mental health. Students will identify signs and symptoms of common mental health concerns like anxiety and depression. Students will learn how to communicate about mental health concerns and ways to ask for help. This presentation concludes with a review of many local and national teen friendly resources.
Social Media Safety (MS, HS, Transitions+, College)
Although we will be talking about technology, students will not need to have access to any technology. This lesson begins with discussing current trends in social media by using the expertise of the students in the room. It covers some of the common dangers of the internet: sexting, bullying, unwanted exposure to pornography, and personal information being shared. Students are encouraged to think about the positives and negatives of living in a “plugged-in” society. Students will also learn what can be done and who to go to if something negative does occur while online, and how positively navigate the internet and social media. This presentation can be adapted to the needs of younger and older aged students
Gender Norms and Body Image (ES, MS, HS, Transitions+, College)
This lesson is jam-packed with activities. Students will critically examine the beauty standards set forth by the media, and discuss why some groups are marginalized, portrayed negatively or totally invisible from mainstream pop culture. Focusing primarily on being a savvy media-consumer, students will realize that with the media, “what you see is not what you get.” Students will engage in an affirmation activity to boost self-esteem and create a positive self-image.
Healthy Boundaries (ES, MS, Transitions+)
This lesson covers virtual, physical and emotional boundaries, exploring what students are okay with and not okay with. Students will learn how boundaries can help maintain emotional and physical safety. As a group, students will define healthy boundaries for themselves, and how to communicate their boundaries with friends, family, peers, and strangers.
Consent (MS, HS, Transitions+, College)
Do you know the difference between flirting and sexual harassment? This presentation will define the word consent and provide a framework in which to engage self and others. Students will examine scenarios and look for ways to communicate consent with friends and partners, intervene as bystanders, and advocate for themselves and their community.
Vaping Awareness (MS, HS, Transitions+, College)
Among Minnesota high school students, e-cigarette use is now double conventional cigarette use. In this presentation, students will learn the truth about vaping and engage in activities that spark peer-led conversations on preventing vaping and other tobacco use. Students will identify the short and long-term effects e-cigarettes can have on a person’s health. This presentation concludes with practicing coping skills that provide stress relief as alternatives to vaping/tobacco use.
Five Circles of Wellness (MS, HS, Transitions+, College)
It is a young person’s job to develop a sense of identity, build a supportive community of peers, and hone healthy skills for wellness. This presentation breaks down wellness in five ways; academic health, self-care, and coping skills, mental health, physical health, and relationship health. Students will explore tough issues they face as young people together and locate ways to manage their “job” successfully.
Puberty (ES, MS)
Aimed primarily at students in the thick of puberty, this high-energy lesson focuses on re-assuring each young person that they are, in fact, “normal.” This presentation begins by asking students to explore their excitement and anxiety about growing up. Students learn about physical and emotional changes that occur during puberty as well as debunk common myths around becoming a teenager.
Stress Management (ES, MS, HS, Transitions+, College)
The goal is for students to be so relaxed that they fall asleep by the end of this presentation. Students will define their own coping skills, learn about physical and emotional responses to stress and effective ways to interrupt negative self-talk. The presentation concludes with myHealth educators leading a guided meditation and practicing healthy coping skills.
Gender, Sexuality and LGBTQAI+ 101 (ES, MS, HS, Transitions+, College)
Many community partners want to increase education for their students on this topic. In this lesson, students learn the definition of letters in the LGBTQIA+ and the importance of pronouns. Our educators will also work through the Gender Unicorn, discussing gender expression, gender identity, sex, and sexual orientation. Students will brainstorm and learn how we can make our schools and shared spaces inclusive and welcoming to all.
*Activities and learning objectives differ based on age and development needs. Please contact a myHealth educator with questions.
Safer Sex Methods (Including Abstinence) (HS, Transitions+, College)
Beginning with a short activity on abstinence, this presentation covers the methods of contraception most widely accepted in the US, and most commonly used by young people. These methods include both prescription (pill, ring, shot, the Nexplanon rod, IUD, and emergency contraception) and non-prescription or behavioral methods (condoms, dental dams, and other barrier methods, withdrawal and chance). Educators will also discuss sexually transmitted infection (STI) prevention and the importance barrier methods have in preventing the spread of STIs. If time allows, we also discuss unplanned pregnancy prevention myths and facts, and common barriers to accessing birth control or condoms. This presentation can include a condom demonstration, per the request of the teacher.
Sexually Transmitted Infections (STIs/STDs-Including HIV/AIDS) (MS, HS, Transitions +, College)
Students will learn about the three types of STIs (bacterial, viral and parasitic) and the five common STIs contracted by young people. Students will also learn about symptoms, testing, treatment, and prevention. Through engaging activities, educators will destigmatize STIs and emphasize communicating about STIs with a partner is normal and healthy. This presentation can include a condom demonstration, per the request of the teacher.
Sexual Decision Making (MS, HS, Transitions+, College)
Covering the various factors that influence a young person’s decision to engage in sexual activities and the common sources of pressure, this lesson allows for critical thinking about personal values and beliefs. We encourage students to determine and reflect on their personal boundaries and choices. Students engage in a “dating line up” which explores “steps” of dating, intimacy building and sexual activity as empowered choices. This presentation can include another activity where students create responses to common pressure lines, encouraging communication between partners and self-advocacy.
Abstinence (MS, HS, Transitions+, College)
This presentation focuses on factors that can influence a young person’s decision to be sexually active or not. We touch on the meaning of abstinence and ask students to define intimacy and boundaries for themselves. Our abstinence presentation does not use a prescribed amount of time that a person should wait before engaging in sexual activity. Instead, we provide evidence-informed, student-centered information and help young people realize that the decision is ultimately their own.
Hygiene and Anatomy (ES, MS, Transitions+)
This presentation explores the anatomy and how to maintain clean and healthy body parts. Students will partake in activities that discover the importance of a daily personal hygiene routine and the public or private locations that one can participate in positive hygienic behaviors. Who knew that taking care of your body could be so much fun?!
Anatomy (ES, MS, HS, Transitions+, College)
This presentation is all about reproductive anatomy. Students will create reproductive models out of household materials while learning the correct terms of body parts, and their functions. Make this presentation a series by pairing it with hygiene, puberty, or both!
Youth Development Groups (MS, HS, Transitions+, College):
In addition to classroom presentations, we facilitate small multi-session psycho-educational youth development groups with young adults. Groups are 5-8 weekly sessions and can extend through the semester or year. The safety of a smaller group allows comprehensive learning when discussing sensitive topics such as healthy relationships, goal setting, stress management, unplanned pregnancy prevention, safer sex methods, STI transmission, and prevention, etc.
To set up a presentation, email us with the following information!
- First & Last Name
- The school (Please include location and room number)
- Teacher/Site Contact (Name, phone number for day-of, email)
- Presentation Date & Time
- Class & Grade Level
- Approximate Number of Students (Attendees per Presentation)
- Presentation Topic(s)
- Technology Needs *If students have access to iPads, laptops or smartphones, please have students bring those to class, as we do ask students to fill out an online evaluation at the end of our presentation
If you have any questions about our presentations or are interested in our youth development groups, please contact Gabby:
Accessibility • Privacy Policy • Cookie Policy
© 2024 myHealth Clinic for Teens and Adults.
How to Practice Self-Care: 10+ Worksheets and 12 Ideas

But while it persistently grabs headlines, it also remains a fuzzy concept.
Though a relatively new phenomenon in the West, self-care has a much older tradition in Eastern cultures, reaching back to antiquity. Marked by a preventive rather than reactive approach to health, many Asian cultures seek to manage our energy economies before they become depleted.
The therapeutics of Traditional Chinese medicine, for example, revolve around preventing the exhaustion or blockage of “qi,” our vital life energy. Qigong, meditation, and yoga are all techniques designed to restore our inner balance and prevent us from burning out.
Combining self-soothing and relaxation with resilience-enhancing strategies, Western-style self-care, too, promotes a proactive approach to our physical and mental wellbeing (Skovholt & Trotter-Mathison, 2011).
Self-care is a sustainable and holistic investment in our minds and bodies. It includes taking good care of our physical health, most notably by eating healthily, exercising, and sleeping well. But it also entails looking after our minds and emotions, which can take the form of setting time aside for activities that nourish our spirits and learning to understand how we can best replenish our energies.
Before you continue, we thought you might like to download our three Self-Compassion Exercises for free . These detailed, science-based exercises will not only help you increase the compassion and kindness you show yourself, but will also give you the tools to help your clients, students, or employees show more compassion to themselves.
This Article Contains:
Why is self-care so important, our 5 favorite self-care worksheets, 3 worksheets for youths, the self-care assessment wheel, self-care activity ideas, emotional intelligence tools, a take-home message.
If we do not practice basic self-care, we may quite simply burn out . We will be unable to decompress or find outlets for our stressors. The worse we take care of ourselves, the less we will have to give. As the saying goes: ‘from an empty cup, we cannot pour.’
Often, self-care advice takes the form of prescribing specific relaxation activities to clients. But this misses the point. The true essence of self-care is twofold: it involves self-knowledge and positive self-talk .
First and foremost, we need to understand our true needs. What does and does not restore us differs substantially from person to person, depending on our tastes and preferences. Our key task is to stimulate our clients to reflect on what it is that they need – their own unique and special sets of self-care activities.
The second core part of self-care is about managing the way we talk to ourselves. Riegel and colleagues (2017) rightly highlights the importance of adjusting our self-talk as a crucial component of self-care. For there is nothing more energy draining and destructive than our inner critic, the bullying voice that tells us we are lacking.
To take better care of ourselves, we need to work on cultivating a kinder, more compassionate voice. Awareness raising and self-compassion (Neff, 2004), then, are the central features of self-care.
A solid starting point for embarking on a self-care journey is to take an inventory of how good we are at it already. This Self-Care Checkup breaks self-care down into physical, psychological, social, spiritual, and professional self-care. Checking how we score in each domain provides a good first indication for what we should prioritize.
An even better first calling point is PositivePsychology.com’s Self-Care Check-in , which invites us to see where more attention is needed to ensure we are addressing our self-care needs. It reminds us of the importance of taking active steps to maintain our mental wellness, and helps us identify where we should focus our attention to satisfy our unmet needs.
A few example self-care domains listed on this sheet are listed below:
- Quality time with family
- Friendships
- Opportunities to engage in pleasurable activities.
Given that self-compassion is such a vital part of any self-care regime worth its salt, another great stock-taking worksheet is PositivePsychology.com’s Letter of Self-Compassion. It reminds us that we are often too hard on ourselves and it is sometimes necessary to take a more forgiving, accepting, and caring attitude to ourselves and others.
An excellent resource for self-compassion-based self-care exercises is Kristin Neff’s website . Her How would you treat a friend? worksheet is particularly significant. It urges us to remember how we would interact with a struggling friend. What would we say to them? What tone of voice would we use?
Next, we are invited to think of how we speak to ourselves when we are struggling. Is there a difference between the way we talk to ourselves and the way we would speak to a friend we care about? If so, why? The aim is to treat ourselves with as much care and kindness as we would treat our friends.
In her Changing Your Critical Self-Talk exercise, Neff invites us to notice when we are talking to ourselves in a critical voice. Whenever we feel bad, we are asked mindfully to notice that voice – what it says, which phrases it uses, its tone, and whether, perhaps, it reminds us of someone in our past.
As a next step, Neff asks us to soften this inner judge and to reframe the observations it makes in a friendlier, more positive way. We may even want to supplement endearing and understanding self-talk with warm physical gestures.

These three exercises are designed to help youths think about how they can incorporate more self-care activities into their daily lives, for increased mental and physical wellbeing.
Self-Care Vision Board
PositivePsychology.com’s Self-Care Vision Board is particularly well suited for younger clients. This tool is available for free as part of our three Self-Compassion Exercises Pack, which you can download here .
Designed to increase self-care and self-compassion in creative ways, it adopts a playful and intuitive approach to the topic.
Clients are invited to create a self-care vision board. It can be drawn or combine cut-out images, photographs, and words. Clients are asked to brainstorm as many positive self-care activities as possible – both activities in which they are already engaging and those they would like to develop.
They are asked to work intuitively rather than rationally, to discuss their representations with their therapists, and then to place the vision board in a prominent place where it reminds them of all the great things they could do to take better care of themselves.
My Self-Care Promise
Another fantastic exercise, for both the young and the old, involves making a simple self-contract.
Self-care is one of the first sets of activities that get neglected when suffering from symptoms of anxiety or depression, and planning pleasant activities can encourage us to reflect on our strengths.
My Self-Care Promise invites the reader to consider times they may be vulnerable to waning self-care. It includes space for a re-affirming mantra to remind them to treat themselves compassionately and invites some ‘if–then’ thinking for when obstacles arise.
Nurturing vs. Depleting Activities
The things we do each day can either enhance or take away from our wellbeing in the long run. While we all find ourselves doing things we ‘need’ to do (e.g., work, looking after others, or running errands), it can be particularly easy to neglect the things that give us life and energy.
The goal of this Nurturing vs. Depleting Activities worksheet is to help the reader become more aware of what adds to or takes away from their mood and energy.
To complete the exercise, the reader is invited to list their daily tasks from morning to evening.
Next, they decide whether each activity is nurturing (energizing, positive, and restorative) or depleting (draining their energy and happiness).
Download 3 Free Self-Compassion Exercises (PDF)
These detailed, science-based exercises will equip you to help others create a kinder and more nurturing relationship with themselves.
Download 3 Free Self-Compassion Tools Pack (PDF)
By filling out your name and email address below.
Self-care assessment wheels are excellent tools for several reasons.
- First and foremost, they powerfully visualize the different domains of self-care.
- Secondly, they show us, at a glance, a more holistic picture of how we are faring in caring for ourselves.
- Thirdly, they remind us that all of the domains of self-care are interconnected, and that as a person, we are defined by how we do in all the relevant areas.
Frequently, the areas covered in self-care assessment wheels include the physical, psychological, emotional, spiritual, personal, and professional spheres.
Assessment wheels are particularly useful for illustrating the importance of balance between these areas in our lives. The best and most widely used self-care assessment wheel is Olga Phoenix’s Self-Care Wheel . It consists of two sheets, one in which general relevant topics have been inserted into the wheel, as inspiration and prompts, and one empty wheel for the client to fill out.
If we want to be less directive and allow our clients to use this wheel more intuitively, we can simply present them with the empty wheel only.
The list of commonly recommended self-care rituals tends to be topped by nutritional and sleep hygiene advice, and also features walks in nature, taking up hobbies, scheduling “me-time,” various relaxation techniques, and making more time for friends.
It also frequently includes sensual rituals such as bathing, pampering ourselves with luxurious beauty products, and lighting scented candles.
But prescribing specific activities to our clients misses the point. For self-care is all about finding out what we need – what our unique energy-draining and energy-boosting strategies are. They will differ in each case, often substantially. What reenergizes an extrovert, for example, may well drain an introvert even further.
The clue, then, is to draw up our unique list of our favorite things. We may take inspiration from the famous Sound of Music song:
Raindrops on roses and whiskers on kittens Bright copper kettles and warm woolen mittens Brown paper packages tied up with strings These are a few of my favorite things
Cream colored ponies and crisp apple strudels Doorbells and sleigh bells and schnitzel with noodles Wild geese that fly with the moon on their wings These are a few of my favorite things
To paraphrase Julie Andrews, when life stings, and we are feeling sad, we can simply remember our favorite things, and then we won’t feel so bad.
My personal list of favorite self-care things includes the following 12 items:
- Practicing balanced breathing for 10 minutes. All you need to do is sit comfortably, with an upright spine, and breathe in on your count of six, and then breathe out on your count of six. It is one of the most simple and powerful exercises I know for changing one’s state.
- Drinking in the colors of all the beautiful flowers and trees when walking in nature.
- Standing with my feet in the shore, where the waves break and foam, looking out to sea and filling my lungs deeply with salty air.
- Remembering all the things I am grateful for.
- Watching my two cats practice self-care; they are the true masters of the art. All day long, they sleep, clean, and groom themselves. They play, seek the sun, stretch, purr, and demand cuddles whenever they feel like it.
- Going for a run along the river listening out for birdsong.
- Playing Pachelbel’s Canon in D major on the piano.
- Singing along at the top of my voice to songs I used to love as a teenager (I won’t tell which ones 😉 ).
- Watching films that make me cry.
- Having coffee with a friend.
- Cuddling my daughter.
- Applying my favorite body lotion all over my skin. Its orange-infused cedar-almond scent reminds me of a holiday in Tuscany when we were all serenely happy. There is nothing as significant as smell for activating memories and associated positive emotional states.
As my list hopefully shows, our self-care lists will be highly specific and will not work for others. Our aim always has to be to stimulate our clients to draw up their own unique lists.

To understand what drains and what replenishes us, we also need to have a basic understanding of our dominant emotional patterns.
In Emotional Intelligence: Why It Can Matter More Than IQ , the American psychologist Daniel Goleman (1995) defines the core components of emotional intelligence as self-control , persistence, and the ability to motivate ourselves; combined with the ability to empathize and read emotions in others; and, crucially, an understanding of our core emotional processes.
Insights into our emotional habits yield greater self-mastery.
The keystone of emotional intelligence – and a crucial prerequisite both to self-understanding and the ability to care well for ourselves – is knowing our emotions. It is a form of meta-self-awareness that is manifest in “recognizing a feeling as it happens.”
For the “ inability to notice our true feelings leaves us at their mercy ,” Goleman writes (1995, p. 43). Those of us who know our feelings are generally better pilots of our lives. There is a crucial difference between simply being caught up in a feeling and developing a metacognitive awareness that we are being submerged by this feeling.
Objective self-observation is, therefore, the key to knowing our emotional selves. Such self-observation entails stepping back from our experience and cultivating an awareness of our conscious thought that hovers above rather than becoming entangled in it.
Two great emotional intelligence tools for enhancing emotional self-knowledge are Emotional Awareness and Emotional Expression . The first exercise allows you to log your emotions throughout the day to improve awareness and become more attuned with your triggers and emotional responses.
The Emotional Expression exercise helps clients to walk through their emotional responses to imagined experiences. It gives clients a helpful and practical way to practice expressing their feelings to others, which is a helpful strategy for coping with stress.
If you’re looking for more science-based ways to help others develop self-compassion, this collection contains 17 validated self-compassion tools for practitioners. Use them to help others create a kinder and more nurturing relationship with the self.
17 Exercises To Foster Self-Acceptance and Compassion
Help your clients develop a kinder, more accepting relationship with themselves using these 17 Self-Compassion Exercises [PDF] that promote self-care and self-compassion.
Created by Experts. 100% Science-based.
The art of taking good care of ourselves includes some basics; eating and sleeping well, getting regular exercise, and paying attention to our breath are among them, and ensuring that our self-talk is kind is also key.
Other than that, we should refrain from prescribing specific activities to our clients. Self-care means very different things to different people. As the ancients in Asia knew well, self-care is essentially about managing our energy wisely.
Truly understanding what drains us and what restores us is crucial in this process. Our task as psychologists and coaches is to create awareness in our clients about what works for them.
Self-knowledge, including emotional intelligence, is thus a crucial precondition for self-care. It may be that yoga or knitting will help us to refuel, but it can just as well be kickboxing or kitesurfing.
Introverts will cherish alone-time activities, while extroverts may reenergize by being with others. So let us not recommend that people light scented candles or take bubble baths, but rather encourage them instead to understand their unique needs and how to meet them – whatever these may be.
We hope you found this article useful. Don’t forget to download our three Self-Compassion Exercises for free .
- Goleman, D. P. (1995). Emotional intelligence: Why it can matter more than IQ for character, health & lifelong achievement. New York, NY: Bantam.
- Kashdan, T. B., Barrett, L.F., & McKnight, P. E. (2015). Unpacking emotion differentiation: Transforming unpleasant experience by perceiving distinctions in negativity. Current Directions in Psychological Science , 24 (1), 10-16.
- Neff, K. (2004). Self-compassion and psychological well-being. Constructivism in the human sciences , 9 (2), 27-37.
- Riegel, B., Dickson, V. V., Garcia, L. E., Creber, R. M., & Streur, M. (2017). Mechanisms of change in self-care in adults with heart failure receiving a tailored, motivational interviewing intervention. Patient Education and Counseling , 100 (2), 283-288.
- Schwartz, T. & McCarthy, C. (2007, October). Manage your energy, not your time. Harvard Business Review . Retrieved from https://hbr.org/2007/10/manage-your-energy-not-your-time
- Skovholt, T. M., & Trotter-Mathison, M. (2011). Counseling and psychotherapy: Investigating practice from scientific, historical, and cultural perspectives. The resilient practitioner: Burnout prevention and self-care strategies for counselors, therapists, teachers, and health professionals (2nd ed.). New York, NY: Routledge.

Share this article:
Article feedback
What our readers think.

Thank you very much ,itcame at the right time as we had a training yesterday emphasising on what are we doing daily to derailt ourselves.This activities will be valuable daily for one to use inoder to look forward to the next day

Good article. Thanks

Appreciate the worksheets.

Thank you for the worksheets!

Really great knowledge I have gained. I learned so much about self compassion.

Hi Meenu, So glad you found these resources helpful. Thanks for being a reader! – Nicole | Community Manager

Greetings Dr. Schaffner! Wonderful article! Thank you so much for sharing all the amazing self-care resources available for us to use, especially during these times. Thank you for sharing the Self Care Assessment Wheel as well and your kind words! I greatly appreciate it. I wanted to reach out and request Self-Care Wheel to be linked to my Self-Care Wheel website page: http://www.olgaphoenix.com/key-offerings/self-care-wheel/ . It contains additional information, Self-Care Wheels translated in other languages, downloadable resources, etc. The current link mentioned in this article is to 3rd non-affiliated party website. Thank you so very much for all your work! In deep gratitude, Olga Phoenix
Hi Olga, Thanks for reaching out to us. Yes, it certainly makes sense to link your original source. I’ll notify our editing team and get this link amended 🙂 – Nicole | Community Manager
Hi Nicole! Thank you so very much! Your time and work is greatly appreciated! Olga Phoenix

I really liked the way the video was put together…I understand the importance of a self-care
Hi Yvette, So glad you enjoyed the resources here. We offer a tool on the topic of self-compassion (which is an important part of self-care) which may be of interest to you. This tool is available for free download here . – Nicole | Community Manager
Let us know your thoughts Cancel reply
Your email address will not be published.
Save my name, email, and website in this browser for the next time I comment.
Related articles

Social Identity Theory: I, You, Us & We. Why Groups Matter
As humans, we spend most of our life working to understand our personal identities. The question of “who am I?” is an age-old philosophical thought [...]

Discovering Self-Empowerment: 13 Methods to Foster It
In a world where external circumstances often dictate our sense of control and agency, the concept of self-empowerment emerges as a beacon of hope and [...]

How to Improve Your Client’s Self-Esteem in Therapy: 7 Tips
When children first master the expectations set by their parents, the experience provides them with a source of pride and self-esteem. As children get older, [...]
Read other articles by their category
- Body & Brain (49)
- Coaching & Application (57)
- Compassion (26)
- Counseling (51)
- Emotional Intelligence (24)
- Gratitude (18)
- Grief & Bereavement (21)
- Happiness & SWB (40)
- Meaning & Values (26)
- Meditation (20)
- Mindfulness (45)
- Motivation & Goals (45)
- Optimism & Mindset (34)
- Positive CBT (28)
- Positive Communication (20)
- Positive Education (47)
- Positive Emotions (32)
- Positive Leadership (18)
- Positive Parenting (4)
- Positive Psychology (33)
- Positive Workplace (37)
- Productivity (16)
- Relationships (46)
- Resilience & Coping (36)
- Self Awareness (21)
- Self Esteem (38)
- Strengths & Virtues (32)
- Stress & Burnout Prevention (34)
- Theory & Books (46)
- Therapy Exercises (37)
- Types of Therapy (64)
3 Self-Compassion Tools (PDF)
Adolescents and Young Adults

While sexually transmitted diseases (STDs) affect individuals of all ages, STDs take a particularly heavy toll on young people. CDC estimates that youth ages 15-24 account for almost half of the 26 million new sexually transmitted infections that occurred in the United States in 2018. The resources on this page provide information about the impact of STDs on youth as well as resources for reaching this population.
Confidentiality Issues and Use of Sexually Transmitted Disease Services Among Sexually Experienced Persons Aged 15–25 Years — United States, 2013–2015 – MMWR March 10, 2017
2021 STI Treatment Guidelines – Adolescents – STI screening and treatment information for youth and young adults. (July, 2021)
Talking with Your Teens about Sex: Going Beyond “the Talk” pdf icon (November 20, 2014)
Adolescents, Technology and Reducing Risk for HIV, STDs and Pregnancy – White paper provides an overview about the ways in which digital technology can be used to improve the sexual health of adolescents. (August 8, 2013)

Let’s Talk About Sexual Health – Video for doctors and young adults on how to talk about sexual health. (November 30, 2012)
Podcast: STD Awareness: Reaching Youth – Dr. Gail Bolan, Director of CDC’s Division of STD Prevention, discusses the role healthcare providers play in educating young patients about sexual health and STD prevention. (April 16, 2012)
STI Prevalence, Incidence, and Cost Estimates : 1 in 5 people in the United States had an STI on any given day in 2018. These updated estimates provide the clearest picture to date of how common and costly STIs are in the United States. (January 25, 2021)
Just Diagnosed? New fact sheet provides the three steps you can take if you were recently diagnosed with gonorrhea or chlamydia, including resources to help you talk to your partner. (August 3, 2017)
STD Fact Sheets – Disease-specific information about symptoms, prevention, and treatment.
Know your CONDOM DOs & DON’Ts pdf icon
- Ways to Prevent STDs
- HIV Among Youth
- Adolescent and School Health
For Public Health Professionals
- STD on Twitter
- STD on Facebook
Exit Notification / Disclaimer Policy
- The Centers for Disease Control and Prevention (CDC) cannot attest to the accuracy of a non-federal website.
- Linking to a non-federal website does not constitute an endorsement by CDC or any of its employees of the sponsors or the information and products presented on the website.
- You will be subject to the destination website's privacy policy when you follow the link.
- CDC is not responsible for Section 508 compliance (accessibility) on other federal or private website.

Young Adulthood
Jul 09, 2014
1.38k likes | 3.24k Views
Young Adulthood . The adult phase of development encompasses the years from the end of adolescence to death: Young adulthood 20 – 40 Middle adulthood 40 – 65 Late adulthood over 65. Maturity: the state of maximal function and integrating or the state of being fully developed.
Share Presentation
- late adulthood
- dental maturity
- operational thought
- primary factor
- glomerular filtration rate

Presentation Transcript
The adult phase of development encompasses the years from the end of adolescence to death: • Young adulthood 20 – 40 • Middle adulthood 40 – 65 • Late adulthood over 65
Maturity: the state of maximal function and integrating or the state of being fully developed. • Mature persons are open to new experiences and continued growth • They can tolerate ambiguity, are flexible, and can adapt to change
Mature persons also assume responsibility for themselves, make decisions and accept responsibility for these decisions • This is a period of exploration • Trying out new possibilities for a career. • It is a period of escaping from parental domination (Psychological separation from parents) • Substituting friends for family
Friendship is important throughout the life span • Friendship is a form of close relationship providing people with • Enjoyment • Acceptance • Trust, respect, and mutual assistance • Confidences shared and a sense of understanding
Young adults are typically busy people • They are expected to assume new roles at work, in the home and in the community and to develop interests, values and attitudes related to these roles. • Deciding whether or not to have children
Establishing adult relationships with parents • Acquiring marketable skills • Choosing a career • Using money to further development • Assuming a social role • Adopting ethical and spiritual values
Physical development: Twenties • The prime years physically • The musculoskeletal system is well developed and coordinated • This is the period when athletic activities reach their peak • All other systems of the body are also functioning at peak efficiency
Body shape and proportions finally reach their finished state (physical changes are minimal), with the exception of: • weight and body mass as they may change as a result of diet and exercise • Extensive physical and psychosocial changes occur in pregnant and lactating women
Muscles continue to gain strength throughout the twenties and reach peak strength at age thirty depending on exercise and genetic • Men have larger muscles that can produce more force than the muscle tissue of women.
Dental maturity is finally achieved in the twenties with the emergence of the last four molars called wisdom teeth • The reproductive systems are fully mature: best time for reproducing children • Brain cell development reaches its peak
Physical development: Thirties • Physically adults begin to gradually slow down in their thirties • Muscle size and strength can be maintained with regular exercise. Without it muscles begin a progressive decline • Skin begins to lose its resilience and elasticity. Both women and men begin to notice wrinkles in their thirties.
Hair may grow more slowly, be lost or occasionally lose its pigmentation (grey hair) • Genetic predisposition toward baldness or early greying • Gradual shrinking of the brain cells after about age thirty (not a cause of great concern) • While visual acuity remains stable through middle age, hearing begins to decline in the late 20s.
Erik Erikson: psychosocial development • Establishing Intimacy • Erikson’s stage of Intimacy vs. Isolation is the psychosocial challenge of young adulthood. • Choices must be made about education and employment, marriage and having children
Intimacy should occur after one is well into establishing a stable and successful identity • Failure to achieve intimacy results in social isolation • Intimacy’s most important aspect is commitment • Research shows that some women resolve intimacy issues after their children have grown and moved away.
What motivates one to be attracted to another? • People actively seek out others to associate with • Familiarity is necessary for a close relationship • People seek others who are similar to themselves but opposites do attract in certain instances • Physical attractiveness may not be the primary factor in establishing and maintaining a relationship • Standards of what is attractive are always changing over time and across cultures
Cognitive Development • Cognitive structures are complete during formal operation period • Piaget: adolescents and adults think qualitatively in the same way – formal operational thought • Others believe idealism decreases as young adults enter world of work and face constraints of reality • Other researchers have found differences in how adolescents and adults process information.
Researchers have suggested a fifth higher stage of cognitive development that may follow formal operations, Post-formal operations: they are able to comprehend the contradictions (love & hate) that exist in both personal and physical reality
Postformal operations • Part of postformal thinking is the recognition that individuals’ experiences differ and will therefore result in different ways of thinking about things. • In postformal thinking there is a recognition of the importance of emotion integrated with logic in decision-making.
Health problems • Accidents: leading cause of death • Suicide • Hypertension • Smoking • Smoking is the leading contributor to health problems. • Nicotine is a known potent teratogen. • Quitting smoking is usually beneficial, regardless of how or when it happens.
Health problems • Substance abuse • Sexually transmitted disease • Abuse of women • Malignancies • Infertility
Middle adulthood 40 – 65 years
Physical changes • Appearance: • Hair begins to thin, and grey hair appears • Skin turgor and moisture decreases • Subcutaneous fat decreases and wrinkling occurs • Fatty tissue is redistributed, resulting in fat deposits in the abdominal area “spare tire” • Nail & hair growth slows • Baldness
Musculoskeletal system: • Skeletal muscle bulk decreases at about age of 60 • As the cartilage between the vertebrae starts to degenerate from normal wear, the vertebrae become compressed and the spinal column gradually begins to shorten causes a decrease in height of about 2.5 cm • Calcium loss from bone tissue is more common among post-menopausal women • Bones lose mass and density, break more easily and heal more slowly
Joint pain may be caused by deterioration of the bones under the cartilage in a condition known as osteoarthritis. • A more common form of arthritis is rheumatoid arthritis which is a destructive disease of the joints causing pain. • During middle age, adults may begin taking anti-inflammatory medications and either steroidal, or non-steroidal drugs. • Muscle growth continue in proportion to use
Cardiovascular system: • Blood vessels lose elasticity and become thicken • The ability of the heart muscle to contract decreases leading to a lower cardiac output • Respiratory system: • Lung and bronchi become increasingly less elastic, causing a progressive decrease in maximum breathing capacity • It takes individuals longer to catch their breaths after exercise
Sensory perception: • Visual acuity declines, often by late forties, especially for near vision (presbyopia) • Hearing loss limited first to high pitches sounds (presbyacusis) particularly in men cause persons to stand or sit closer to the source of sound, they may strain to hear or may talk in compensatory louder tones • Taste sensation also diminish
Metabolism: • Slows resulting in weight gain commonly in the wall of the abdomen, the hips, thighs and chest wall • Gastrointestinal system: • Gradual decrease in the process of digesting, absorbing and eliminating food may predispose the individual to constipation • Urinary system: • Nephron units are lost during this time and glomerular filtration rate decreases
Reproductive changes: • Hormonal changes take place in both men and women • The reproductive organs of both men and women begin to atrophy • The end of the female reproductive cycle is relatively clearly marked the menopause
Menopause: • Usually occurs between age of 40 – 55 years (average 47 years) • Ovarian activities declines until ovulation ceases • Two processes are often seen associated with menopause. • Estrogen-related symptoms: hot flashes, night sweats, vaginal dryness, and urine leakage. • Somatic symptoms: sleep problems, headaches, rapid heart-beat, stiffness or soreness in the joints. • Climacteric (Andropause) • The change of life in men when sexual activity decreases • Less gradual and less obvious than menopause in women
Psychosocial development • Erikson: Generativity vs. stagnation • Generativity: • The concern for establishing and guiding the next generation • Increase concept of service to others and love and compassion: social work, political work, community fund-raising • Marriage can be more satisfying • Feel a sense of comfort in their lifestyle
Stagnation: • People who are unable to expand their interests at this time suffer a sense of boredom and stagnation • Have difficulty in accepting their aging bodies and become withdrawn and isolated • Preoccupied with self and unable to give to others • Some may regress to younger behaviour in dress or actions or marrying younger partners
Cognitive development • Learning continues and can be enhanced by increased motivation at this time • The experiences of the professional, social, and personal life will be reflected in their cognitive performance thus approaches to problem solving and task completion will vary considerably
Cognitive Development Does intelligence decline with age? • Cross-sectional studies - which test people of different ages at the same point in time - clearly showed that older subjects scored less well than younger subjects on traditional IQ tests. • Intelligence peaks at 18, stays steady until mid-20s, and declines till end of life.
Crystallized & Fluid Intelligence • Many researchers believe there are two kinds of intelligence. • FLUID INTELLIGENCE: is defined as one’s reasoning and problem solving abilities, independent from the culture and the environment. • It is the ability to deal with new problems and situations • Fluid intelligence does decline with age.
(Crystallized & Fluid Intelligence, continued) • CRYSTALLIZED INTELLIGENCE is the store of information, skills, and strategies that people have acquired through education and prior experiences, and through their previous use of fluid intelligence. • Crystallized intelligence includes numerical and verbal abilities, such as solving a crossword puzzle or a mathematical problem. • Crystallized intelligence holds steady or increases with age.
Changes in Crystallized & Fluid Intelligence
Professional success may not rely exclusively on cognitive ability. • Older, successful people may have developed expertise in their particular occupational area or SELECTIVE OPTIMIZATION,the process by which people concentrate on particular skill areas to compensate for losses in other areas.
Memory in Middle Adulthood • According to research on memory changes in adulthood, most people show only minimal losses, and many exhibit no memory loss in middle adulthood. • Memory is viewed in terms of three sequential components…
Memory in middle adulthood, continued • Sensory memory is an initial, momentary storage of information that lasts only an instant. • No decline in middle age. • Short-term memory holds information for 15 to 25 seconds. • No decline in middle age. • Long-term memory holds information that is rehearsed for a relatively permanent time. • Some decline in middle age. • storage is less efficient • a reduction in efficiency of memory retrieval
Nutrition • As metabolic rate decreases, food intake should be adjusted accordingly. • If wise eating habits were not followed earlier in life, the body may start giving its owner messages of disease. Heartburn, ulcers, colitis, high blood pressure -- all these and more are at least partially caused by poor diet and poor digestion
Health problems • Life style patterns, aging, family history, developmental stressors, situational stressors are related to health problems • CVD • Cancer • Accidents: Due to decreases reaction time and visual acuity
Heart Disease in Middle Adulthood • More men die in middle age of diseases of the heart and circulatory system than any other cause. • Both genetic and experiential characteristics are involved. • Heart disease runs in families. • Men are more likely to suffer than women, and risks increase with age.
According to the American College of Sports Medicine and the Centers for Disease Control and Prevention, every adult should get at least 30 minutes of moderate-intensity physical activity daily. • walking • gardening • climbing stairs • reduces risk of heart disease, osteoporosis, weight gain, and hypertension • psychological benefits of sense of control and well-being
Heart disease, continued • There are several environmental and behavioral risk factors for heart disease. • cigarette smoking • high fat and cholesterol in diet • lack of physical exercise
The Type A’s and Type B’s personality • Evidence suggests that some psychological factors are also related to heart disease. • People with TYPE A BEHAVIOR PATTERN,which is characterized by competitiveness, impatience, and a tendency toward frustration and hostility, are more susceptible to heart disease.
(type A behavior, continued) • They engage in multiple activities carried out simultaneously. • They are easily angered and become verbally and nonverbally hostile if prevented from reaching their goals. • Heart rate and blood pressure rise, epinephrine and norepinephrine increase. • Most experts now say it is the negative emotion and hostility that are the major links to heart disease.
Type B’s and heart attack risk • By contrast, people with TYPE B BEHAVIOR PATTERN,which is characterized by noncompetitiveness, patience, and a lack of aggression, have less than half the risk of coronary disease that Type A people have. ~ Not all type A’s are destined to suffer heart disease! ~ Can learn to behave differently
Stress in Middle Adulthood • Stress continues to significantly impact health during middle adulthood • Stressors themselves may be different • 3 main consequences… • Direct physiological effect • Harmful behaviors • Indirect health related behaviors
- More by User

Adulthood. Where we are going…. Physical Changes. Physical Peak is 18-35 Hair starts to gray around 40 Hair Thins out Weight gain because of less activity Wrinkles appear Bags under eyes Notable differences in walking and strength. Physical Changes. Health Issues.
883 views • 40 slides

Physical and Cognitive Development in Young Adulthood
Physical and Cognitive Development in Young Adulthood. Dr. Arra PSY 232. Young Adulthood (22 – 40). Piaget Cognitive development beyond formal operational stage Postformal thought Acknowledged by Piaget. Young Adulthood. Perry’s Cognitive Theory (1970, 1981) Interviewed college students
1.22k views • 18 slides

Young Adulthood to Late Life
Young Adulthood to Late Life . Emotional Development. **Levenson’s seasons of life** ** Vaillant: intimacy & career consolidation. Birth. Death. 20. 25. 35. 30. What experiences do you expect to have in in your 20s & 30s?. Birth. Death. 40. 45. 55. 50.
380 views • 18 slides

Independence and Young Adulthood
The state or quality of being independent; freedom from dependence; exemption from reliance on, or control by, others; self-subsistence or maintenance; direction of one's own affairs without interference. Self sufficiencyNot the same as isolation. Definitions of Independence. It's easy to be ind
199 views • 18 slides

Young Adulthood. Psychosocial Development. PERSONALITY DEVELOPMENT . Normative-stage models : a definite sequence of age-related changes. Timing-of-events model : a response to the expected or unexpected occurrence and timing of important life events. Trait models :
581 views • 17 slides

SCHAIE Adult Stages: Young Adulthood
SCHAIE Adult Stages: Young Adulthood. Transition to adulthood marked by end of schooling, working/becoming financially independent, living apart from family, marriage, and parenthood. Erikson’s stages: Trust versus mistrust Autonomy versus shame, doubt Initiative versus guilt
1.03k views • 28 slides

Young Adulthood: Love and Work
Young Adulthood: Love and Work. “ Lieben und artbeiten .” ~Sigmund Freud. Transition to Adulthood. Accepting responsibility for oneself Making independent decisions Becoming financially independent Intimacy versus isolation is central conflict according to Erikson
408 views • 24 slides

Adulthood. Early Adulthood. Middle Adulthood. Late Adulthood. Physical Changes. All physical abilities essentially peak by our mid twenties. Physical Milestones. Menopause: the natural ending of a woman’s ability to reproduce. There are physical symptoms led by a lack of estrogen.
549 views • 14 slides

Adulthood. S. Richards Spring 2010 . Young Adulthood. Age 20 – Age 40 Desire to try new ways of doing things and by changing relationships with parents. Learning to become less dependent and take responsibility for yourself. . Young Adulthood.
1.26k views • 31 slides

Markers of Adulthood and the Dreams of Young Adulthood
Markers of Adulthood and the Dreams of Young Adulthood. t erri martinson elton , phd. |dreams |. Share a story about a young adult in your life… In their 20s In their 30s In their 40s What are their issues? What are their joys?. What’s a Robust Faith ?. 8 facets (Parks)
369 views • 16 slides

YOUNG ADULTHOOD
YOUNG ADULTHOOD . 18 – 40 Years of Age. Introduction.
310 views • 12 slides

Forming Relationships in Young and Middle Adulthood
Forming Relationships in Young and Middle Adulthood . Chapter 11. Friendship. Based in feeling, reciprocity, choice Less emotionally, intense than romantic Help self-esteem, self-awareness, self-respect Facilitate socialization in adulthood. Adult Friends. Stages (ABCDE) Acquaintanceship
896 views • 34 slides

Chapter 10: Young and Middle Adulthood
Chapter 10: Young and Middle Adulthood. Becoming an Adult: Physical, Cognitive, and Personality Development. What role transitions mark entry into adulthood in Western societies? How do non-Western cultures mark the transitions to adulthood?
874 views • 23 slides

SCPHRP’s Adolescence and Young Adulthood Working Group
Evidence base for tackling health inequalities in transition services and critical transition periods. Ruth Jepson, Senior Scientific Advisor, Scottish Collaboration for Public Health Research and Policy (SCPHRP ) John McAteer , SCPHRP.
283 views • 17 slides

Young Adulthood. Te Piataata Trust . Maori concepts of development in adolescence – Rangitahi 1. Marae Atea/ Whare Tupuna – the physical heart of whanau Turangawaewae – a place to stand Whatumanawa –the emotional dimension Mana ake – positive and unique identity
873 views • 47 slides

Young Adulthood Developmental Tasks
Young Adulthood Developmental Tasks. Young Adults Population. Population of young adults ages 18-25 was over 29 million in 2004 Young Adult by Race/Ethnicity, 2000. 2.1%. 4.4%. 0.8%. Source: U.S. Census, 2000. Substance Use. past month use: 40% reported any cigarette use
594 views • 7 slides

UNIT 7 – Young Adulthood Chapter - 10
UNIT 7 – Young Adulthood Chapter - 10. Michelle Fischer, ACSW, LSW, MSW HN144. GOOD NEWS!! . No quiz this week! Let’s take a quick look at the directions for your project this week. Eco-Map Project Details.
499 views • 30 slides

Ch.12 Sect.1:Young Adulthood
Ch.12 Sect.1:Young Adulthood. Age 20-40 During 20s and early 30s… Height of Cognitive Powers Learn to become… Goal for men Women… Reevaluate decisions in 30s Ask themselves… Major life changes Women in their 30s concerned with childbearing Women feel…
223 views • 15 slides
Got any suggestions?
We want to hear from you! Send us a message and help improve Slidesgo
Top searches
Trending searches

teacher appreciation
11 templates

cybersecurity
6 templates

spring season
34 templates

archaeology
45 templates

46 templates

23 templates
Young People Theme
Young people theme presentation, free google slides theme, powerpoint template, and canva presentation template.
Download the "Young People Theme" presentation for PowerPoint or Google Slides and start impressing your audience with a creative and original design. Slidesgo templates like this one here offer the possibility to convey a concept, idea or topic in a clear, concise and visual way, by using different graphic resources. You need to talk about a specific topic, but you don't know how to do it? Try using presentations like this one here, 100% customizable!
"### Features of this template
- 100% editable and easy to modify
- Different slides to impress your audience
- Contains easy-to-edit graphics such as graphs, maps, tables, timelines and mockups
- Includes 500+ icons and Flaticon’s extension for customizing your slides
- Designed to be used in Google Slides, Canva, and Microsoft PowerPoint
- Includes information about fonts, colors, and credits of the resources used"
How can I use the template?
Am I free to use the templates?
How to attribute?
Attribution required If you are a free user, you must attribute Slidesgo by keeping the slide where the credits appear. How to attribute?
Related posts on our blog.

How to Add, Duplicate, Move, Delete or Hide Slides in Google Slides

How to Change Layouts in PowerPoint

How to Change the Slide Size in Google Slides
Related presentations.

Premium template
Unlock this template and gain unlimited access

Register for free and start editing online

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
Money Smart
Money Smart for Young People
Vea esta página en español
- An educator guide, student handouts, and powerpoint slides
- Multiple lessons that can be taught alone or in combination
- Standards alignment charts
- Ideas for grade-level modification
- Real-life exercises and examples
- Suggestions for optional books or online games/tools that can reinforce student understanding
- Ideas to integrate into existing academic subjects such as English, Mathematics, and Social Studies
FDIC Money Smart News for Kids was based on the Money Smart for Young People, grades 3-5 curriculum. It includes nine chapters, which introduce basic banking terms to young people, who are perhaps just beginning to learn about finances. Each issue builds upon the next and introduces two characters, Isabella and Noah, who try out different financial concepts along the way. Available at no-cost in English and Spanish language.
Other Youth Resources

Grades PreK-2 contains six lessons with hands-on, cross-curricular activities that engage preschool through second grade students. It explains financial concepts with age appropriate activities such as counting coins and defining needs and wants.
Full Grades PreK - 2 Curriculum
PreK - 2 Standard Alignment Chart
Due to the small screen size some information is no longer visible. Full information available when viewed on a larger screen.
Grades 3-5 contains eight lessons that expand on the lessons introduced in the PreK-2 curriculum. There are also newer topics such as how to create a budget and identifying ways to set goals for saving money.
Full Grades 3 - 5 Curriculum
Grades 3 - 5 Standard Alignment Chart
Grades 6-8 contains 12 lessons and is most appropriate for children ages 11 – 13. This curriculum contains important topics such as how to choose a successful career, and an introduction to understanding credit and debt.
Full Grades 6 - 8 Curriculum
Grades 6 - 8 Standard Alignment Chart
Grades 9-12 is our most expansive Money Smart for Young People curriculum. It contains 22 lessons that help prepare students for the real world by discussing topics such as car purchases, financing college and home ownership.
Grades 9 - 12 Standard Alignment Chart
Parent/ Caregiver Guides
The Money Smart Parent/ Caregiver Guides summarize key lesson concepts and exists as standalone resources. These guides also offer practical activities and conversation-starters on financial topics such as saving, setting financial goals, prioritizing spending decisions, and staying safe online.
Grades PreK-2
grade 6-8, grades 3-5, grades 9-12, digital toolkit.
The Digital toolkit consists of a few special activities from the MSYP Lesson plans that have been formatted for use on a computer or smart phone.
Digital toolkit PDF Fillable Forms
The Digital toolkit is available for immediate download (catalog.fdic.gov).
Money Smart for Young People Digital Toolkit
Coloring/ Activity Book
Money Smart for Elementary School Students introduces key personal finance concepts to children ages 5-8. This resource features a coloring/activity book for the students accompanied by a companion manual for use by anyone leading a discussion with a group of youngsters.
The Student Activity Book and Instructor Guide are available for immediate download (catalog.fdic.gov).
The Federal Deposit Insurance Corporation is prohibited from endorsing any specific organizations. Money Smart users must ensure that their publicity, advertisements, and public statements do not use the FDIC name or logo to imply that FDIC endorses their organization or its products or services.
Additional Links
This paper is in the following e-collection/theme issue:
Published on 24.4.2024 in Vol 26 (2024)
The Impact of Video-Based Microinterventions on Attitudes Toward Mental Health and Help Seeking in Youth: Web-Based Randomized Controlled Trial
Authors of this article:
Original Paper
- Diana Lemmer 1, 2 , MSc ;
- Markus Moessner 1 , PD, PhD ;
- Nicolas Arnaud 3 , PhD ;
- Harald Baumeister 4 , Prof Dr ;
- Agnes Mutter 4 , MSc ;
- Sarah-Lena Klemm 5 , BSc ;
- Elisa König 6 , Dipl-Psych ;
- Paul Plener 6, 7 , Prof Dr Med ;
- Christine Rummel-Kluge 5 , Prof Dr Med ;
- Rainer Thomasius 3 , Prof Dr Med ;
- Michael Kaess 8, 9 , Prof Dr Med ;
- Stephanie Bauer 1, 2, 10 , Prof Dr
1 Center for Psychotherapy Research, Center for Psychosocial Medicine, University Hospital Heidelberg, Heidelberg, Germany
2 Ruprecht-Karls University Heidelberg, Heidelberg, Germany
3 German Centre for Addiction Research in Childhood and Adolescence, University Medical Centre Hamburg-Eppendorf, Hamburg, Germany
4 Department of Clinical Psychology and Psychotherapy, Ulm University, Ulm, Germany
5 Department of Psychiatry and Psychotherapy, University of Leipzig Medical Center, Leipzig, Germany
6 Department of Child and Adolescent Psychiatry and Psychotherapy, University Hospital Ulm, Ulm, Germany
7 Department of Child and Adolescent Psychiatry, Medical University of Vienna, Vienna, Austria
8 University Hospital of Child and Adolescent Psychiatry and Psychotherapy, University of Bern, Bern, Switzerland
9 Clinic of Child and Adolescent Psychiatry, Center for Psychosocial Medicine, University Hospital Heidelberg, Heidelberg, Germany
10 German Center for Mental Health (DZPG), Partner site Mannheim/Heidelberg/Ulm, Heidelberg, Germany
Corresponding Author:
Stephanie Bauer, Prof Dr
Center for Psychotherapy Research
Center for Psychosocial Medicine
University Hospital Heidelberg
Bergheimer Str. 54
Heidelberg, 69115
Phone: 49 6221 56 7345
Fax:49 6221 56 7350
Email: [email protected]
Background: Mental health (MH) problems in youth are prevalent, burdening, and frequently persistent. Despite the existence of effective treatment, the uptake of professional help is low, particularly due to attitudinal barriers.
Objective: This study evaluated the effectiveness and acceptability of 2 video-based microinterventions aimed at reducing barriers to MH treatment and increasing the likelihood of seeking professional help in young people.
Methods: This study was entirely web based and open access. The interventions addressed 5 MH problems: generalized anxiety disorder, depression, bulimia, nonsuicidal self-injury, and problematic alcohol use. Intervention 1 aimed to destigmatize and improve MH literacy, whereas intervention 2 aimed to induce positive outcome expectancies regarding professional help seeking. Of the 2435 participants who commenced the study, a final sample of 1394 (57.25%) participants aged 14 to 29 years with complete data and sufficient durations of stay on the video pages were randomized in a fully automated manner to 1 of the 5 MH problems and 1 of 3 conditions (control, intervention 1, and intervention 2) in a permuted block design. After the presentation of a video vignette, no further videos were shown to the control group, whereas a second, short intervention video was presented to the intervention 1 and 2 groups. Intervention effects on self-reported potential professional help seeking (primary outcome), stigma, and attitudes toward help seeking were examined using analyses of covariance across and within the 5 MH problems. Furthermore, we assessed video acceptability.
Results: No significant group effects on potential professional help seeking were found in the total sample ( F 2,1385 =0.99; P =.37). However, the groups differed significantly with regard to stigma outcomes and the likelihood of seeking informal help ( F 2,1385 =3.75; P =.02). Furthermore, separate analyses indicated substantial differences in intervention effects among the 5 MH problems.
Conclusions: Interventions to promote help seeking for MH problems may require disorder-specific approaches. The study results can inform future research and public health campaigns addressing adolescents and young adults.
Trial Registration: German Clinical Trials Register DRKS00023110; https://drks.de/search/de/trial/DRKS00023110
Introduction
Mental health (MH) problems in youth are prevalent and pose severe health-related, social, and financial burdens on individuals [ 1 - 5 ] and societies [ 6 , 7 ]. Approximately half of all mental disorders first manifest before the age of 18 years [ 8 ], and MH problems in youth often persist and aggravate over the life span [ 9 - 14 ]. Therefore, the need for effective prevention and intervention programs targeting young people is an important public health goal. However, while effective MH services exist, most youth with MH problems do not seek professional help. Low uptake has been reported for various conventional [ 15 - 18 ] as well as digital MH services [ 19 - 22 ]. The burden of mental illness can only be alleviated at the population level if a substantial proportion of the population uses the available services [ 23 , 24 ]. Otherwise, the public health impact of MH services remains limited. Thus, increasing the reach of MH services (ie, fostering the uptake and use of professional help) is vital for the improvement of youth MH at the population level.
To facilitate service use, specific barriers to help seeking need to be addressed. Previous research has indicated that attitudinal factors pose larger impediments to help seeking than structural factors (eg, treatment costs and inconvenient scheduling) [ 25 , 26 ]. Specifically, self-reliance, a low perceived need for help [ 25 - 27 ], low treatment expectations [ 28 ], stigma [ 26 , 27 , 29 , 30 ], and poor MH literacy [ 27 , 31 , 32 ] have been identified as major contributors to the lack of professional help seeking.
Different approaches to facilitate help seeking and promote positive attitudes toward MH issues and help seeking in youth have been evaluated in previous research, including face-to-face and digital interventions. In a systematic mapping review, 84% (106/126) of the studies focused on school-based interventions, whereas only 10 (8%) articles covered internet-based approaches to improve MH literacy, MH-related attitudes, stigma, and help-seeking behavior in adolescents [ 33 ]. The internet-based interventions included both minimal, single-session interventions [ 34 , 35 ] and multisession approaches intended to be used over several weeks [ 36 , 37 ], with different outcome measures. A total of 4 studies focused on MH more broadly, whereas 6 studies investigated interventions for specific MH problems (depression: n=5; eating disorders: n=1). Keeping the limited number of studies in this area of research in mind, the results nevertheless point to the potential of internet-based interventions with respect to reduced stigma (2 studies), enhanced help-seeking intentions (2 studies), and improved help-seeking behaviors (1 study).
Clearly, there is a need for more research in this area, particularly with respect to digital brief and microinterventions (ie, highly focused in-the-moment interventions with a narrower scope and time frame than standard interventions [ 38 ]), which allow for a flexible, easily accessible, scalable, and efficient delivery of MH content. Initial research on such brief and microinterventions with psychoeducational and destigmatizing components has shown promising results. For instance, a brief acceptance-facilitating intervention that included a text-based personalized psychoeducation component had a small but significant effect on the intention to use MH services in German university students [ 39 ]. More recently, randomized controlled trials (RCTs) in young adults, university students, and adolescents with short video interventions demonstrated effects with regard to public stigma toward schizophrenia [ 40 , 41 ] and depression [ 42 , 43 ], as well as help-seeking intentions [ 42 ] and attitudes [ 43 ]. Furthermore, an Australian pilot study with international students found that a brief, web-based MH literacy intervention alleviated MH stigma. However, it had no significant effect on help-seeking intentions or MH literacy [ 44 ].
Another component of previous help seeking–facilitating strategies has been storytelling. A pilot study on a video-based intervention indicated that storytelling was well accepted and perceived as engaging [ 45 ]. In addition, an RCT evaluated internet-based storytelling programs with varying interactivity and stigma-related content. Significant reductions in MH stigma and microaggression toward individuals with MH problems were observed [ 46 ].
Concerning the theoretical foundation of interventions, few studies have investigated help seeking–promoting strategies that were explicitly based on the premises of health behavior models. Logsdon et al [ 47 ] evaluated an internet-based depression intervention for adolescent mothers, which was conceptualized according to the theory of planned behavior. The intervention led to significant improvements in help-seeking attitudes, intentions, and behavior. Another well-established and yet more recent health behavior model, which incorporates elements of previously developed approaches, is the Health Action Process Approach (HAPA) [ 48 ]. It encompasses a stage theoretical perspective on health behavior and includes a motivational, intention-forming phase as well as a volitional phase, where planning and behavior maintenance occur. In both the HAPA model and the updated version of the theory of planned behavior, namely, the reasoned action approach, outcome expectancies (or instrumental attitudes) play a crucial role in the formation of intentions, and intentions significantly predict actual behavior [ 49 , 50 ]. The results of previous research on a trauma recovery internet intervention support the use of the HAPA model for the prediction of e-MH engagement. Specifically, outcome expectations significantly predicted the intention to use the intervention (β=.36) [ 51 ]. Skepticism about treatment effectiveness has further been identified as a predictor for not using MH services in another study with university students [ 28 ].
Building on the findings of previous research, this study investigates the short-term effectiveness of 2 brief animated video interventions to promote potential professional help seeking in a general sample of adolescents and young adults aged 14 to 29 years using a web-based RCT approach. Both interventions aimed to improve participants’ willingness to seek professional help (ie, psychotherapists, psychiatrists, and counseling services) for 5 MH problems (generalized anxiety disorder [GAD], depression, bulimia, nonsuicidal self-injury [NSSI], and problematic alcohol use). The inclusion of various MH problems allowed for the investigation of potential differential effects. While one intervention followed a destigmatizing and psychoeducational approach, the other intervention aimed to induce positive outcome expectancies in accordance with the HAPA model through storytelling. The interventions were both compared to each other and to a nonintervention control group (CG) where participants were presented with a stand-alone video vignette without an additional intervention video. This approach was chosen due to both contextual (ie, vignette characters were described as experiencing difficulties in several life domains, and thus, additional control videos referring to the vignettes were unfeasible) and practical (ie, the creation of 10 additional videos was not necessary) considerations.
This study had the following objectives:
- To investigate the short-term effectiveness of the 2 interventions in the promotion of potential MH help seeking (professional and informal), whereby self-reported professional help seeking was defined as the primary outcome.
- To investigate the interventions’ effectiveness in the improvement of self-reported attitudes toward MH problems and MH service use (stigmatization and attitudes toward seeking MH services).
- To evaluate the interventions’ self-reported acceptability.
Within the framework of this study, the videos were evaluated as stand-alone interventions. They were not developed to replace existing interventions. However, in case of favorable outcomes, they have the potential to complement existing health care services. Results and procedures are reported in accordance with the Checklist for Reporting Results of Internet E-Surveys [ 52 ] and the CONSORT-EHEALTH (Consolidated Standards of Reporting Trials of Electronic and Mobile Health Applications and Online Telehealth) [ 53 ]. The study was preregistered at the German Clinical Trials Register on September 23, 2020 (DRKS00023110).
Study Design
This anonymous, fully automated, web-based, parallel-group exploratory RCT compared the effects of intervention 1 (psychoeducational intervention) and intervention 2 (positive consequences of help seeking) against those of the CG (no further videos after the case vignette) with regard to potential help seeking, attitudes toward help seeking, and stigma. The design comprised 15 conditions in total (5 MH problems × 3 interventional conditions). Randomization was stratified by gender and implemented using a permuted block design (block sizes: 15 and 30). Due to anonymous participation and automated randomization, researchers were unable to assign specific conditions to individuals. However, 2 of the authors were able to view the randomization list. The video material was aligned with the participants’ gender to increase identification with the character (ie, participants who identified as woman, female, or nonbinary viewed videos with a female protagonist [Paula], and participants identifying as man or male viewed videos with a male protagonist [Paul]). The study components and conditions as well as the study procedure are shown in Figure 1 .

Recruitment and Sample
Recruitment started in October 2020 and ended in May 2022. Youth aged between 14 and 29 years with sufficient German language skills were eligible for participation. The age of 14 years is widely accepted as appropriate to provide informed consent for medical decisions and participation in studies [ 54 , 55 ]. The upper age limit of 29 years aligns with the definition of emerging adulthood, a separate life stage between adolescence and adulthood [ 56 , 57 ]. Participants were primarily recruited through the web on social media platforms and via mailing lists, web-based marketplaces, and forums for adolescents and young adults (eg, accounts and emails of youth clubs and student associations). As an incentive to complete the study, participants were offered to take part in an optional gift card lottery at the end of the study (100 gift cards of €20 [US $21.58]). We asked participants for a valid email address if they were interested in the lottery and stored email addresses separately from other study data and user IDs to ensure anonymous participation.
We recorded page change time stamps. Participants whose time stamp data indicated that the video or the videos they were assigned to had not been fully viewed (ie, duration of stay<length of the respective videos) were excluded from statistical analyses. Furthermore, only data from participants who completed all questionnaires were included in the final analysis (n=1394; completion rate: 1394/2435, 57.25%). We also excluded 5 cases with duplicate user IDs, which occurred due to a technical error and indicated repeated participation ( Figure 1 ). HTTP cookies were used to assign individual user IDs to participants. For each session, new cookies were generated and used. Therefore, duplicate participation was possible after the completion of each study session and was not registered by the system. In the 5 aforementioned cases, duplicate IDs were mistakenly generated when participants tried to use the “back” button of their web browser and restarted their participation.
This study was conducted in an open access, voluntary web-based setting. A website was established to provide study information and enable participation. The ASMO software (Center for Psychotherapy Research) [ 58 ] was used to implement the RCT. A randomization list with numbers representing the conditions was generated and embedded in our ASMO database [ 58 ] before recruitment. Data were collected at the Center for Psychotherapy Research, Heidelberg. The study’s technical functionality and usability were extensively tested before recruitment by the authors and their colleagues at their respective institutions. Before their participation, the youth received detailed information about the aims, scope, procedures, data processing, and data storage of the study on the website. Participants were informed that they would be randomly assigned to 1 of 5 MH problems and 1 of 3 video versions. They were not informed about the specific health issues or the conditions’ details before participation. As the aim of the conditions was to provide information about a specific MH problem, blinding of participants after assignment to the interventions was not possible. Only participants who provided informed consent through a web-based checkbox were eligible for participation. After study completion, participants were debriefed in writing about the objectives on the study website. The debriefing form also included contact information for formal help services. Study duration amounted to approximately 30 minutes. Participants were first asked to complete sociodemographic and screening questionnaires; were then randomly assigned to 1 of the 15 experimental conditions; and, finally, were presented with the outcome questionnaires. The whole study (including informed consent and gift card lottery pages) comprised 26 pages with 1 to 12 items on each page. Each segment or measure was presented on 1 or 2 separate pages depending on its respective length. Some items were conditional for adaptive questioning (eg, when lifetime NSSI was denied, no further questions about NSSI were presented). Changes to the item responses could only be made while they had not been confirmed through a click on the “next” button, which brought participants to the next page. There was no “back” button.
Sociodemographics and Screening
All measures were self-reported. The sociodemographic form asked participants about their age, gender, migration background, education, whether they knew someone with MH problems, and participants’ previous or current MH service use (actual help seeking). Thereafter, participants’ subjective psychological distress was assessed using several screening instruments.
Anxiety symptoms were measured using the 7-item Generalized Anxiety Disorder Scale (GAD-7) [ 59 ]. Symptom frequency within the previous 2 weeks was indicated on a 4-point response scale. Total scores (potential range 0-21) were used for further analyses. Scores of ≥5 indicate a mild anxiety symptomatology, scores of ≥10 indicate a moderate anxiety symptomatology, and scores of ≥15 indicate a severe anxiety symptomatology [ 59 ].
The 9-item Patient Health Questionnaire (PHQ-9) [ 60 ] was used for depression symptomatology assessment. Frequencies of depression symptoms within the previous 2 weeks were measured on a 4-point scale. Total scores (potential range 0-27) were calculated for further analyses. Total scores of ≥5 were interpreted as mild, scores of ≥10 were interpreted as moderate, scores of ≥15 were interpreted as moderately severe, and scores of ≥20 were interpreted as severe depression symptomatology [ 60 ].
The Weight Concerns Scale (WCS) [ 61 , 62 ] assessed weight and body shape concerns. It consists of 5 items with varying response scale types (4- to 7-point scales). The response categories of each item represent scores between 0 and 100. The mean across all items was used for further analyses. Scores of ≥57 are indicative of a high risk of eating disorders [ 61 ].
Problematic alcohol use during the previous 12 months was measured using the Alcohol Use Disorders Identification Test for Consumption (AUDIT-C) [ 63 , 64 ]. It comprises 3 items with 5-point response scales. Sum scores range between 0 and 12. A score of 0 indicates abstinence, whereas scores between 1 and 3 are interpreted as moderate alcohol consumption. Scores of ≥4 indicate hazardous alcohol consumption [ 63 , 65 ].
A total of 4 items of the Self-Injurious Thoughts and Behaviors Interview [ 66 ] served to assess NSSI. The first item identified whether participants had ever harmed themselves without suicidal intention. If participants reported lifetime NSSI, the 3 subsequent questions were presented. These items measured the frequency of NSSI within the last year, the age at the first occurrence of NSSI, and the age at the last occurrence of NSSI. Item responses were analyzed separately and descriptively.
Experimental Conditions and Materials
The interventional strategies were applied using short animated videos. The videos were created with the Pro+ version of the web-based animation tool Powtoon (Powtoon Limited) [ 67 ]. Each research group involved in this study prepared materials for 1 of the 5 MH problems based on their respective field of expertise. The materials were structured in a similar fashion across MH problems. The main characters, Paul and Paula, were introduced as students aged 16 years in each condition. In total, 30 videos were created: 5 MH problems × 2 main character genders × 3 video types. Participants in the control condition only viewed a vignette, whereas participants in both intervention groups each viewed 1 additional video (either for intervention 1 or intervention 2). A subset of the videos was pretested between July 2020 and September 2020 with a convenience sample of 9 youths (mean age 18.56, SD 3.74 years; range 14-24 years; 3/9, 33% male), who confirmed comprehensibility and overall acceptability.
All participants viewed a case vignette. Each vignette depicted the respective main character, who was affected by 1 of 5 MH problems (GAD, depression, bulimia, NSSI, or problematic alcohol use). The vignettes introduced the characters to the viewers in a third-person perspective and described their challenges in their everyday lives due to their MH conditions (eg, difficult emotions and cognitions, physical symptoms, and social and school-related issues). The accurate diagnostic labels were not presented in the vignettes [ 68 ]. Vignette duration ranged from 2 minutes, 19 seconds to 2 minutes, 47 seconds (mean 2 min, 29 s; SD 11 s). The bulimia vignettes were developed first. They were inspired by the vignettes by Mond et al [ 69 ] and adapted in accordance with International Classification of Diseases, 10th Revision and Diagnostic and Statistical Manual of Mental Disorders, 5th Edition diagnostic criteria, as well as further literature on the symptomatology and psychological strain of bulimia [ 70 ]. The bulimia vignettes then served as a template for the vignettes of the other 4 MH problems.
Intervention 1
Intervention 1 aimed to improve MH literacy and decrease stigmatization through the presentation of psychoeducational information to encourage help seeking. These intervention videos first presented the correct diagnostic label, prevalence rates, and core symptoms of the condition shown in the vignette. Next, 5 destigmatizing and psychoeducational facts about the respective condition were presented (eg, “Bulimia is a serious illness and not a lifestyle”), which were inspired by the work by Bulik [ 71 ]. The videos then presented treatment options, information about potential challenges in professional help seeking, and encouraging statements about the benefits of professional MH support. Intervention 1 video durations ranged from 4 to 5 minutes (mean 4 min, 27 s; SD 21 s). The information provided in these intervention videos was based on epidemiological, etiological, diagnostic, barrier-related, and interventional findings on the respective MH problems (eg, the studies by Bulik [ 71 ], Keski-Rahkonen and Mustelin [ 72 ], and Nagl et al [ 73 ] for bulimia).
Intervention 2
The second strategy (intervention 2) was based on the premises of the HAPA [ 48 ]. Intervention 2 was designed to induce positive outcome expectancies of professional help seeking through the continuation of Paul and Paula’s stories. The videos showed the main characters 1 year after their initial situation as described in the vignettes. Intervention 2 videos first demonstrated the help-seeking process of the main characters in a retrospective fashion. Encouraged by their teachers, friends, or parents, the main characters sought and received professional support from a psychotherapist. The psychotherapist’s gender matched the gender of the main character. The videos showed how the psychotherapist informed the main character about the correct diagnostic label of their condition and shortly portrayed the therapeutic process. The process included initial difficulties of the main character, such as feelings of insecurity about disclosing their experiences to their therapist, which were resolved over time, and the main characters became invested in their psychotherapy. Then, 5 positive consequences of psychotherapy were presented, such as decreased impairment and an improved quality of life. The videos ended with the notion that the main character was still facing occasional difficulties, but substantial improvements in overall well-being and satisfaction with their decision to seek help were emphasized. Intervention 2 video durations ranged from 4 minutes, 1 second to 4 minutes, 29 seconds (mean 4 min, 15 s; SD 14 s). These interventions were designed in accordance with previous literature on the therapeutic process in MH conditions, including treatment expectations, experiences, and consequences [ 74 ].
Outcome Measures
Primary outcome measure.
Our primary outcome was the potential use of professional MH services (ie, the hypothetical likelihood of seeking formal sources of help if participants experienced Paul’s or Paula’s MH problem), measured using a 12-item version of the General Help Seeking Questionnaire (GHSQ) [ 75 ]. The GHSQ measures the willingness of seeking various formal and informal sources of help within the next 4 weeks for an indicated MH problem on a 7-point rating scale (1=“extremely unlikely”; 7=“extremely likely”). The maximum score among the 3 items, which measured potential help seeking with professional MH services (psychotherapists, psychiatrists, and counseling services), was used as our primary outcome. The GHSQ is the most frequently used instrument for help seeking [ 76 ].
Secondary Outcome Measures
GHSQ data on the potential use of informal sources (romantic partner, friend, parent, or other family member) and no intended help seeking (1 item) were used as secondary outcomes. For informal sources of support, the items’ maximum score was used for the analyses.
Attitudes toward help seeking were measured using the Inventory of Attitudes Toward Seeking Mental Health Services (IASMHS) [ 77 ] on a 5-point rating scale. It comprises 24 items. Its 3 dimensions—“psychological openness,” “help-seeking propensity,” and “indifference to stigma”—are represented with 8 items. Subscale scores range from 0 to 32. Higher scores indicate more positive attitudes.
The Universal Stigma Scale (USS) [ 78 ] was used for stigma measurement. It consists of 11 statements in 2 subscales (“blame/personal responsibility”: 5 items; “impairment/distrust”: 6 items). The extent of agreement with these statements is indicated on a 5-point Likert scale. Means were calculated for each of the 2 subscales. Lower scores indicate higher stigmatization.
Transportation (ie, the immersiveness of the stories presented in the videos) was measured using an adapted version of the Transportation Scale–Short Form [ 79 ]. Adjustments were made to suit the medium of the narratives (ie, video material in contrast to written stories). Our adapted version contained 5 items on a 7-point Likert scale.
Video acceptability was measured using a translated and adapted 4-item version of the acceptability and likability scale used by Gaudiano et al [ 45 ]. In total, 3 items measured overall likability, comprehensibility, and interestingness of the videos on a 5-point rating scale.
Statistical Analysis
Sociodemographic, screening, and outcome data were first analyzed descriptively. Intervention effects on potential professional help seeking (primary outcome) and secondary outcomes in the total sample (ie, across all MH problems and across participants with and without actual help seeking as reported in the screening) were analyzed via analyses of covariance (ANCOVAs) at an α level of P <.05. In addition to the intervention group, the models included age as a covariate, the participants’ actual help seeking (fixed effects), and the 5 MH problems (random effects) as control variables. The results of the main ANCOVA in the total sample are presented in the Results section.
Subgroup ANCOVAs were conducted for each of the 5 MH problems separately. In this case, the respective screening scores (GAD-7, PHQ-9, WCS, number of NSSI events during the last year, and AUDIT-C) were included as additional covariates. Subgroup analyses were further conducted for cases with and without actual help seeking in the total sample and within each of the 5 MH issue groups.
In case of significant ( P <.05) and trend ANCOVA effects, pairwise group comparisons were conducted using 2-tailed t tests. All tests were 2-sided with an α level of 5%. Mean differences (MDs) adjusted for covariates are reported in the Results section.
An a priori power analysis was conducted using G*Power (Heinrich-Heine-Universität Düsseldorf) [ 80 ]. Under the assumption of a medium effect size ( f =0.25), a minimum of 240 participants (80 per condition) were needed to test the expected effect within each of the 5 MH problems via ANCOVAs with a significance criterion of α=.05 and a power of 90%. Statistical analyses were performed using R (version 4.3; R Foundation for Statistical Computing) [ 81 ] and SPSS (version 28; IBM Corp) [ 82 ]. R was also used to generate the random allocation sequence. Authors involved in data analysis and interpretation were not blinded with respect to the assigned experimental conditions.
Deviations From the Protocol
In the beginning of recruitment, the upper age limit was raised from 25 years originally to 29 years due to the aforementioned findings of previous research.
Ethical Considerations
Ethics approval was obtained from Ethics Committee I of the Heidelberg Medical Faculty on July 27, 2020 (protocol S378/2020). The procedures were in accordance with the Helsinki Declaration of 1975, as revised in 2000. All participants received information about the study’s aims, scope, procedures, data processing, and data storage on the study website in written form. Furthermore, all participants received contact information if they wished to clarify questions via telephone or email. Only participants who provided their informed consent through a web-based checkbox were eligible for participation. Participants were able to opt out of the study at any time by closing the study website, which they were informed of before their participation. Participants were offered to take part in an optional gift card lottery at the end of the study (100 gift cards of €20 [US $21.58] each). If they were interested in the lottery, they could enter their email address. Email addresses were stored separately from other study data and user IDs to ensure anonymity. All other data were collected and are reported anonymously. Thus, this study does not contain any individual data of identifiable participants.
Sample Characteristics
Figure 1 shows the flow of participants. Of the 2208 participants who were randomized to 1 of the 15 conditions, 472 (21.38%) were excluded because their time spent on the video pages fell below the durations of the videos they were assigned to, indicating that they did not view the entire videos. Of the remaining 1736 participants, 342 (19.7%) were excluded due to incomplete data (ie, they did not complete all the relevant scales that the study entailed [beginning with informed consent up to and including the last acceptability item]). Our final sample consisted of 1394 youths aged 14 to 29 years (mean 20.97, SD 3.67 years). Sociodemographic and screening results are shown in Table 1 .
a MH: mental health.
b GAD-7: 7-item Generalized Anxiety Disorder Scale.
c PHQ-9: 9-item Patient Health Questionnaire.
d WCS: Weight Concerns Scale.
e SITBI-G: German version of the Self-Injurious Thoughts and Behaviors Interview.
f NSSI: nonsuicidal self-injury.
g We excluded 4 cases in “Age of last NSSI – age of first NSSI” due to invalid values (age of first NSSI>age of last NSSI).
h AUDIT-C: Alcohol Use Disorders Identification Test for Consumption.
A total of 79.56% (1109/1394) of the sample identified as woman or girl, and 44.76% (624/1394) were help seekers (ie, they used professional MH services at the time of or before data collection). On average, the youth were moderately anxious (mean GAD-7 score 8.38, SD 5.00) and depressed (mean PHQ-9 score 9.56, SD 6.07). While 22.88% (319/1394) reported abstinence in the AUDIT-C, 30.85% (430/1394) indicated hazardous alcohol consumption. A total of 19.58% (273/1394) were at high risk of developing an eating disorder according to the WCS. One-third (479/1394, 34.36%) of the sample reported a lifetime history of NSSI according to the Self-Injurious Thoughts and Behaviors Interview, with a 12-month prevalence rate of 19.01% (265/1394).
Intervention Effects
The main results are presented in Table 2 .
a Results controlled for help seeking (fixed factor), mental health issue (random factor), and age (covariate).
b CG: control group.
c GHSQ: General Help Seeking Questionnaire.
d Higher scores represent a greater level of agreement.
e Pairwise comparisons were conducted in case of significant or trend analysis of covariance effects. Empty cells indicate that pairwise comparisons were not conducted due to the analysis of covariance results.
f USS: Universal Stigma Scale.
g Higher scores represent more positive attitudes toward mental health issues and help seeking.
h IASMHS: Inventory of Attitudes Toward Seeking Mental Health Services.
i TS-SF: Transportation Scale–Short Form.
Figure 2 summarizes the results of the overall efficacy and the MH issue–specific subgroup analyses graphically. Specific results of the subgroup analyses can be found in Multimedia Appendices 1 , 2 , and 3 .

Primary Outcome: Potential Professional Help Seeking (GHSQ)
On the 7-point scale of the GHSQ, most participants (1046/1394, 75.04%) selected a score of ≥4 (CG: 409/554, 73.8%; intervention 1: 316/410, 77.1%; intervention 2: 321/430, 74.7%). In total, 19.23% (268/1394; CG: 105/554, 19%; intervention 1: 74/410, 18%; intervention 2: 89/430, 20.7%) of participants reported a score of 7 (“extremely likely”), whereas 6.74% (94/1394; CG: 47/554, 8.5%; intervention 1: 24/410, 5.9%; intervention 2: 23/430, 5.3%) responded with a score of 1 (“extremely unlikely”). Across all MH problems, no statistically significant group main effect was found on potential professional help seeking ( F 2,1385 =0.99; P =.37; Table 2 ).
Secondary Outcomes
Potential informal help seeking (ghsq).
For informal sources of support, most participants (1190/1394, 85.37%) selected a score of ≥5 on the 7-point scale (CG: 478/554, 86.3%; intervention 1: 338/410, 82.4%; intervention 2: 374/430, 87%). For 43.69% (609/1394) of the participants, informal help seeking was “extremely likely,” with a selected score of 7 (CG: 244/554, 44%; intervention 1: 161/410, 39.3%; intervention 2: 204/430, 47.4%), whereas a minority of 1% (14/1394; CG: 4/554, 0.7%; intervention 1: 7/410, 1.7%; intervention 2: 3/430, 0.7%) responded with a score of 1 (“extremely unlikely”). In the total sample, significant group differences were found regarding informal help seeking ( F 2,1385 =3.75; P =.02), with intervention 2 showing a significantly higher mean score than intervention 1 (adjusted MD=0.25; P =.007; Table 2 ). In the subsample of help seekers across MH problems, the same pattern was observed ( F 2,616 =3.21; P =.04; adjusted MD=0.37; P =.01; Multimedia Appendix 1 ). A significant group effect was also found for the total sample in the problematic alcohol use conditions ( F 2,273 =3.51; P =.03; Multimedia Appendix 2 ). Both the CG (adjusted MD=0.42; P =.02) and intervention 2 (adjusted MD=0.41; P =.03) had greater mean scores than intervention 1.
No Potential Help Seeking (GHSQ)
With regard to no intention of seeking help with any of the potential sources listed in the GHSQ (“I would not seek help from anyone” item), almost half (674/1394, 48.35%) of participants selected a score of 1 or 2 (1=“extremely unlikely”; CG: 264/554, 47.7%; intervention 1: 185/410, 45.1%; intervention 2: 225/430, 52.3%), whereas 15.42% (215/1394) responded with a score of 6 or 7 (7=“extremely likely”; CG: 89/554, 16.1%; intervention 1: 68/410, 16.6%; intervention 2: 58/430, 13.5%). There were no statistically significant group differences in the total sample ( P =.07; Table 2 ). However, there were trends for group differences in some of the MH issue subgroups ( Multimedia Appendices 2 and 3 and Figure 2 ).
Public Stigma: Blame and Personal Responsibility (USS)
With regard to the USS blame and personal responsibility subscale, statistically significant group differences were found in the total sample ( F 2,1385 =3.25; P =.04; Table 2 ) and in non–help seekers across MH problems ( F 2,762 =3.21; P =.04; Multimedia Appendix 1 ). In the total sample, both intervention 1 and intervention 2 had significantly greater means compared to the CG (intervention 1>CG: adjusted MD=0.084 and P =.03; intervention 2>CG: adjusted MD=0.085 and P =.03). In the subgroup of non–help seekers, there was a significant difference between intervention 2 and the CG (adjusted MD=0.13; P =.02). Further subgroup analyses revealed no additional differences between experimental conditions. It should be noted that blame and personal responsibility data distributions were heavily skewed to the left (total sample: skew=−1.58). As logarithmic, natural logarithm, square root, and reciprocal transformations did not normalize the distributions, we decided to perform ANCOVAs using the untransformed blame data. Therefore, results should be interpreted with caution.
Public Stigma: Impairment and Distrust (USS)
For the USS distrust subscale, ANCOVAs revealed statistically significant group differences in the total sample ( F 2,1385 =8.01; P <.001; Table 2 ) in both help seekers ( F 2,616 =4.39; P =.01) and non–help-seekers across MH problems ( F 2,762 =3.74; P =.02; Multimedia Appendix 1 ). Moreover, statistically significant group differences were found in the total problematic alcohol use subsample ( F 2,273 =4.49; P =.01; Multimedia Appendix 2 ) and its subgroup of non–help seekers ( F 2,144 =4.00; P =.02; Multimedia Appendix 3 ). In the NSSI subgroup of non–help seekers, a significant group main effect was observed ( F 2,160 =4.50; P =.01; Multimedia Appendix 3 ). Across MH problems, both in the total sample (intervention 1>CG: adjusted MD=0.13 and P =.005; intervention 2>CG: adjusted MD=0.17 and P <.001) and the subsample of help seekers (intervention 1>CG: adjusted MD=0.16 and P =.02; intervention 2>CG: adjusted MD=0.17 and P =.01), significantly larger means in both interventions as compared to the CG were observed. Among participants without previous help seeking across MH problems, post hoc comparisons only revealed a statistically significant difference between intervention 2 and the CG (adjusted MD=0.16; P =.007). In the NSSI subgroup of non–help seekers, intervention 2 differed significantly from both the CG (adjusted MD=0.36; P =.005) and intervention 1 (adjusted MD=0.31; P =.02). For problematic alcohol use, in both the total sample and the subsample of non–help seekers, significant post hoc differences between intervention 2 and the CG (MD for the total=0.32 and P =.003; MD for those without previous help seeking=0.42 and P =.006) were found.
Psychological Openness (IASMHS)
No statistically significant group main effect on the IASMHS psychological openness subscale was found in the total sample ( Table 2 ). Significant effects were found in the total depression sample ( F 2,255 =4.59; P =.01; Multimedia Appendix 2 ) and its subgroup of non–help seekers ( F 2,138 =4.20; P =.02; Multimedia Appendix 3 ). In the total depression sample, intervention 1 showed a greater mean in comparison to the CG (adjusted MD=1.38; P =.046) and intervention 2 (adjusted MD=2.24; P =.003). In the subsample of non–help seekers in the depression conditions, intervention 1 was found to have a greater mean than intervention 2 (adjusted MD=2.75; P =.004), but no significant difference was found with the CG (adjusted MD=1.55; P =.09). No significant group main effects were observed in the other subsamples.
Help Seeking Propensity (IASMHS)
In the total sample, no significant group main effect was found for the IASMHS help seeking propensity subscale ( Table 2 ). Subgroup analyses revealed significant differences in the total bulimia sample ( F 2,271 =3.27; P =.04), where both intervention 1 (adjusted MD=1.51; P =.03) and intervention 2 (adjusted MD=1.40; P =.04) showed larger means than the CG ( Multimedia Appendix 2 ). No further group differences were found in the other subsamples.
Indifference to Stigma (IASMHS)
For the IASMHS indifference to stigma subscale, differential group main effects were found in the total sample ( F 2,1385 =3.18; P =.04; Table 2 ), in the subsample of non–help seekers ( F 2,762 =3.74; P =.02; Multimedia Appendix 1 ), in the total ( F 2,288 =3.22; P =.04; Multimedia Appendix 2 ) and non–help-seeking ( F 2,176 =4.48; P =.01; Multimedia Appendix 3 ) GAD samples, in the total bulimia sample ( F 2,271 =3.45; P =.03; Multimedia Appendix 2 ), and in the NSSI subsample of non–help seekers ( F 2,160 =3.23; P =.04; Multimedia Appendix 3 ). Across MH problems, the CG showed a larger mean than intervention 1 in the total sample (adjusted MD=0.97; P =.02), whereas a greater mean score in the CG compared to those of both intervention 1 (adjusted MD=1.20; P= .02) and intervention 2 (adjusted MD=1.15; P =.02) was found in the subsample without previous help seeking. A similar pattern emerged in the total GAD sample and its subsample of non–help seekers, where the CG’s means were significantly larger in comparison to those of intervention 1 (adjusted MD=2.09; P =.02) in the total sample and of both intervention 1 (adjusted MD=2.57; P =.02) and intervention 2 (adjusted MD=2.91; P =.008) among non–help seekers. In the total bulimia sample, intervention 1 had a significantly higher mean than intervention 2 (adjusted MD=2.26; P =.009), whereas both the CG (adjusted MD=2.10; P =.04) and intervention 2 had greater means than intervention 1 (adjusted MD=2.59; P= .02) in the NSSI subsample of non–help seekers.
Video Acceptability and Transportation
In the total sample, most participants (1041/1394, 74.68%) rated the videos with a score of “4” (705/1394, 50.57%) or “5” (336/1394, 24.1%) on the overall likability item. Regarding comprehensibility, 83.93% (1170/1394) rated the videos as “very comprehensible” (“5” on the 5-point scale), whereas 14.13% (197/1394) assigned them a score of “4.” With respect to the videos’ interestingness, the responses were distributed across the 5-point scale as follows: 27.4% (382/1394) of participants gave a rating of “5,” a total of 41.61% (580/1394) gave the videos a rating of “4,” a total of 22.02% (307/1394) assigned them a score of “3,” and 7.32% (102/1394) gave them a rating of “2.” A minority of participants (23/1394, 1.65%) rated the videos with a score of “1” on the interestingness scale.
In the total sample ( Table 2 ), the intervention 1 videos were rated as generally more likable ( F 2,1385 =12.20; P <.001; intervention 1>CG: adjusted MD=0.25 and P <.001; intervention 1>intervention 2: adjusted MD=0.20 and P <.001) and interesting ( F 2,1385 =6.39; P =.002; intervention 1>CG: adjusted MD=0.06 and P =.02; intervention 1>intervention 2: adjusted MD=0.07 and P <.001) in comparison to those of the CG and intervention 2. The groups did not differ significantly in video comprehensibility ( F 2,1385 =2.01; P =.13). Participants felt more “transported” into the videos’ narratives in the CG and intervention 1 as compared to participants in intervention 2 ( F 2,1385 =4.23; P =.02; CG>intervention 2: adjusted MD=0.17 and P =.03; intervention 1>intervention 2: adjusted MD=0.23 and P =.006; Table 2 ). Most subgroup analyses revealed either similar patterns with regard to general likability and interestingness (eg, total help seekers, total GAD sample, and GAD non–help seekers) or no significant differences (eg, GAD help seekers, bulimia help seekers, all depression samples, and all alcohol use samples; Multimedia Appendices 1 - 3 ). In the cases of bulimia (total and non–help-seeking subsamples; Multimedia Appendices 2 and 3 ) and NSSI ( Multimedia Appendix 2 ), different patterns emerged. In the total bulimia sample, the videos of both the CG and intervention 1 scored significantly higher on the interestingness scale than those of intervention 2 ( F 2,271 =4.49; P =.01; CG>intervention 2: adjusted MD=0.33 and P =.02; intervention 1>intervention 2: adjusted MD=0.44 and P =.005). In the total NSSI sample, the videos of both intervention 1 and intervention 2 were rated as significantly more likable than those of the CG ( F 2,277 =10.31; P <.001; intervention 1>CG: adjusted MD=0.51 and P <.001; intervention 2>CG: adjusted MD=0.29 and P =.008).
Principal Findings
This study developed and tested the short-term effectiveness of 2 brief video-based strategies targeted at adolescents and young adults (aged 14 to 29 years) aiming to foster potential professional help seeking (main outcome) and related attitudes for 5 MH problems. In the total sample, we did not find effects of either intervention 1 (psychoeducation) or intervention 2 (positive outcome expectancies) on our primary outcome. However, significant group effects were found with respect to potential informal help seeking, stigma toward others, and indifference to stigma in the total sample. While both intervention groups showed more favorable attitudes than the CG with regard to public stigma, this did not translate to participants’ own indifference to stigma. In this case, the CG showed significantly more positive attitudes in comparison to intervention 1. However, this finding was not apparent in the MH issue–specific subgroup analysis with the exception of GAD. Unintended adverse effects of MH interventions have been reported in previous research [ 83 - 85 ], which underlines the need for thorough evaluations of such interventions before their public dissemination. Accordingly, we would advise against the implementation of our GAD interventions at the current stage and would recommend the development and evaluation of other tailored strategies for this MH problem.
With regard to informal help, participants in intervention 2 showed a greater willingness to approach friends, family members, or romantic partners for help than participants in intervention 1. This might have been due to the interventions’ design as intervention 2 explicitly depicted improvements in social relationships after the main characters in the videos had sought professional support. Overall, the videos were well accepted and rated as quite interesting, with some room for improvement and with the videos of intervention 1 outperforming those of the other 2 conditions. All videos were, on average, rated as very comprehensible, and no significant group differences were observed in this regard. Interestingly, participants felt more transported into the narratives in the CG and intervention 1 as compared to those in intervention 2. As intervention 2 followed a narrative approach, continuing Paul and Paula’s vignette stories, this was surprising. However, as previously stated, intervention 1 was generally more liked and viewed as more interesting in comparison to intervention 2. The animated and fictional third-person approach of intervention 2 seemed to not have sparked as much interest in participants as the facts presented in intervention 1. While we aimed to increase identification with our main characters through the alignment of their genders with those of the participants, intervention 2 might have been insufficient with regard to the perceived “realness” of the story and the characters, which has been identified as crucial for the formation of narrative transportation and, in turn, attitudes and intentions [ 86 ]. The rather optimistic portrayal of the help-seeking process might have contributed to a lack of perceived authenticity in this sample as well. Furthermore, implicit MH statements in the videos’ scenarios could have been more fruitful. For instance, the viewer could have watched directly how Paul and Paula discussed their issues with a psychotherapist rather than having a narrator describe the situation to them. These types of videos have been associated with improved health literacy and more beneficial attitudes toward cervical cancer [ 87 ], and their application to the field of MH would be interesting.
We further observed differential outcomes with respect to the assigned MH problems and participants’ actual help-seeking status. While the CG outperformed either intervention 1 (total) or both interventions (subgroup of non–help seekers) for GAD with regard to stigma indifference and no further outcomes were found for GAD, different patterns emerged in the other MH issue groups. Results were mixed, where both intervention 1 and intervention 2 outperformed the other conditions in some of the outcomes but not in others (eg, in depression), or a clearer tendency toward the superiority of one of the interventions emerged (eg, in NSSI). In summary, our results point toward the usefulness of tailored interventions with regard to MH issue type and previous help-seeking experiences of potential target groups. Our finding that different strategies might work differently for each of the 5 MH problems included in our study is in accordance with those of previous research. For example, Ebneter and Latner [ 78 ] found varying stigmatizing attitudes among different MH problems. The participants in their study blamed a vignette character with an eating disorder more for their condition than a character with depression, whereas the latter was regarded as more impaired. Our finding that a destigmatizing and psychoeducational intervention such as intervention 1 might work better for bulimia fits their recommendation to target stigmatizing attitudes toward specific MH problems [ 78 ]. Similarly, alcohol dependency and self-endangering behaviors were perceived as particularly dangerous in a Swiss vignette study [ 88 ]. The humanizing depiction of our NSSI and problematic alcohol use characters within a framework of close supportive relationships, which improved in quality through psychotherapy, might have been a relevant factor for reduced distrust scores in the intervention 2 condition as compared to the CG and in the case of non–help seekers in the NSSI condition as compared to intervention 1 as well. This approach might be advantageous to reduce public stigma regarding MH problems that are viewed as particularly dangerous. Decisions for one or another interventional strategy may also depend on the specific goal and targeted outcome. While more research is needed, our study provides preliminary evidence for the tailored strategies suggested in Table 3 .
a Check marks (✓) represent recommended use of an intervention; crosses (X) represent advice against the use of an intervention; and question marks (?) represent inconclusive results and, therefore, no clear recommendation. Recommendations are solely based on the results of this study.
b GAD: generalized anxiety disorder.
c No recommended use.
d NSSI: nonsuicidal self-injury.
Limitations
One limitation of this study lies within the sole investigation of effects on hypothetical intentions and attitudes instead of actual help-seeking behavior. While intentions are substantially associated with behavior and provide valuable insights, they do not translate directly to behavior change [ 49 ]. Moreover, only short-term effects were investigated. Previous studies on short video-based interventions have demonstrated sustaining destigmatizing effects for 1 [ 40 ] and 5 months after their delivery [ 43 ]. While potential long-term effects of our interventions in particular remain unknown and might be investigated in the future, the current state of research points toward potentially impactful long-term effects of low-threshold microinterventions. Related to this, we did not investigate dose-response effects. Research on optimal doses (ie, durations, frequencies, and amounts of intervention components) needed for sustainable change through microinterventions and interventions in general is crucial for well-founded recommendations for or against specific interventions [ 89 ].
Just as in other microintervention studies among youth [ 39 ], group differences in our study were small. However, the potential high reach of easily accessible, low-threshold interventions such as the ones evaluated in this study is apparent in the final sample size of 1394. As it depends on both effectiveness and reach, this allows for a comparably high public health impact [ 23 , 24 ]. We also included trend effects in our overview ( Figure 2 ), which should be interpreted with caution. However, these findings might be useful to inform the planning of subsequent research in this field.
Future research should focus on improvements in the effectiveness of microinterventions. One approach could be the investigation of interventional framing. In a Japanese study on depression, loss-framed messages (ie, emphasizing negative consequences of refraining from help seeking) had a greater impact on help-seeking intentions than gain-framed (positive consequences of help seeking) or neutral (eg, prevalence rates) messages as well as unformatted, plain-text messages in middle-aged adults [ 90 ]. Thus, it might be interesting to conduct future studies on the effects of video-based microinterventions with differently framed messaging as the videos in this study emphasized potential gains of help seeking rather than potential losses of help seeking restraint.
Furthermore, our sample showed, on average, a high level of education, very little public stigma, a pronounced willingness to seek help, and a high rate of actual professional help seeking (624/1394, 44.76%), which limits the generalizability of our findings. More than 90% (1285/1394, 92.18%) of our sample knew someone with MH problems. While we were careful not to recruit MH experts, such as university students of medicine and psychology, youth with a personal interest in MH-related topics seemed to have been more inclined to participate. Related to this, we aimed for a community youth sample rather than a clinical sample. The scenarios that our items referred to were hypothetical and did not necessarily reflect participants’ own experiences due to the random assignment to 1 of the 5 MH problems. A similar approach with targeted interventions according to youth’s actual MH status and more individualized elements with regard to gender-related [ 91 ] and cultural [ 92 , 93 ] aspects could be promising in future research. Thus, upcoming studies should strive to align their research objectives more closely with the characteristics and needs of the selected target groups.
Finally, we did not include a comprehension check to assess participants’ understanding of and engagement with the content presented in the videos. While we accounted for the time participants spent on the video pages and only included participants with sufficient durations of stay in the final analyses, they may not have fully comprehended or attended to the video material. The substantial number of excluded participants who completed the study without meeting the time threshold (472/2208, 21.38%) underlines this potential issue. Thus, future studies should address this limitation by including comprehension checks to improve the robustness of the findings.
Conclusions
The low uptake of professional MH services in youth reflects the need for appropriate strategies to facilitate professional help seeking. This study investigated the effectiveness of 2 short video-based strategies targeted at youth (aged 14 to 29 years) on potential professional help seeking and related attitudes for 5 MH problems. While we did not find intervention effects on potential professional help seeking (with the exception of previous help seekers in the depression conditions), differential intervention effects depending on each MH problem and participants’ actual help-seeking status were found in our secondary outcomes, such as public stigma. Our study results can be used to inform the development of new antistigma interventions, which, based on our results, we would recommend tailoring to specific MH problems, target groups, and outcomes. While group differences were small, such low-threshold interventions can be easily disseminated and, therefore, hold potential for a high reach and, thus, a meaningful impact at the population level. More research is needed for more robust and generalizable recommendations.
Acknowledgments
This study was funded by the German Federal Ministry of Education and Research (funding identifier: 01GL1904). The Federal Ministry of Education and Research had no influence on the design of the study and was not involved in data collection, analysis, and interpretation or the writing of the manuscript. For the publication fee, the authors acknowledge financial support from Heidelberg University. The authors thank Sabrina Baldofski, Elisabeth Kohls, Felicitas Mayr, and Maria I. Austermann for their support in the creation of video materials for this study (depression and alcohol abuse videos). The authors thank Lutfi Arikan (University Hospital Heidelberg) for enabling the technical implementation of this study.
Data Availability
Individual participant data underlying the results presented in this publication (text, tables, figures, and appendices) and statistical code will be shared during the period of 3 months to 5 years following publication of the paper with researchers who provide a methodologically sound proposal to the corresponding author.
Authors' Contributions
SB, MM, and MK conceptualized the study. SB led the grant application. SB, MM, MK, and DL contributed to the study design and selection of screening and outcome measures. DL prepared the technical implementation of this study. DL, AM, EK, and SK prepared the video interventions under the supervision of MM, NA, HB, PP, CRK, RT, and SB, who also provided feedback and information with regard to their fields of expertise. MM generated the random allocation sequence. DL was responsible for study recruitment, which was supported by student assistants. DL analyzed the data, wrote the first draft of this manuscript, and created its tables and figures, with SB and MM providing further feedback, guidance, and supervision during each step. All authors provided feedback on the manuscript. All authors read and approved the final manuscript.
Conflicts of Interest
PP is an advisor for Boehringer Ingelheim and has received speaker’s honoraria from InfectoPharm, GSK, Janssen, and Oral B.
Separate analysis of covariance results and pairwise comparisons for participants with and without previous help-seeking experience.
Separate analysis of covariance results and pairwise comparisons for outcomes per mental health problem.
Separate analysis of covariance results and pairwise comparisons for participants with and without previous help-seeking experience per mental health problem.
CONSORT-eHEALTH Checklist V 1.6.1.
- Gibb SJ, Fergusson DM, Horwood LJ. Burden of psychiatric disorder in young adulthood and life outcomes at age 30. Br J Psychiatry. Aug 2010;197(2):122-127. [ CrossRef ] [ Medline ]
- Weitkamp K, Daniels JK, Romer G, Wiegand-Grefe S. Health-related quality of life of children and adolescents with mental disorders. Health Qual Life Outcomes. Jul 31, 2013;11(1):129. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Sawyer MG, Whaites L, Rey JM, Hazell PL, Graetz BW, Baghurst P. Health-related quality of life of children and adolescents with mental disorders. J Am Acad Child Adolesc Psychiatry. May 2002;41(5):530-537. [ CrossRef ] [ Medline ]
- Romanowska S, MacQueen G, Goldstein BI, Wang J, Kennedy SH, Bray S, et al. Social and role functioning in youth at risk of serious mental illness. Early Interv Psychiatry. Aug 10, 2020;14(4):463-469. [ CrossRef ] [ Medline ]
- Gardner A, Filia K, Killackey E, Cotton S. The social inclusion of young people with serious mental illness: a narrative review of the literature and suggested future directions. Aust N Z J Psychiatry. Jan 2019;53(1):15-26. [ CrossRef ] [ Medline ]
- Erskine HE, Moffitt TE, Copeland WE, Costello EJ, Ferrari AJ, Patton G, et al. A heavy burden on young minds: the global burden of mental and substance use disorders in children and youth. Psychol Med. May 2015;45(7):1551-1563. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Suhrcke M, Pillas D, Selai C. Economic aspects of mental health in children and adolescents. Social Cohesion for Mental Wellbeing among adolescents. 2008. URL: https://pure.york.ac.uk/portal/en/publications/economic-aspects-of-mental-health-in-children-and-adolescents [accessed 2024-04-08]
- Solmi M, Radua J, Olivola M, Croce E, Soardo L, Salazar de Pablo G, et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol Psychiatry. Jan 02, 2022;27(1):281-295. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Kessler RC, Avenevoli S, Costello EJ, Georgiades K, Green JG, Gruber MJ, et al. Prevalence, persistence, and sociodemographic correlates of DSM-IV disorders in the National Comorbidity Survey Replication Adolescent Supplement. Arch Gen Psychiatry. Apr 01, 2012;69(4):372-380. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Hofstra MB, Van Der Ende J, Verhulst FC. Adolescents' self-reported problems as predictors of psychopathology in adulthood: 10-year follow-up study. Br J Psychiatry. Sep 02, 2001;179(3):203-209. [ CrossRef ] [ Medline ]
- Pardini D, White HR, Stouthamer-Loeber M. Early adolescent psychopathology as a predictor of alcohol use disorders by young adulthood. Drug Alcohol Depend. Apr 2007;88 Suppl 1(Suppl 1):S38-S49. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Heijmens Visser JH, van der Ende J, Koot HM, Verhulst FC. Predictors of psychopathology in young adults referred to mental health services in childhood or adolescence. Br J Psychiatry. Jul 02, 2000;177(1):59-65. [ CrossRef ] [ Medline ]
- Reef J, Diamantopoulou S, van Meurs I, Verhulst F, van der Ende J. Child to adult continuities of psychopathology: a 24-year follow-up. Acta Psychiatr Scand. Sep 03, 2009;120(3):230-238. [ CrossRef ] [ Medline ]
- Pearson CM, Miller J, Ackard DM, Loth KA, Wall MM, Haynos AF, et al. Stability and change in patterns of eating disorder symptoms from adolescence to young adulthood. Int J Eat Disord. Jul 15, 2017;50(7):748-757. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Hintzpeter B, Metzner F, Pawils S, Bichmann H, Kamtsiuris P, Ravens-Sieberer U, et al. Inanspruchnahme von ärztlichen und psychotherapeutischen Leistungen durch Kinder und Jugendliche mit psychischen Auffälligkeiten. Kindh Entwickl. Oct 2014;23(4):229-238. [ CrossRef ]
- Wang PS, Aguilar-Gaxiola S, Alonso J, Angermeyer MC, Borges G, Bromet EJ, et al. Use of mental health services for anxiety, mood, and substance disorders in 17 countries in the WHO world mental health surveys. Lancet. Sep 08, 2007;370(9590):841-850. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Cotter P, Kaess M, Corcoran P, Parzer P, Brunner R, Keeley H, et al. Help-seeking behaviour following school-based screening for current suicidality among European adolescents. Soc Psychiatry Psychiatr Epidemiol. Jun 6, 2015;50(6):973-982. [ CrossRef ] [ Medline ]
- Vanheusden K, Mulder CL, van der Ende J, van Lenthe FJ, Mackenbach JP, Verhulst FC. Young adults face major barriers to seeking help from mental health services. Patient Educ Couns. Oct 2008;73(1):97-104. [ CrossRef ] [ Medline ]
- Kaltenthaler E, Sutcliffe P, Parry G, Beverley C, Rees A, Ferriter M. The acceptability to patients of computerized cognitive behaviour therapy for depression: a systematic review. Psychol Med. Nov 2008;38(11):1521-1530. [ CrossRef ] [ Medline ]
- Lawrence D, Johnson S, Hafekost J, Boterhoven de Haan K, Sawyer M, Ainley J, et al. The mental health of children and adolescents: report on the second Australian child and adolescent survey of mental health and wellbeing. Government of Australia. 2015. URL: https://www.health.gov.au/sites/default/files/documents/2020/11/the-mental-health-of-children-and-adolescents_0.pdf [accessed 2024-04-08]
- Lillevoll KR, Vangberg HC, Griffiths KM, Waterloo K, Eisemann MR. Uptake and adherence of a self-directed internet-based mental health intervention with tailored e-mail reminders in senior high schools in Norway. BMC Psychiatry. Jan 21, 2014;14(1):14. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Woodford J, Farrand P, Bessant M, Williams C. Recruitment into a guided internet based CBT (iCBT) intervention for depression: lesson learnt from the failure of a prevalence recruitment strategy. Contemp Clin Trials. Sep 2011;32(5):641-648. [ CrossRef ] [ Medline ]
- Glasgow RE, Estabrooks PE. Pragmatic applications of RE-AIM for health care initiatives in community and clinical settings. Prev Chronic Dis. Jan 04, 2018;15:E02. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. Sep 1999;89(9):1322-1327. [ CrossRef ] [ Medline ]
- Andrade LH, Alonso J, Mneimneh Z, Wells JE, Al-Hamzawi A, Borges G, et al. Barriers to mental health treatment: results from the WHO World Mental Health surveys. Psychol Med. Aug 09, 2013;44(6):1303-1317. [ CrossRef ]
- Mojtabai R, Olfson M, Sampson NA, Jin R, Druss B, Wang PS, et al. Barriers to mental health treatment: results from the National Comorbidity Survey replication. Psychol Med. Aug 2011;41(8):1751-1761. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Gulliver A, Griffiths KM, Christensen H. Perceived barriers and facilitators to mental health help-seeking in young people: a systematic review. BMC Psychiatry. Dec 30, 2010;10:113. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Eisenberg D, Golberstein E, Gollust SE. Help-seeking and access to mental health care in a university student population. Med Care. Jul 2007;45(7):594-601. [ CrossRef ] [ Medline ]
- Clement S, Schauman O, Graham T, Maggioni F, Evans-Lacko S, Bezborodovs N, et al. What is the impact of mental health-related stigma on help-seeking? a systematic review of quantitative and qualitative studies. Psychol Med. Jan 2015;45(1):11-27. [ CrossRef ] [ Medline ]
- Schnyder N, Panczak R, Groth N, Schultze-Lutter F. Association between mental health-related stigma and active help-seeking: systematic review and meta-analysis. Br J Psychiatry. Apr 2017;210(4):261-268. [ CrossRef ] [ Medline ]
- Furnham A, Swami V. Mental health literacy: a review of what it is and why it matters. Int Perspect Psychol. Oct 2018;7(4):240-257. [ CrossRef ]
- Jorm AF. Mental health literacy: empowering the community to take action for better mental health. Am Psychol. Apr 2012;67(3):231-243. [ CrossRef ] [ Medline ]
- Patafio B, Miller P, Baldwin R, Taylor N, Hyder S. A systematic mapping review of interventions to improve adolescent mental health literacy, attitudes and behaviours. Early Interv Psychiatry. Dec 03, 2021;15(6):1470-1501. [ CrossRef ] [ Medline ]
- Howard KA, Griffiths KM, McKetin R, Ma J. Can a brief biologically-based psychoeducational intervention reduce stigma and increase help-seeking intentions for depression in young people? a randomised controlled trial. J Child Adolesc Ment Health. May 15, 2018;30(1):27-39. [ CrossRef ] [ Medline ]
- Jaber R, Farroukh M, Ismail M, Najda J, Sobh H, Hammad A, et al. Measuring depression and stigma towards depression and mental health treatment among adolescents in an Arab-American community. Int J Cult Ment Health. Sep 24, 2015;8(3):247-254. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Bruning Brown J, Winzelberg AJ, Abascal LB, Taylor CB. An evaluation of an internet-delivered eating disorder prevention program for adolescents and their parents. J Adolesc Health. Oct 2004;35(4):290-296. [ CrossRef ] [ Medline ]
- O'Kearney R, Kang K, Christensen H, Griffiths K. A controlled trial of a school-based internet program for reducing depressive symptoms in adolescent girls. Depress Anxiety. 2009;26(1):65-72. [ CrossRef ] [ Medline ]
- Baumel A, Fleming T, Schueller SM. Digital micro interventions for behavioral and mental health gains: core components and conceptualization of digital micro intervention care. J Med Internet Res. Oct 29, 2020;22(10):e20631. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Ebert DD, Franke M, Kählke F, Küchler AM, Bruffaerts R, Mortier P, et al. WHO World Mental Health - International College Student collaborators. Increasing intentions to use mental health services among university students. Results of a pilot randomized controlled trial within the World Health Organization's World Mental Health International college student initiative. Int J Methods Psychiatr Res. Jun 2019;28(2):e1754. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Amsalem D, Markowitz JC, Jankowski SE, Yang LH, Valeri L, Lieff SA, et al. Sustained effect of a brief video in reducing public stigma toward individuals with psychosis: a randomized controlled trial of young adults. Am J Psychiatry. Jul 26, 2021;178(7):635-642. [ CrossRef ] [ Medline ]
- Amsalem D, Jankowski SE, Pagdon S, Valeri L, Smith S, Yang LH, et al. "It is hard to be a woman with schizophrenia": randomized controlled trial of a brief video intervention to reduce public stigma in young adults. J Clin Psychiatry. Dec 19, 2022;84(1):22m14534. [ CrossRef ] [ Medline ]
- Amsalem D, Martin A. Reducing depression-related stigma and increasing treatment seeking among adolescents: randomized controlled trial of a brief video intervention. J Child Psychol Psychiatry. Feb 06, 2022;63(2):210-217. [ CrossRef ] [ Medline ]
- Conceição V, Rothes I, Gusmão R. The effects of a video-based randomized controlled trial intervention on depression stigma and help-seeking attitudes in university students. Psychiatry Res. Feb 2022;308:114356. [ CrossRef ] [ Medline ]
- Clough BA, Nazareth SM, Casey LM. Making the grade: a pilot investigation of an e-intervention to increase mental health literacy and help-seeking intentions among international university students. Br J Guid Couns. Oct 03, 2019;48(3):347-359. [ CrossRef ]
- Gaudiano BA, Davis CH, Miller IW, Uebelacker L. Pilot randomized controlled trial of a video self-help intervention for depression based on acceptance and commitment therapy: feasibility and acceptability. Clin Psychol Psychother. May 28, 2020;27(3):396-407. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Fong TH, Mak WW. The effects of internet-based storytelling programs (amazing adventure against stigma) in reducing mental illness stigma with mediation by interactivity and stigma content: randomized controlled trial. J Med Internet Res. Aug 12, 2022;24(8):e37973. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Logsdon CM, Myers J, Rushton J, Gregg JL, Josephson AM, Davis DW, et al. Efficacy of an internet-based depression intervention to improve rates of treatment in adolescent mothers. Arch Womens Ment Health. Jun 2018;21(3):273-285. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Schwarzer R, Luszczynska A. How to overcome health-compromising behaviors. Eur Psychol. Jan 2008;13(2):141-151. [ CrossRef ]
- Zhang CQ, Zhang R, Schwarzer R, Hagger MS. A meta-analysis of the health action process approach. Health Psychol. Jul 2019;38(7):623-637. [ CrossRef ] [ Medline ]
- Fishbein M, Ajzen I. Predicting and Changing Behavior: The Reasoned Action Approach. New York, NY. Psychology Press; 2010.
- Yeager CM, Shoji K, Luszczynska A, Benight CC. Engagement with a trauma recovery internet intervention explained with the Health Action Process Approach (HAPA): longitudinal study. JMIR Ment Health. Apr 10, 2018;5(2):e29. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Eysenbach G. Improving the quality of web surveys: the checklist for reporting results of internet E-surveys (CHERRIES). J Med Internet Res. Sep 29, 2004;6(3):e34. [ CrossRef ] [ Medline ]
- Eysenbach G, CONSORT-EHEALTH Group. CONSORT-EHEALTH: improving and standardizing evaluation reports of web-based and mobile health interventions. J Med Internet Res. Dec 31, 2011;13(4):e126. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Santelli JS, Rosenfeld WD, DuRant RH, Dubler N, Morreale M, English A, et al. Guidelines for adolescent health research: a position paper of the society for adolescent medicine. J Adolesc Health. Nov 1995;17(5):270-276. [ CrossRef ] [ Medline ]
- Schachter D, Kleinman I, Harvey W. Informed consent and adolescents. Can J Psychiatry. Aug 01, 2005;50(9):534-540. [ CrossRef ] [ Medline ]
- Arnett JJ. Emerging adulthood: a theory of development from the late teens through the twenties. Am Psychol. 2000;55(5):469-480. [ CrossRef ]
- Mehta CM, Arnett JJ, Palmer CG, Nelson LJ. Established adulthood: a new conception of ages 30 to 45. Am Psychol. May 2020;75(4):431-444. [ CrossRef ] [ Medline ]
- Wilhelm M, Feldhege J, Bauer S, Moessner M. Einsatz internetbasierter verlaufsmessung in der psychotherapieforschung. Psychotherapeut. Oct 12, 2020;65(6):505-511. [ CrossRef ]
- Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. May 22, 2006;166(10):1092-1097. [ CrossRef ] [ Medline ]
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. Sep 2001;16(9):606-613. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Killen JD, Taylor CB, Hammer LD, Litt I, Wilson DM, Rich T, et al. An attempt to modify unhealthful eating attitudes and weight regulation practices of young adolescent girls. Int J Eat Disord. May 1993;13(4):369-384. [ CrossRef ] [ Medline ]
- Killen JD, Taylor CB, Hayward C, Wilson DM, Haydel KF, Hammer LD, et al. Pursuit of thinness and onset of eating disorder symptoms in a community sample of adolescent girls: a three-year prospective analysis. Int J Eat Disord. Nov 1994;16(3):227-238. [ CrossRef ] [ Medline ]
- Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA. The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Ambulatory care quality improvement project (ACQUIP). Alcohol use disorders identification test. Arch Intern Med. Sep 14, 1998;158(16):1789-1795. [ CrossRef ] [ Medline ]
- Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption--II. Addiction. Jun 1993;88(6):791-804. [ CrossRef ] [ Medline ]
- Kuitunen-Paul S, Roerecke M. Alcohol Use isorders Identification Test (AUDIT) and mortality risk: a systematic review and meta-analysis. J Epidemiol Community Health. Sep 2018;72(9):856-863. [ CrossRef ] [ Medline ]
- Fischer G, Ameis N, Parzer P, Plener PL, Groschwitz R, Vonderlin E, et al. The German version of the self-injurious thoughts and behaviors interview (SITBI-G): a tool to assess non-suicidal self-injury and suicidal behavior disorder. BMC Psychiatry. Sep 18, 2014;14(1):265. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Home page. Powtoon. URL: https://www.powtoon.com/ [accessed 2024-04-08]
- Wright A, Jorm AF, Mackinnon AJ. Labels used by young people to describe mental disorders: which ones predict effective help-seeking choices? Soc Psychiatry Psychiatr Epidemiol. Jun 2012;47(6):917-926. [ CrossRef ] [ Medline ]
- Mond JM, Hay PJ, Paxton SJ, Rodgers B, Darby A, Nillson J, et al. Eating disorders "mental health literacy" in low risk, high risk and symptomatic women: implications for health promotion programs. Eat Disord. 2010;18(4):267-285. [ CrossRef ] [ Medline ]
- DeJong H, Hillcoat J, Perkins S, Grover M, Schmidt U. Illness perception in bulimia nervosa. J Health Psychol. Apr 2012;17(3):399-408. [ CrossRef ] [ Medline ]
- Bulik CM. Towards a science of eating disorders: replacing myths with realities: the fourth Birgit Olsson lecture. Nord J Psychiatry. Sep 10, 2016;70(3):224-230. [ CrossRef ] [ Medline ]
- Keski-Rahkonen A, Mustelin L. Epidemiology of eating disorders in Europe: prevalence, incidence, comorbidity, course, consequences, and risk factors. Curr Opin Psychiatry. Nov 2016;29(6):340-345. [ CrossRef ] [ Medline ]
- Nagl M, Jacobi C, Paul M, Beesdo-Baum K, Höfler M, Lieb R, et al. Prevalence, incidence, and natural course of anorexia and bulimia nervosa among adolescents and young adults. Eur Child Adolesc Psychiatry. Aug 2016;25(8):903-918. [ CrossRef ] [ Medline ]
- Laberg S, Törnkvist Å, Andersson G. Experiences of patients in cognitive behavioural group therapy: a qualitative study of eating disorders. Cogn Behav Ther. Jan 2001;30(4):161-178. [ CrossRef ]
- Wilson CJ, Deane FP, Ciarrochi J, Rickwood D. Measuring help-seeking intentions: properties of the general help-seeking questionnaire. Can J Couns. 2005;39(1):15-28. [ FREE Full text ]
- Divin N, Harper P, Curran E, Corry D, Leavey G. Help-seeking measures and their use in adolescents: a systematic review. Adolescent Res Rev. Jan 17, 2018;3(1):113-122. [ CrossRef ]
- Mackenzie CS, Knox VJ, Gekoski WL, Macaulay HL. An adaptation and extension of the attitudes toward seeking professional psychological help scale. J Applied Social Pyschol. Jul 31, 2006;34(11):2410-2433. [ CrossRef ]
- Ebneter DS, Latner JD. Stigmatizing attitudes differ across mental health disorders: a comparison of stigma across eating disorders, obesity, and major depressive disorder. J Nerv Ment Dis. Apr 2013;201(4):281-285. [ CrossRef ] [ Medline ]
- Appel M, Gnambs T, Richter T, Green MC. The Transportation Scale–Short Form (TS–SF). Media Psychol. Feb 03, 2015;18(2):243-266. [ CrossRef ]
- Faul F, Erdfelder E, Lang A, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. May 2007;39(2):175-191. [ CrossRef ]
- R Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing. URL: https://www.r-project.org/ [accessed 2024-04-08]
- IBM SPSS Statistics for Windows, version 28.0. IBM Corp. URL: https://www.ibm.com/support/pages/downloading-ibm-spss-statistics-28010 [accessed 2024-04-08]
- Lienemann BA, Siegel JT, Crano WD. Persuading people with depression to seek help: respect the boomerang. Health Commun. Oct 2013;28(7):718-728. [ CrossRef ] [ Medline ]
- Lienemann BA, Siegel JT. State psychological reactance to depression public service announcements among people with varying levels of depressive symptomatology. Health Commun. Jun 18, 2016;31(1):102-116. [ CrossRef ] [ Medline ]
- Siegel JT, Lienemann BA, Rosenberg BD. Resistance, reactance, and misinterpretation: highlighting the challenge of persuading people with depression to seek help. Soc Pers Psychol Compass. Jun 05, 2017;11(6):e12322. [ CrossRef ]
- van Laer T, de Ruyter K, Visconti LM, Wetzels M. The extended transportation-imagery model: a meta-analysis of the antecedents and consequences of consumers' narrative transportation. J Consum Res. Feb 01, 2014;40(5):797-817. [ FREE Full text ] [ CrossRef ]
- Murphy ST, Frank LB, Chatterjee JS, Baezconde-Garbanati L. Narrative versus non-narrative: the role of identification, transportation and emotion in reducing health disparities. J Commun. Feb 07, 2013;63(1):116-137. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Sowislo JF, Gonet-Wirz F, Borgwardt S, Lang UE, Huber CG. Perceived dangerousness as related to psychiatric symptoms and psychiatric service use - a vignette based representative population survey. Sci Rep. Apr 03, 2017;8(1):45716. [ FREE Full text ] [ CrossRef ] [ Medline ]
- McVay MA, Bennett GG, Steinberg D, Voils CI. Dose-response research in digital health interventions: concepts, considerations, and challenges. Health Psychol. Dec 2019;38(12):1168-1174. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Suka M, Yamauchi T, Yanagisawa H. Comparing responses to differently framed and formatted persuasive messages to encourage help-seeking for depression in Japanese adults: a cross-sectional study with 2-month follow-up. BMJ Open. Nov 12, 2018;8(11):e020823. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Kaushik A, Kostaki E, Kyriakopoulos M. The stigma of mental illness in children and adolescents: a systematic review. Psychiatry Res. Sep 30, 2016;243:469-494. [ CrossRef ] [ Medline ]
- Misra S, Jackson VW, Chong J, Choe K, Tay C, Wong J, et al. Systematic review of cultural aspects of stigma and mental illness among racial and ethnic minority groups in the United States: implications for interventions. Am J Community Psychol. Dec 2021;68(3-4):486-512. [ CrossRef ] [ Medline ]
- Papadopoulos C, Foster J, Caldwell K. 'Individualism-collectivism' as an explanatory device for mental illness stigma. Community Ment Health J. Jun 27, 2013;49(3):270-280. [ CrossRef ] [ Medline ]
Abbreviations
Edited by G Eysenbach, T de Azevedo Cardoso; submitted 13.11.23; peer-reviewed by A Morgan; comments to author 15.12.23; revised version received 22.12.23; accepted 08.03.24; published 24.04.24.
©Diana Lemmer, Markus Moessner, Nicolas Arnaud, Harald Baumeister, Agnes Mutter, Sarah-Lena Klemm, Elisa König, Paul Plener, Christine Rummel-Kluge, Rainer Thomasius, Michael Kaess, Stephanie Bauer. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 24.04.2024.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work, first published in the Journal of Medical Internet Research, is properly cited. The complete bibliographic information, a link to the original publication on https://www.jmir.org/, as well as this copyright and license information must be included.
- Research Note
- Open access
- Published: 22 April 2024
Impact of the COVID-19 pandemic on utilization and cost for care of pediatric and young adult ALL
- Alex Hoover 1 ,
- Dave Watson 2 ,
- Paige Reimche 2 ,
- Lynn Tanner 2 ,
- Laura Gilchrist 2 , 3 ,
- Mike Finch 2 ,
- Yoav H Messinger 2 &
- Lucie M. Turcotte 1
BMC Research Notes volume 17 , Article number: 112 ( 2024 ) Cite this article
66 Accesses
2 Altmetric
Metrics details
Acute lymphoblastic leukemia (ALL) is the most common childhood malignancy and among the most common malignancies in young adults and requires a unique pattern of healthcare utilization including an acute/emergent presentation and an intensive initial 8 months of therapy followed by two years of outpatient treatment. The COVID-19 pandemic caused massive global disruptions in healthcare use and delivery. This report aims to examine the effects of the COVID-19 pandemic on the presentation, diagnosis and continued management of childhood and young adult ALL in regard to utilization and cost of care among commercially insured individuals in the United States.
Utilizing a commercial insurance claims database, 529 pediatric and young adult patients were identified who were diagnosed with ALL between January 2016 and March 2021. New diagnoses were evaluated by era and demographics. Utilization was measured by COVID-related era as number of inpatient and outpatient encounters, inpatient days, and cumulative cost during the initial 8 months of therapy. None of these cost or utilization factors changed significantly during or shortly after the pandemic. These findings reinforce that the necessary care for pediatric and young adult ALL was unwavering despite the massive shifts in the healthcare system caused by the COVID-19 pandemic. This provides a valuable benchmark as we further examine the factors that influence the pandemic’s impact on health equity and access to care, especially in vulnerable pediatric and young adult populations. This is the first investigation of the effect of the COVID-19 pandemic on utilization and cost of care in pediatric and young adult cancer.
Peer Review reports
Introduction
Acute lymphoblastic leukemia (ALL) is the most common cancer of childhood and adolescence, with approximately 3000 new cases diagnosed each year in individuals under age 18 years of age in the United States (US) [ 1 ]. Although the incidence decreases with age, it remains among the most common malignancies for young adults as well [ 1 ]. The COVID-19 pandemic affected healthcare use and delivery across the United States and internationally, with multiple studies showing decreased healthcare utilization in both the emergency and ambulatory setting, particularly in the early months of the pandemic [ 2 , 3 , 4 ]. A reduction in visits due to patient fear of infection and reduced access to typical care due to public health regulations led to dramatic reductions in the use of preventive and elective care, including cancer-related care, during the first and second quarter of 2020 [ 5 ]. Pediatric and young adult ALL requires unique healthcare utilization including elements of acute/emergent presentation, an intensive initial 6–8 months of treatment and nearly two years of lower intensity outpatient treatment. We sought to examine the effects of the COVID-19 pandemic on the presentation, diagnosis and continued management of childhood ALL in regard to utilization and cost of healthcare and to examine whether changes in use and cost differ by patient characteristics.
Using de-identified commercial insurance data from the OptumLabs® Data Warehouse, a cohort of patients with ALL was identified, aged 1–30 years and diagnosed between January 2016 and March 2021 in the United States. The ages for inclusion were selected based on inclusion criteria for previous Children’s Oncology Group ALL treatment protocols, which included individuals aged 1–30 years. Notably, the most recent ALL protocol (AALL1732), which opened in June 2019, included individuals aged 1–25 years; however, many individuals treated for ALL as young adults are treated based on pediatric ALL protocols. Date of ALL diagnosis was confirmed based on initial ICD-9 and ICD-10 diagnostic codes (204.00, 204.01, 204.02 and C91.00, C91.01, C91.02, respectively) in combination with either a CPT code for bone marrow biopsy or lumbar puncture within 14 days of the first ALL diagnostic code. Total number of new diagnoses were identified and stratified by timing of diagnosis, including early pre-COVID era (1/2016–6/2019), overlap COVID era (7/2019–3/2020), and COVID era (4/2020–3/2021). New diagnoses were also evaluated by age, sex and region of the US for differences in diagnostic patterns. Utilization was measured as number of inpatient and outpatient encounters, inpatient days, and cumulative cost (inflation adjusted) for the initial 8 months of therapy. Associations of demographics and utilization outcomes with era of diagnosis were assessed using chi-square test (or Fisher exact test when necessary) and Kruskal-Wallis test. R was used for statistical analyses [ 6 ].
Among the 529 identified pediatric and young adult ALL patients diagnosed within the predetermined timeframe, 42.5% were female and median age at diagnosis was 7 years (interquartile range 4–15 years). There were 363 new ALL diagnoses in the pre-COVID era, 63 in the overlap COVID era, and 103 in the COVID era. These frequencies were proportional to the length of the respective eras with 8.6, 7.0, and 8.6 diagnoses per month, respectively (goodness-of-fit chi-square p = 0.29). Patient characteristics of new ALL diagnoses across all three eras were similar with respect to age, sex, and geographic region (Table 1 ).
Utilization for all four measures were similar across all three eras (Figure 1 ). Over the first 8 months of therapy, the median utilization was 5 inpatient encounters, 64 outpatient encounters, 38 total inpatient days, and $495,000 for cumulative cost of care; these values did not vary significantly by era (all p > 0.05, Table 1 ).

Inpatient/outpatient encounters, inpatient days and cost by COVID era (Pre-COVID era (1/2016–6/2019), overlap COVID era (7/2019–3/2020), and COVID era (4/2020–3/2021))
This real-world cost analysis shows for the first time the effect of the COVID-19 pandemic on patterns of care for pediatric and young adult ALL– encompassing not only the pattern of new diagnoses but also patterns of care and cost during the initial 8 months of intensive therapy. We show that the number of inpatient and outpatient encounters, inpatient days and cost of care did not change significantly during the pandemic, reinforcing the fact that the care for pediatric and young adult ALL was unwavering despite the massive shifts in the healthcare system caused by the COVID-19 pandemic. Although the median cost increased between the pre-COVID and COVID eras, the change was not statistically significant and variability in cost was relatively large, consistent with our previous report [ 7 ].
Investigations into pandemic-related changes in care for other pediatric diseases that require significant medical care and attention at diagnosis include diabetic ketoacidosis (DKA) for new-onset type 1 diabetes have found an increase in incidence of DKA and severe DKA [ 8 ]. Shifts in access to primary care and patient fear of infection with accessing the healthcare system have been attributed to these alterations in diabetes presentation and DKA severity [ 9 ].
However, in the face of major decreases in preventative and elective healthcare shown in other studies, we have shown that care for pediatric and young adult ALL continued at a steady rate throughout the early pandemic time period. This study provides a valuable benchmark of patterns that can be reassessed over time as we attempt to further examine the factors that influence the pandemic’s impact on health equity and access to care, especially in vulnerable pediatric and young adult populations.
Limitations
Despite the many strengths of this study, limitations must be acknowledged. The use of claims data relies on accurate and consistent coding, which can make it difficult to ascertain the exact date of diagnosis or relapse. We were unable to comprehensively evaluate racial or ethnic differences in pandemic-era ALL cost or care utilization given the large proportion of individuals with missing or undefined race and ethnicity data. Additionally, the OptumLabs Data Warehouse is limited to commercially insured individuals, thus excluding publicly insured or managed care patients from this analysis and limiting the generalizability of these results.
Data availability
The dataset supporting the conclusions of this article is available in the OptumLabs data repository, with restricted access but available upon request.
Abbreviations
Acute lymphoblastic leukemia
Diabetic ketoacidosis
International statistical Classification of Diseases
United States
Howlader NNA, Krapcho M, Miller D, Brest A, Yu M, Ruhl J, Tatalovich ZMA, Lewis DR, Chen HS, Feuer EJ, Cronin KA, editors. SEER Cancer Statistics Review, 1975–2018. Based on November 2020 SEER data submission, posted to the SEER web site, April 2021. ed: National Cancer Institute. Bethesda, MD.
Whaley CM, Pera MF, Cantor J, Chang J, Velasco J, Hagg HK, et al. Changes in health services use among commercially insured US populations during the COVID-19 pandemic. JAMA Netw Open. 2020;3(11):e2024984.
Article PubMed PubMed Central Google Scholar
Pujolar G, Oliver-Anglès A, Vargas I, Vázquez ML. Changes in access to health services during the COVID-19 pandemic: a scoping review. Int J Environ Res Public Health. 2022;19(3).
Sato K, Mano T, Niimi Y, Iwata A, Toda T, Iwatsubo T. The impact of COVID-19 pandemic on the utilization of ambulatory care for patients with chronic neurological diseases in Japan: evaluation of an administrative claims database. Biosci Trends. 2021;15(4):219–30.
Article CAS PubMed Google Scholar
Patt D, Gordan L, Diaz M, Okon T, Grady L, Harmison M, et al. Impact of COVID-19 on cancer care: how the pandemic is delaying cancer diagnosis and treatment for American seniors. JCO Clin Cancer Inf. 2020;4:1059–71.
Article Google Scholar
Team RC. R: a language and environment for statistical computing. Vienna A, R Foundation for Statistical Computing.
Turcotte LM, Watson D, Tanner L, Hoover A, Gilchrist L, Finch M, et al. Real-world cost of pediatric acute lymphoblastic leukemia care among commercially insured individuals in the United States: effect of era and age at diagnosis. JCO Oncol Pract. 2022;18(11):e1750–61.
Elgenidy A, Awad AK, Saad K, Atef M, El-Leithy HH, Obiedallah AA et al. Incidence of diabetic ketoacidosis during COVID-19 pandemic: a meta-analysis of 124,597 children with diabetes. Pediatr Res. United States: © 2022. The Author(s), under exclusive licence to the International Pediatric Research Foundation, Inc.; 2022. pp. 1–12.
Rabbone I, Schiaffini R, Cherubini V, Maffeis C, Scaramuzza A. Has COVID-19 delayed the diagnosis and worsened the presentation of type 1 diabetes in children? Diabetes Care. 2020;43(11):2870–2.
Download references
This work was supported in part by the NIH-NRSA Research Fellowship in Translational & Genomic Pediatric Cancer Epidemiology - T32CA099936 (AH), the National Cancer Institute Grant No. K08CA234232 (LMT); the Pine Tree Apple Classic Fund (LG, YHM); and the Children’s Cancer Research Fund (LMT).
Author information
Authors and affiliations.
Optum Labs Visiting Fellow, Division of Pediatric Blood and Marrow Transplantation, University of Minnesota Medical School, Mayo Mail Code 366, 420 Delaware St SE, 55455, Minneapolis, MN, USA
Alex Hoover & Lucie M. Turcotte
Children’s Minnesota, Minneapolis, MN, USA
Dave Watson, Paige Reimche, Lynn Tanner, Laura Gilchrist, Mike Finch & Yoav H Messinger
St. Catherine University, St. Paul, MN, USA
Laura Gilchrist
You can also search for this author in PubMed Google Scholar
Contributions
Dr. Alex Hoover and Dr. Lucie Turcotte conceptualized and designed the study, drafted the initial manuscript, and critically reviewed and revised the manuscript. Dr. Dave Watson and Dr. Mike Finch, and Paige Reimche designed the data collection instruments, collected data, carried out the initial analyses, and critically reviewed and revised the manuscript. Dr. Lynn Tanner, Dr. Laura Gilchrist and Dr. Yoav Messinger critically reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Correspondence to Alex Hoover .
Ethics declarations
Ethics approval and consent to participate.
All methods were carried out in accordance with relevant guidelines and regulations. This study was reviewed by the Institutional Review Board of the University of Minnesota on 7/19/2021 and assigned a determination of “Not Human Research” under exemption clause 4: “Collection or study of existing data, documents, records, pathological specimens, or diagnostic specimens if publicly available or information is recorded by investigator in a manner that subjects cannot be identified.” Therefore, the need for informed consent was waived by the IRB of the University of Minnesota.
Consent for publication
Not applicable– no identifiable data present.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Hoover, A., Watson, D., Reimche, P. et al. Impact of the COVID-19 pandemic on utilization and cost for care of pediatric and young adult ALL. BMC Res Notes 17 , 112 (2024). https://doi.org/10.1186/s13104-024-06768-x
Download citation
Received : 04 December 2023
Accepted : 04 April 2024
Published : 22 April 2024
DOI : https://doi.org/10.1186/s13104-024-06768-x
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Young adult
- Acute Lymphoblastic Leukemia (ALL)
- Utilization
BMC Research Notes
ISSN: 1756-0500
- Submission enquiries: [email protected]
- General enquiries: [email protected]
IMAGES
VIDEO
COMMENTS
Mental health conditions typically begin during childhood, adolescence or young adulthood. Here you will find additional information intended to help provide young people, educators, parents and caregivers with the resources they need. From a free downloadable coloring and activity book to a teen mental heath education presentation, to a guide for navigating college with a […]
YouTube Series in supporting young adults? Check out this development and the role of MCH • Young Adults and MCH - Do you work in MCH? Wonder what your role is video exploring young adult programs. (14:10 min) • 10 Things MCH Should Know About Young Adults - Important tips for understanding and working with young adults.(18:49 min)
Key facts. Over 1.5 million adolescents and young adults aged 10-24 years died in 2021, about 4500 every day. Young adolescents aged 10-14 years have the lowest risk of death among all age groups. Injuries (including road traffic injuries and drowning), interpersonal violence, self-harm and maternal conditions are the leading causes of ...
While majorities across all age groups say young adults have it harder when it comes to buying a home, saving for the future and paying for college, Americans ages 18 to 29 are more likely than older age groups to say this. More than eight-in-ten adults younger than 30 (84%) say buying a home is harder for young adults today, while 80% say the ...
Have the Right Frame of Mind. Speakers should approach a young audience with one very important understanding - young people are genuine. Young audiences openly express feelings where adults often pretend. When young people don't like what's being said, they will never act like they do.
Public Speaking Tip 2: Body Language. Body language can make a big difference in how your message is perceived. Sit/stand up straight. Use your hands as you talk (but not too much) and avoid crossing your arms. Maintain eye contact with your audience to establish connection, trust, and show confidence.
This chapter provides a foundation for the remainder of the report. It summarizes current knowledge regarding young adulthood as a critical developmental period in the life course; highlights historical patterns and recent trends in the social and economic transitions of young adults in the United States; reviews data on the health status of the current cohort of young adults; briefly ...
Free Google Slides theme and PowerPoint template. Adolescence is an exciting time for young people as they explore their unique personalities and talents. With this captivating Life Stages presentation, you can help parents, teachers, and counselors lead adolescents through this crucial period. Featuring stylish graphics, vibrant colors, and ...
Provide helpful materials, but don't overwhelm your participants. It can be useful for participants to have a tip sheet or a summary of some key information from the presentation, but too many materials can be overwhelming. Providing participants with all the information and notes can make them feel like they do not need to be engaged.
Watch on. Teens and young adults can lose interest in their faith. Here's a topic that can get their attention in a powerful way! A fast-moving, wonderful introduction to Eucharistic miracles, the stigmata, incorrupt bodies, and more, Elizabeth delivers a presentation that is educational and engaging for teens and young adults.
examples from when they were young. Adults can be well-intentioned, but often, young people report feeling tokenized or under-utilized, or worse yet, disrespected. When youth are meaningfully engaged in the planning and execution of a workshop or presentation, it can benefit everyone and ensure that adults are not speaking on behalf of youth.
• aims to support others working to improve the health and well-being of young adults. Pre-COVID-19, depression and anxiety among young adults was already on the rise. • Young adult past-month serious anxiety increased from 8% in 2008 to 15% in 2018. These rates and this 87% increase are higher than for any other adult age group.
The Civic Outlook of Young Adults in America is a first-of-its-kind national survey of 18-24-year-old Americans that sheds light on their civic knowledge, civic engagement, and commitment to democracy. Part of our multi-year research initiative to measure holistic youth civic preparedness in America, Citizens & Scholars commissioned Citizen ...
Youth Presentations. myHealth for Teens & Young Adults' education team is comprised of professional speakers that are knowledgeable about the issues teens and young adults face. myHealth facilitates presentations in classrooms or any other community space. myHealth educators come out to schools, alternative learning centers, transition ...
•Among young adults aged 18-25, 1 in 3 struggle with a diagnosable mental health disorder* •64% of young adults who end college early do so because of a mental health related reason (depression, bipolar disorder, and PTSD being most common)* •Between 1999-2017, the age-adjusted suicide rate increased 33% among males and females**
Mental ill-health in Australian youth. 10. Young Minds Matter Survey (2015) www.youngmindsmatter.org.au • 1 in 7, 4 - 17 year olds had a mental health problem in the previous 12 months = 560,000 children • Prevalence rates stable but illnesses have changed: • in ADHD • in depression • Prevalence in families where other risk factors ...
Young Adults And Their Mental Health-Related Issues. Youth and typical mental health problems feel tense, have interpersonal problems, have concerns about money, acquire a drug or alcohol issue, struggling at work or in school, need assistance caring for a child, esteem oneself poorly, feel overweight or underweight, encounter harassment at work or online, and being lonely.
Levy, A. and A. Perry, Outcomes in adolescents and adults with autism: A review of the literature. Research in Autism Spectrum Disorders, 2011. 5(4): p. 1271-1282. Taylor, J.L. and M.M. Seltzer, Employment and post-secondary educational activities for young adults with autism spectrum disorders during the transition to adulthood.
Adolescents and young adults benefit greatly by learning to use self-care as a coping strategy for life. These three exercises are designed to help youths think about how they can incorporate more self-care activities into their daily lives, for increased mental and physical wellbeing. Self-Care Vision Board
Adolescents and Young Adults. Print. While sexually transmitted diseases (STDs) affect individuals of all ages, STDs take a particularly heavy toll on young people. CDC estimates that youth ages 15-24 account for almost half of the 26 million new sexually transmitted infections that occurred in the United States in 2018.
Young Adulthood . The adult phase of development encompasses the years from the end of adolescence to death: Young adulthood 20 - 40 Middle adulthood 40 - 65 Late adulthood over 65. Maturity: the state of maximal function and integrating or the state of being fully developed.
Free Google Slides theme, PowerPoint template, and Canva presentation template. Download the "Young People Theme" presentation for PowerPoint or Google Slides and start impressing your audience with a creative and original design. Slidesgo templates like this one here offer the possibility to convey a concept, idea or topic in a clear, concise ...
Money Smart for Young People. FDIC Money Smart for Young People features four free age-appropriate curricula that promote financial understanding and are specifically designed for pre-kindergarten through 12th grade educators. Each curriculum includes: FDIC Money Smart News for Kids was based on the Money Smart for Young People, grades 3-5 ...
Among parents whose young adult children have kids of their own, 40% say they disagree with them at least sometimes about how they're raising their children. Parents whose youngest adult child is 25 or older are more likely than those with a child age 18 to 24 to say they rarely or never disagree about their children's finances or social ...
Despite the existence of effective treatment, the uptake of professional help is low, particularly due to attitudinal barriers. Objective: This study evaluated the effectiveness and acceptability of 2 video-based microinterventions aimed at reducing barriers to MH treatment and increasing the likelihood of seeking professional help in young people.
Acute lymphoblastic leukemia (ALL) is the most common childhood malignancy and among the most common malignancies in young adults and requires a unique pattern of healthcare utilization including an acute/emergent presentation and an intensive initial 8 months of therapy followed by two years of outpatient treatment. The COVID-19 pandemic caused massive global disruptions in healthcare use and ...