
Vitamin E is a fat-soluble vitamin with several forms, but alpha-tocopherol is the only one used by the human body. Its main role is to act as an antioxidant, scavenging loose electrons—so-called “free radicals”—that can damage cells. [1] It also enhances immune function and prevents clots from forming in heart arteries. Antioxidant vitamins, including vitamin E, came to public attention in the 1980s when scientists began to understand that free radical damage was involved in the early stages of artery-clogging atherosclerosis, and might also contribute to cancer, vision loss, and a host of other chronic conditions. Vitamin E has the ability to protect cells from free radical damage as well as reduce the production of free radicals in certain situations. However, conflicting study results have dimmed some of the promise of using high dose vitamin E to prevent chronic diseases.

Recommended Amounts
The Recommended Dietary Allowance (RDA) for vitamin E for males and females ages 14 years and older is 15 mg daily (or 22 international units, IU), including women who are pregnant. Lactating women need slightly more at 19 mg (28 IU) daily.
Vitamin E and Health
For a time, vitamin E supplements looked like an easy way to prevent cardiovascular disease. The U.S. Preventive Services Task Force’s latest review of evidence from clinical trials found no conclusive benefit of vitamin E supplements for the prevention of cardiovascular disease, and therefore recommended against their use. [2] Although some large observational studies and clinical trials have shown a heart-protective benefit from these supplements, particularly in relatively healthy people, most randomized clinical trials have shown no benefit in either healthy people or those at risk for, or with, heart disease.
Benefit Found
- Observational studies: The Nurses’ Health Study [3] and Health Professionals Follow-Up Study [4] suggested 20-40% reductions in heart disease risk among individuals who took vitamin E supplements (usually containing 400 IU or more) for at least two years. [5]
- Randomized controlled trials: In the Women’s Health Study, which followed almost 40,000 healthy women for 10 years, vitamin E supplements of 600 IU taken every other day did not significantly reduce the risk of so-called “major cardiac events” (heart attack, stroke, or cardiovascular death). But there was some encouraging news in the findings: When these major cardiac events were analyzed separately, vitamin E supplementation was linked to a 24% lower risk of cardiovascular death. [6] And among women ages 65 and older, vitamin E supplementation reduced the risk of major cardiac events by 26%. A later analysis found that women who took the vitamin E supplements also had a lower risk of developing serious blood clots in the legs and lungs, with women at the highest risk of such blood clots receiving the greatest benefit. [7]
No Benefit Found
- Randomized controlled trials in people who were at high risk for or who had heart disease at baseline. In the GISSI Prevention Trial, the results were mixed but mostly showed no preventive effects after more than three years of treatment with vitamin E among 11,000 heart attack survivors. [8] Results from the Heart Outcomes Prevention Evaluation (HOPE) trial also showed no benefit of four years’ worth of vitamin E supplementation in more than 9,500 men and women already diagnosed with heart disease or at high risk for it. [9] In fact, when the HOPE trial was extended for another four years, researchers found that study volunteers who took vitamin E had a higher risk of heart failure. [10]
Based on such studies, the American Heart Association concluded that “the scientific data do not justify the use of antioxidant vitamin supplements (such as vitamin E) for CVD risk reduction.” [11] It is possible that in people who already have heart disease or are at high risk of heart disease, the use of drugs such as aspirin, beta blockers, and ACE inhibitors mask a modest effect of vitamin E, and that vitamin E may have benefits among healthier people.
- Randomized controlled trials in people without heart disease at baseline. The SU.VI.MAX randomized controlled trial found that seven years of low-dose vitamin E supplementation (as part of a daily antioxidant pill) reduced the risk of cancer and the risk of dying from any cause in men, but did not show these beneficial effects in women; the supplements did not offer any protection against heart disease in men or women. [12] Discouraging results have also come from the Physicians’ Health Study II, an eight-year randomized controlled trial that involved nearly 15,000 middle-aged men, most of whom were free of heart disease at the start of the study. Researchers found that taking vitamin E supplements of 400 IU every other day, alone or with vitamin C, failed to offer any protection against heart attacks, strokes, or cardiovascular deaths. [13]
More recent evidence introduces a theory that vitamin E supplements may have potential benefits only in certain subgroups of the general population. A trial of high-dose vitamin E in Israel, for example, showed a marked reduction in heart disease among people with type 2 diabetes who had a common genetic predisposition for greater oxidative stress. [14]
Taken as a whole, observational studies have not found that vitamin E in food or supplements offers much protection against cancer in general, or against specific cancers. [15–24] The U.S. Preventive Services Task Force’s latest review of the evidence from clinical trials on the efficacy of vitamin E for cancer also showed no benefit of these supplements on a decreased incidence of or deaths from any cancer. [2] Observational studies and clinical trials have been inconsistent, some suggesting that vitamin E supplements might lower the risk of advanced prostate cancer in smokers and a large randomized trial suggesting that vitamin E increases the risk of prostate cancer. [17,25–27]
Prostate cancer
Investigators had hoped that the Selenium and Vitamin E Cancer Prevention Trial (SELECT) would give more definitive answers on vitamin E and prostate cancer. SELECT’s 18,000 men were assigned to follow one of four pill regimens—vitamin E plus selenium, vitamin E plus a selenium placebo, selenium plus a vitamin E placebo, or a double placebo—and to be tracked for 7 to 12 years. But investigators halted the study halfway through in 2008 when early analyses showed that vitamin E offered no cancer or prostate cancer prevention benefit. [28] Though the trial ended, researchers continued to follow the men who had participated. In 2011, they reported a 17% higher risk of prostate cancer among men assigned to take vitamin E; there was no significant increased risk of prostate cancer among men who took vitamin E and selenium. [29]
Though these results may sound worrisome, two other major trials of vitamin E and prostate cancer had quite different results: The Alpha-Tocopherol Beta Carotene randomized trial, for example, followed nearly 30,000 Finnish male smokers for an average of six years. [25] It found that men assigned to take daily vitamin E supplements had a 32% lower risk of developing prostate cancer—and a 41% lower risk of dying from prostate cancer—than men given a placebo. Vitamin E’s protective effect was strongest for men whose cancers were far enough along that they could be detected by a clinical exam. The large and long-term Physicians’ Health Study II trial, meanwhile, found that vitamin E supplements did not increase or decrease the risk of prostate cancer or any other cancer. [30]
Why were the SELECT findings on vitamin E and prostate cancer so different from those of earlier studies? Previous studies of vitamin E supplements and prostate cancer found the greatest benefit in men who were smokers and who had more advanced cancers. [17,25–27] In the SELECT trial, however, fewer than 10% of the men were smokers and most had early-stage cancer detected through prostate specific antigen (PSA) blood tests. [28,29] Many early-stage, low-grade prostate cancers identified by PSA test would not become advanced cancers. There is also evidence that different processes may be at work in early versus late-stage prostate cancers. A large trial of a drug to prevent prostate cancer found opposite effects when used in early versus advanced prostate cancers. [31]
Bear in mind that most prostate cancer develops slowly, and any study looking at prostate cancer prevention needs to track men for a long time. By stopping the SELECT trial early, there is no way to tell if vitamin E could have helped protect against prostate cancer in some men if they had continued the trial over a longer period of time. Very few cases in the SELECT trial were of advanced prostate cancer, further limiting the interpretation of the findings.
A six-year trial found that vitamin E, in combination with vitamin C, beta carotene, and zinc, offered some protection against the development of advanced age-related macular degeneration (AMD), but not cataracts, in people who were at high risk of the disease. [32,33] On its own, however, vitamin E does not seem to offer much benefit against either AMD or cataracts. [34,35]
Scientists seeking to untangle the causes of Alzheimer’s, Parkinson’s, and other diseases of the brain and nervous system have focused on the role that free radical damage plays in these diseases’ development. [36] But to date, there is little evidence as to whether vitamin E can help protect against these diseases or that it offers any benefit to people who already have these diseases.
- Dementia: Some prospective studies suggest that vitamin E supplements, particularly in combination with vitamin C, may be associated with small improvements in cognitive function or lowered risk of Alzheimer’s disease and other forms of dementia, while other studies have failed to find any such benefit. [37–41] A three-year randomized controlled trial in people with mild cognitive impairment—often a precursor to Alzheimer’s disease—found that taking 2,000 IU of vitamin E daily failed to slow the progression to Alzheimer’s disease. [42] Keep in mind, however, that the progression from mild cognitive impairment to Alzheimer’s disease can take many years, and this study was fairly short, so it is probably not the last word on vitamin E and dementia.
- Parkinson’s Disease: Some, but not all, prospective studies suggest that getting higher intakes of vitamin E from diet—not from high-dose supplements—is associated with a reduced risk of Parkinson’s disease. [43–45] In people who already have Parkinson’s, high-dose vitamin E supplements do not slow the disease’s progression. [46] Why the difference between vitamin E from foods versus that from supplements? It is possible that foods rich in vitamin E, such as nuts or legumes, contain other nutrients that protect against Parkinson’s disease. More research is needed.
- Amyotrophic Lateral Sclerosis (ALS): One large prospective study that followed nearly 1 million people for up to 16 years found that people who regularly took vitamin E supplements had a lower risk of dying from ALS than people who never took vitamin E supplements. [47] More recently, a combined analysis of multiple studies with more than 1 million participants found that the longer people used vitamin E supplements, the lower their risk of ALS. [48] Clinical trials of vitamin E supplements in people who already have ALS have generally failed to show any benefit, however. [49] This may be a situation where vitamin E is beneficial for prevention, rather than treatment, but more research is needed.
Food Sources
Vitamin E is found in plant-based oils, nuts , seeds, fruits , and vegetables .
- Wheat germ oil
- Sunflower, safflower, and soybean oil
- Sunflower seeds
- Peanuts, peanut butter
- Beet greens, collard greens, spinach
- Red bell pepper
Signs of Deficiency
Because vitamin E is found in a variety of foods and supplements, a deficiency in the U.S. is rare. People who have digestive disorders or do not absorb fat properly (e.g., pancreatitis, cystic fibrosis, celiac disease) can develop a vitamin E deficiency. The following are common signs of a deficiency:
- Retinopathy (damage to the retina of the eyes that can impair vision)
- Peripheral neuropathy (damage to the peripheral nerves, usually in the hands or feet, causing weakness or pain)
- Ataxia (loss of control of body movements)
- Decreased immune function
There is no evidence of toxic effects from vitamin E found naturally in foods. Most adults who obtain more than the RDA of 22 IU daily are using multivitamins or separate vitamin E supplements that contain anywhere from 400-1000 IU daily. There have not been reports of harmful side effects of supplement use in healthy people. However, there is a risk of excess bleeding, particularly with doses greater than 1000 mg daily or if an individual is also using a blood thinning medication such as warfarin. For this reason, an upper limit for vitamin E has been set for adults 19 years and older of 1000 mg daily (1465 IU) of any form of tocopherol supplement. [1]
Did You Know?
Due to occasional reports of negative health effects of vitamin E supplements, scientists have debated whether these supplements could be harmful and even increase the risk of death.
Researchers have tried to answer this question by combining the results of multiple studies. In one such analysis, the authors gathered and re-analyzed data from 19 clinical trials of vitamin E, including the GISSI and HOPE studies [50]; they found a higher rate of death in trials where patients took more than 400 IU of supplements a day. While this meta-analysis drew headlines when it was released, there are limitations to the conclusions that can be drawn from it. Some of the findings were based on very small studies. In some of these trials, vitamin E was combined with high doses of beta-carotene, which itself has been related to excess mortality. Furthermore, many of the high-dose vitamin E trials included in the analysis included people who had advanced heart disease or Alzheimer’s disease. Other meta-analyses have come to different conclusions. So it is not clear that these findings would apply to healthy people. The Physicians’ Health Study II, for example, did not find any difference in death rates between the study participants who took vitamin E and those who took a placebo. [13]
Vitamins and Minerals
- Institute of Medicine. Dietary reference intakes for vitamin C, vitamin E, selenium, and carotenoids . Washington, D.C.: National Academies Press; 2000.
- U.S Preventive Services Task Force, Mangione CM, Barry MJ, Nicholson WK, Cabana M, Chelmow D, Coker TR, Davis EM, Donahue KE, Doubeni CA, Jaén CR, Kubik M, Li L, Ogedegbe G, Pbert L, Ruiz JM, Stevermer J, Wong JB. Vitamin, Mineral, and Multivitamin Supplementation to Prevent Cardiovascular Disease and Cancer: US Preventive Services Task Force Recommendation Statement. JAMA . 2022 Jun 21;327(23):2326-2333.
- Stampfer MJ, Hennekens CH, Manson JE, Colditz GA, Rosner B, Willett WC. Vitamin E consumption and the risk of coronary disease in women. N Engl J Med . 1993;328:1444-9.
- Rimm EB, Stampfer MJ, Ascherio A, Giovannucci E, Colditz GA, Willett WC. Vitamin E consumption and the risk of coronary heart disease in men. N Engl J Med . 1993;328:1450-6.
- Rimm EB, Stampfer MJ. Antioxidants for vascular disease. Med Clin North Am . 2000;84:239-49.
- Lee IM, Cook NR, Gaziano JM, et al. Vitamin E in the primary prevention of cardiovascular disease and cancer: the Women’s Health Study: a randomized controlled trial. JAMA . 2005;294:56-65.
- Glynn RJ, Ridker PM, Goldhaber SZ, Zee RY, Buring JE. Effects of random allocation to vitamin E supplementation on the occurrence of venous thromboembolism: report from the Women’s Health Study. Circulation . 2007;116:1497-503.
- Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzione trial. Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico. Lancet . 1999;354:447-55.
- Yusuf S, Dagenais G, Pogue J, Bosch J, Sleight P. Vitamin E supplementation and cardiovascular events in high-risk patients. The Heart Outcomes Prevention Evaluation Study Investigators. N Engl J Med . 2000;342:154-60.
- Lonn E, Bosch J, Yusuf S, et al. Effects of long-term vitamin E supplementation on cardiovascular events and cancer: a randomized controlled trial. JAMA . 2005;293:1338-47.
- Kris-Etherton PM, Lichtenstein AH, Howard BV, Steinberg D, Witztum JL. Antioxidant vitamin supplements and cardiovascular disease. Circulation . 2004;110:637-41.
- Hercberg S, Galan P, Preziosi P, et al. The SU.VI.MAX Study: a randomized, placebo-controlled trial of the health effects of antioxidant vitamins and minerals. Arch Intern Med . 2004;164:2335-42.
- Sesso HD, Buring JE, Christen WG, et al. Vitamins E and C in the prevention of cardiovascular disease in men: the Physicians’ Health Study II randomized controlled trial. JAMA . 2008;300:2123-33.
- Milman U, Blum S, Shapira C, et al. Vitamin E supplementation reduces cardiovascular events in a subgroup of middle-aged individuals with both type 2 diabetes mellitus and the haptoglobin 2-2 genotype: a prospective double-blinded clinical trial. Arterioscler Thromb Vasc Biol . 2008;28:341-7.
- Hunter DJ, Manson JE, Colditz GA, et al. A prospective study of the intake of vitamins C, E, and A and the risk of breast cancer. N Engl J Med . 1993;329:234-40.
- Willett WC, Polk BF, Underwood BA, et al. Relation of serum vitamins A and E and carotenoids to the risk of cancer. N Engl J Med . 1984;310:430-4.
- Chan JM, Stampfer MJ, Ma J, Rimm EB, Willett WC, Giovannucci EL. Supplemental vitamin E intake and prostate cancer risk in a large cohort of men in the United States. Cancer Epidemiol Biomarkers Prev . 1999;8:893-9.
- van Dam RM, Huang Z, Giovannucci E, et al. Diet and basal cell carcinoma of the skin in a prospective cohort of men. Am J Clin Nutr . 2000;71:135-41.
- Wu K, Willett WC, Chan JM, et al. A prospective study on supplemental vitamin e intake and risk of colon cancer in women and men. Cancer Epidemiol Biomarkers Prev . 2002;11:1298-304.
- Fung TT, Spiegelman D, Egan KM, Giovannucci E, Hunter DJ, Willett WC. Vitamin and carotenoid intake and risk of squamous cell carcinoma of the skin. Int J Cancer . 2003;103:110-5.
- Feskanich D, Willett WC, Hunter DJ, Colditz GA. Dietary intakes of vitamins A, C, and E and risk of melanoma in two cohorts of women. Br J Cancer . 2003;88:1381-7.
- Cho E, Spiegelman D, Hunter DJ, et al. Premenopausal intakes of vitamins A, C, and E, folate, and carotenoids, and risk of breast cancer. Cancer Epidemiol Biomarkers Prev . 2003;12:713-20.
- Cho E, Hunter DJ, Spiegelman D, et al. Intakes of vitamins A, C and E and folate and multivitamins and lung cancer: a pooled analysis of 8 prospective studies. Int J Cancer . 2006;118:970-8.
- Lee JE, Giovannucci E, Smith-Warner SA, Spiegelman D, Willett WC, Curhan GC. Intakes of fruits, vegetables, vitamins A, C, and E, and carotenoids and risk of renal cell cancer. Cancer Epidemiol Biomarkers Prev . 2006;15:2445-52.
- Heinonen OP, Albanes D, Virtamo J, et al. Prostate cancer and supplementation with alpha-tocopherol and beta-carotene: incidence and mortality in a controlled trial. J Natl Cancer Inst . 1998;90:440-6.
- Kirsh VA, Hayes RB, Mayne ST, et al. Supplemental and dietary vitamin E, beta-carotene, and vitamin C intakes and prostate cancer risk. J Natl Cancer Inst . 2006;98:245-54.
- Peters U, Littman AJ, Kristal AR, Patterson RE, Potter JD, White E. Vitamin E and selenium supplementation and risk of prostate cancer in the Vitamins and Lifestyle (VITAL) study cohort. Cancer Causes Control . 2008;19:75-87.
- Lippman SM, Klein EA, Goodman PJ, et al. Effect of selenium and vitamin E on risk of prostate cancer and other cancers: the Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA . 2009;301:39-51.
- Klein EA, Thompson IM, Jr., Tangen CM, et al. Vitamin E and the risk of prostate cancer: the Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA . 2011;306:1549-56.
- Wang L, Sesso HD, Glynn RJ, Christen WG, Bubes V, Manson JE, Buring JE, Gaziano JM. Vitamin E and C supplementation and risk of cancer in men: posttrial follow-up in the Physicians’ Health Study II randomized trial. The American journal of clinical nutrition . 2014 Sep 1;100(3):915-23.
- Thompson IM, Goodman PJ, Tangen CM, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med . 2003;349:215-24.
- A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol . 2001;119:1417-36.
- Age Related Eye Disease Study 2 (AREDS2). National Eye Institute, 2007. Accessed 8 November 2007,
- Chong EW, Wong TY, Kreis AJ, Simpson JA, Guymer RH. Dietary antioxidants and primary prevention of age related macular degeneration: systematic review and meta-analysis. BMJ . 2007;335:755.
- Christen WG, Glynn RJ, Chew EY, Buring JE. Vitamin E and age-related macular degeneration in a randomized trial of women. Ophthalmology . 2010;117:1163-8.
- Kamat CD, Gadal S, Mhatre M, Williamson KS, Pye QN, Hensley K. Antioxidants in central nervous system diseases: preclinical promise and translational challenges. J Alzheimers Dis . 2008;15:473-93.
- Grodstein F, Chen J, Willett WC. High-dose antioxidant supplements and cognitive function in community-dwelling elderly women. Am J Clin Nutr . 2003;77:975-84.
- Zandi PP, Anthony JC, Khachaturian AS, et al. Reduced risk of Alzheimer disease in users of antioxidant vitamin supplements: the Cache County Study. Arch Neurol . 2004;61:82-8.
- Laurin D, Masaki KH, Foley DJ, White LR, Launer LJ. Midlife dietary intake of antioxidants and risk of late-life incident dementia: the Honolulu-Asia Aging Study. Am J Epidemiol . 2004;159:959-67.
- Gray SL, Anderson ML, Crane PK, et al. Antioxidant vitamin supplement use and risk of dementia or Alzheimer’s disease in older adults. J Am Geriatr Soc . 2008;56:291-5.
- Devore EE, Kang JH, Stampfer MJ, Grodstein F. The association of antioxidants and cognition in the Nurses’ Health Study. American journal of epidemiology . 2013 Jan 1;177(1):33-41.
- Petersen RC, Thomas RG, Grundman M, et al. Vitamin E and donepezil for the treatment of mild cognitive impairment. N Engl J Med . 2005;352:2379-88.
- Zhang SM, Hernan MA, Chen H, Spiegelman D, Willett WC, Ascherio A. Intakes of vitamins E and C, carotenoids, vitamin supplements, and PD risk. Neurology . 2002;59:1161-9.
- Etminan M, Gill SS, Samii A. Intake of vitamin E, vitamin C, and carotenoids and the risk of Parkinson’s disease: a meta-analysis. Lancet Neurol . 2005;4:362-5.
- Morens DM, Grandinetti A, Waslien CI, Park CB, Ross GW, White LR. Case-control study of idiopathic Parkinson’s disease and dietary vitamin E intake. Neurology . 1996;46:1270-4.
- Effects of tocopherol and deprenyl on the progression of disability in early Parkinson’s disease. The Parkinson Study Group. N Engl J Med . 1993;328:176-83.
- Ascherio A, Weisskopf MG, O’Reilly E J, et al. Vitamin E intake and risk of amyotrophic lateral sclerosis. Ann Neurol . 2005;57:104-10.
- Wang H, O’Reilly EJ, Weisskopf MG, et al. Vitamin E intake and risk of amyotrophic lateral sclerosis: a pooled analysis of data from 5 prospective cohort studies. Am J Epidemiol . 2011;173:595-602.
- Orrell RW, Lane RJ, Ross M. Antioxidant treatment for amyotrophic lateral sclerosis / motor neuron disease. Cochrane Database Syst Rev . 2007:CD002829.
- Miller ER, 3rd, Pastor-Barriuso R, Dalal D, Riemersma RA, Appel LJ, Guallar E. Meta-analysis: high-dosage vitamin E supplementation may increase all-cause mortality. Ann Intern Med . 2005;142:37-46.
Last reviewed March 2023
Terms of Use
The contents of this website are for educational purposes and are not intended to offer personal medical advice. You should seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website. The Nutrition Source does not recommend or endorse any products.
Learn how UpToDate can help you.
Select the option that best describes you
- Medical Professional
- Resident, Fellow, or Student
- Hospital or Institution
- Group Practice
- Patient or Caregiver
- Find in topic
RELATED TOPICS
INTRODUCTION
In 1922, Evans and Bishop discovered that rats fed a lard-based diet developed infertility, suggesting a dietary deficiency [ 1 ]. The fertility was corrected when a lipid extract of cereals was added to the diet; this was termed the "anti-sterility factor" [ 2 ]. In 1925, vitamin E was officially recognized as the fifth vitamin. A few years later, the name tocopherol, from the Greek word of "toc" (child) and "phero" (to bring forth), was coined to describe its role as an essential dietary substance in normal fetal and childhood development [ 3 ]. In 1969, the US Food and Drug Administration (FDA) formally recognized vitamin E as an essential nutrient for humans.
This topic review will focus on vitamin E. Overviews of the other fat-soluble vitamins, minerals, and water-soluble vitamins are available elsewhere. (See "Overview of vitamin A" and "Overview of vitamin D" and "Overview of vitamin K" and "Overview of dietary trace elements" and "Overview of water-soluble vitamins" and "Vitamin intake and disease prevention" .)
Vitamin E is also available in supplements, either alone or as part of a multivitamin supplement.
Appointments at Mayo Clinic
Vitamin E is a nutrient that's important to vision, reproduction, and the health of your blood, brain and skin.
Vitamin E also has antioxidant properties. Antioxidants are substances that might protect your cells against the effects of free radicals — molecules produced when your body breaks down food or is exposed to tobacco smoke and radiation. Free radicals might play a role in heart disease, cancer and other diseases. If you take vitamin E for its antioxidant properties, keep in mind that the supplement might not offer the same benefits as naturally occurring antioxidants in food.
Foods rich in vitamin E include canola oil, olive oil, margarine, almonds and peanuts. You can also get vitamin E from meats, dairy, leafy greens and fortified cereals. Vitamin E is also available as an oral supplement in capsules or drops.
Vitamin E deficiency can cause nerve pain (neuropathy).
The recommended daily amount of vitamin E for adults is 15 milligrams a day.
What the research says
Research on vitamin E use for specific conditions shows:
- Alzheimer's disease. Some research has shown that high-dose vitamin E might delay the progression of Alzheimer's disease in people who have been diagnosed with mild to moderate Alzheimer's disease. Other studies haven't shown this benefit. Vitamin E supplements appear to have no effect on whether people with mild cognitive impairment progress to Alzheimer's disease.
- Liver disease. Studies show that vitamin E might improve symptoms of nonalcoholic fatty liver disease. However, some evidence suggests that taking oral vitamin E for this purpose for two years is linked to insulin resistance.
- Preeclampsia. Increasing your intake of vitamin E hasn't been shown to prevent this pregnancy condition that affects blood pressure.
- Prostate cancer. Research shows that vitamin E and selenium supplements don't prevent prostate cancer. There is also concern that use of vitamin E supplements might increase the risk of prostate cancer.
Most people get enough vitamin E from a balanced diet. If you've been diagnosed with mild to moderate Alzheimer's disease, some research suggests that vitamin E therapy might help slow disease progression.
However, oral use of vitamin E might increase the risk of prostate cancer. Use of the supplement can pose other serious risks, particularly at high doses and if you have other health conditions or have had a heart attack or stroke.
Safety and side effects
When taken at appropriate doses, oral use of vitamin E is generally considered safe. Rarely, oral use of vitamin E can cause:
- Intestinal cramps
- Blurred vision
- Gonadal dysfunction
- Increased concentration of creatine in the urine (creatinuria)
Taking higher doses of vitamin E might increase the risk of side effects. Also, there is concern that people in poor health who take high doses of vitamin E are at increased risk of death.
Use of vitamin E can interact with many conditions. For example, research suggests that oral use of vitamin E might increase the risk of prostate cancer. Other research suggests that vitamin E use might increase the risk of death in people with a severe history of heart disease, such as heart attack or stroke. Talk with your doctor before taking vitamin E if you have:
- A vitamin K deficiency
- An eye condition in which the retina is damaged (retinitis pigmentosa)
- Bleeding disorders
- A history of a previous heart attack or stroke
- Head and neck cancer
- Liver disease
The supplement might increase your risk of bleeding. If you're planning to have surgery, stop taking vitamin E two weeks beforehand. Also, talk to your doctor about vitamin E use if you're about to have or you just had a procedure to open blocked arteries and restore normal blood flow to your heart muscle (angioplasty).
Interactions
Use of some drugs can affect your vitamin E levels. Possible interactions include:
- Alkylating agents and anti-tumor antibiotics. There's concern that high doses of vitamin E might affect the use of these chemotherapy drugs.
- Anticoagulants and anti-platelet drugs, herbs and supplements. Use of vitamin E with these drugs, herbs and supplements to reduce blood clotting might increase the risk of bleeding.
- Cytochrome P450 3A4 (CYP3A4) substrates. Use caution when taking vitamin E and other drugs affected by these enzymes, such as omeprazole (Prilosec, Zegerid).
- Statins and niacin. Taking vitamin E with statins or niacin, which might benefit people with high cholesterol, could reduce niacin's effect.
- Vitamin K. Taking vitamin E with vitamin K might decrease the effects of vitamin K.
There is a problem with information submitted for this request. Review/update the information highlighted below and resubmit the form.
From Mayo Clinic to your inbox
Sign up for free and stay up to date on research advancements, health tips, current health topics, and expertise on managing health. Click here for an email preview.
Error Email field is required
Error Include a valid email address
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
Thank you for subscribing!
You'll soon start receiving the latest Mayo Clinic health information you requested in your inbox.
Sorry something went wrong with your subscription
Please, try again in a couple of minutes
- Vitamin E oral. Facts & Comparisons eAnswers. http://www.wolterskluwercdi.com/facts-comparisons-online/. Accessed Aug. 10, 2017.
- Vitamin E. Micromedex 2.0 Healthcare Series. http://www.micromedexsolutions.com. Accessed Aug. 10, 2017.
- Vitamin E. Natural Medicines. https://naturalmedicines.therapeuticresearch.com. Accessed Sept. 27, 2017.
- Antioxidants. AskMayoExpert. Rochester, Minn.: Mayo Foundation for Medical Education and Research; 2017.
- Press D, et al. Prevention of dementia. https://www.uptodate.com/contents/search. Accessed Aug. 15, 2017.
- Sexton DJ, et al. The common cold in adults: Treatment and prevention. https://www.uptodate.com/content/search. Accessed Aug. 8, 2017.
- Press D, et al. Treatment of dementia. https://www.uptodate.com/contents/search. Accessed Aug. 17, 2017.
- Vitamin and mineral supplements. American Heart Association. http://www.heart.org/HEARTORG/HealthyLiving/HealthyEating/Vitamin-and-Mineral-Supplements_UCM_306033_Article.jsp#.WDpy-X0mGLU. Accessed Aug. 17, 2017.
Mayo Clinic does not endorse companies or products. Advertising revenue supports our not-for-profit mission.
- Opportunities
Mayo Clinic Press
Check out these best-sellers and special offers on books and newsletters from Mayo Clinic Press .
- Mayo Clinic on Incontinence - Mayo Clinic Press Mayo Clinic on Incontinence
- The Essential Diabetes Book - Mayo Clinic Press The Essential Diabetes Book
- Mayo Clinic on Hearing and Balance - Mayo Clinic Press Mayo Clinic on Hearing and Balance
- FREE Mayo Clinic Diet Assessment - Mayo Clinic Press FREE Mayo Clinic Diet Assessment
- Mayo Clinic Health Letter - FREE book - Mayo Clinic Press Mayo Clinic Health Letter - FREE book
Your gift holds great power – donate today!
Make your tax-deductible gift and be a part of the cutting-edge research and care that's changing medicine.

- U.S. Department of Health & Human Services HHS
- National Institutes of Health NIH
- Division of Program Coordination, Planning, and Strategic Initiatives DPCPSI

This is a general overview. For more in-depth information, see our health professional fact sheet .
What is vitamin E and what does it do?
Vitamin E is a fat-soluble nutrient found in many foods. In the body, it acts as an antioxidant , helping to protect cells from the damage caused by free radicals . Free radicals are compounds formed when our bodies convert the food we eat into energy. People are also exposed to free radicals in the environment from cigarette smoke, air pollution, and ultraviolet light from the sun.
The body also needs vitamin E to boost its immune system so that it can fight off invading bacteria and viruses . It helps to widen blood vessels and keep blood from clotting within them. In addition, cells use vitamin E to interact with each other and to carry out many important functions.
How much vitamin E do I need?
The amount of vitamin E you need each day depends on your age. Average daily recommended amounts are listed below in milligrams (mg).
What foods provide vitamin E?
Vitamin E is found naturally in foods and is added to some fortified foods. You can get recommended amounts of vitamin E by eating a variety of foods including the following:
- Vegetable oils like wheat germ, sunflower, and safflower oils are among the best sources of vitamin E. Corn and soybean oils also provide some vitamin E.
- Nuts (such as peanuts, hazelnuts, and, especially, almonds) and seeds (like sunflower seeds) are also among the best sources of vitamin E.
- Green vegetables, such as spinach and broccoli, provide some vitamin E.
- Food companies add vitamin E to some breakfast cereals, fruit juices, margarines and spreads, and other foods. To find out which ones have vitamin E, check the product labels .
What kinds of vitamin E dietary supplements are available?
Vitamin E supplements come in different amounts and forms. Two main things to consider when choosing a vitamin E supplement are:
- The amount of vitamin E: Most once-daily multivitamin/mineral supplements provide about 13.5 mg of vitamin E, whereas vitamin E-only supplements commonly contain 67 mg or more. The doses in most vitamin E-only supplements are much higher than the recommended amounts. Some people take large doses because they believe or hope that doing so will keep them healthy or lower their risk of certain diseases.
- The form of vitamin E: Although vitamin E sounds like a single substance, it is actually the name of eight related compounds in food, including alpha-tocopherol . Each form has a different potency, or level of activity in the body.
Vitamin E from natural sources is commonly listed as d -alpha-tocopherol on food packaging and supplement labels. Synthetic (laboratory-made) vitamin E is commonly listed as dl -alpha-tocopherol. The natural form is more potent; 1 mg vitamin E = 1 mg d -alpha-tocopherol (natural vitamin E) = 2 mg dl -alpha-tocopherol (synthetic vitamin E).
Some food and dietary supplement labels still list vitamin E in International Units ( IUs ) rather than mg. One IU of the natural form of vitamin E is equivalent to 0.67 mg. One IU of the synthetic form of vitamin E is equivalent to 0.45 mg.
Some vitamin E supplements provide other forms of the vitamin, such as gamma-tocopherol, tocotrienols, and mixed tocopherols. Scientists do not know if any of these forms are superior to alpha-tocopherol in supplements.
Am I getting enough vitamin E?
The diets of most Americans provide less than the recommended amounts of vitamin E. Nevertheless, healthy people rarely show any clear signs that they are not getting enough vitamin E (see next question for information on the signs of vitamin E deficiency ).
What happens if I don't get enough vitamin E?
Vitamin E deficiency is very rare in healthy people. It is almost always linked to certain diseases in which fat is not properly digested or absorbed . Examples include Crohn's disease , cystic fibrosis , and certain rare genetic diseases such as abetalipoproteinemia and ataxia with vitamin E deficiency (AVED). Vitamin E needs some fat for the digestive system to absorb it.
Vitamin E deficiency can cause nerve and muscle damage that results in loss of feeling in the arms and legs, loss of body movement control , muscle weakness, and vision problems. Another sign of deficiency is a weakened immune system.
What are some effects of vitamin E on health?
Scientists are studying vitamin E to understand how it affects health. Here are several examples of what this research has shown.
Heart disease
Some studies link higher intakes of vitamin E from supplements to lower chances of developing coronary heart disease . However, the best research finds no benefit. People in these studies are randomly assigned to take vitamin E or a placebo (dummy pill with no vitamin E or active ingredients ) and they don't know which they are taking. Vitamin E supplements do not seem to prevent heart disease, reduce its severity, or affect the risk of death from this disease. Scientists do not know whether high intakes of vitamin E might protect the heart in younger, healthier people who do not have a high risk of heart disease.
Most research indicates that vitamin E does not help prevent cancer and may be harmful in some cases. Large doses of vitamin E have not consistently reduced the risk of colon and breast cancer in studies, for example. A large study found that taking vitamin E supplements (180 mg/day [400 IU]) for several years increased the risk of developing prostate cancer in men. Two studies that followed middle-age men and women for 7 or more years found that extra vitamin E (201−268 mg/day [300–400 IU], on average) did not protect them from any form of cancer. However, one study found a link between the use of vitamin E supplements for 10 years or more and a lower risk of death from bladder cancer .
Vitamin E dietary supplements and other antioxidants might interact with chemotherapy and radiation therapy . People undergoing these treatments should talk with their doctor or oncologist before taking vitamin E or other antioxidant supplements, especially in high doses.
Eye disorders
Age-related macular degeneration (AMD), or the loss of central vision in older people, and cataracts are among the most common causes of vision loss in older people. The results of research on whether vitamin E can help prevent these conditions are inconsistent. Among people with AMD who were at high risk of developing advanced AMD, a supplement containing large doses of vitamin E combined with other antioxidants, zinc , and copper showed promise for slowing down the rate of vision loss.
Mental function
Several studies have investigated whether vitamin E supplements might help older adults remain mentally alert and active as well as prevent or slow the decline of mental function and Alzheimer's disease . So far, the research provides little evidence that taking vitamin E supplements can help healthy people or people with mild mental functioning problems to maintain brain health.
Can vitamin E be harmful?
Vitamin E that is naturally present in food and beverages is not harmful and does not need to be limited.
In supplement form, however, high doses of vitamin E might increase the risk of bleeding (by reducing the blood's ability to form clots after a cut or injury) and of serious bleeding in the brain (known as hemorrhagic stroke ). Because of this risk, the upper limit for adults is 1,000 mg/day for supplements of either natural or synthetic vitamin E. This is equal to 1,500 IU/day for natural vitamin E supplements and 1,100 IU/day for synthetic vitamin E supplements. The upper limits for children are lower than those for adults. Some research suggests that taking vitamin E supplements even below these upper limits might cause harm. In one study, for example, men who took 400 IU (180 mg) of synthetic vitamin E each day for several years had an increased risk of prostate cancer.
Does vitamin E interact with medications or other dietary supplements?
Vitamin E dietary supplements can interact or interfere with certain medicines that you take. Here are some examples:
- Vitamin E can increase the risk of bleeding in people taking anticoagulant or antiplatelet medicines, such as warfarin (Coumadin).
- In one study, vitamin E plus other antioxidants (such as vitamin C , selenium , and beta-carotene ) reduced the heart-protective effects of two drugs taken in combination (a statin and niacin ) to affect blood cholesterol levels.
- Taking antioxidant supplements while undergoing chemotherapy or radiation therapy for cancer could alter the effectiveness of these treatments.
Tell your doctor, pharmacist , and other health care providers about any dietary supplements and medicines you take. They can tell you if those dietary supplements might interact or interfere with your prescription or over-the-counter medicines, or if the medicines might interfere with how your body absorbs, uses, or breaks down nutrients.
Vitamin E and healthful eating
Where can I find out more about vitamin E?
- Office of Dietary Supplements (ODS) Health Professional Fact Sheet on Vitamin E
- Nutrient List for vitamin E (listed by food or by vitamin E content ), USDA
- ODS Frequently Asked Questions: Which brand(s) of dietary supplements should I purchase?
This fact sheet by the National Institutes of Health (NIH) Office of Dietary Supplements (ODS) provides information that should not take the place of medical advice. We encourage you to talk to your health care providers (doctor, registered dietitian, pharmacist, etc.) about your interest in, questions about, or use of dietary supplements and what may be best for your overall health. Any mention in this publication of a specific product or service, or recommendation from an organization or professional society, does not represent an endorsement by ODS of that product, service, or expert advice.
Updated: March 22, 2021 History of changes to this fact sheet
- Weight Management
- Nutrition Facts
- Nutrition Basics
- Meal Delivery Services
- Fitness Gear
- Apparel & Accessories
- Recipe Nutrition Calculator
- Weight Loss Calorie Goal
- BMI Calculator
- Body Fat Percentage Calculator
- Calories Burned by Activity
- Daily Calories Burned
- Pace Calculator
- Editorial Process
- Meet Our Review Board
The Health Benefits of Vitamin E
Supplements may prevent or treat certain age-related diseases
Melissa Rifkin is a Connecticut-based registered dietitian with over 15 years of experience working in the clinical setting.
:max_bytes(150000):strip_icc():format(webp)/unnamed-38aa6879f8b546c3a3ba36ec48bda560.jpeg "presentation of vitamin e")
Cara Lustik is a fact-checker and copywriter with more than 15 years of experience crafting stories in the branding, licensing, and entertainment industries.
:max_bytes(150000):strip_icc():format(webp)/Cara-Lustik-1000-8eb5718d7cd34f8797e1ffa65d7f3e7a.jpg "presentation of vitamin e")
Vitamin E Benefits
Possible side effects, dosage and preparation, what to look for, other questions.
Fat-soluble vitamins, including vitamin E, must be consumed with dietary fat to be efficiently transported and used throughout the body. Mother Nature has made this easy as vitamin E is naturally found in many foods containing fat like vegetable oils, eggs, meat, poultry, and nuts. Vitamin E is also found in broccoli, spinach, kiwifruit, mango, and tomato.
After vitamin E is absorbed in the small intestine, it's taken up by the liver, where it's stored until it's needed for use. At that point, the liver only resecretes alpha-tocopherol, the form that is recognized by the body.
Vitamin E benefits your immune system and contributes to eye, brain, and skin health. Though vitamin E deficiency is rare, meeting daily vitamin E requirements is important to maintain health and prevent and treat disease.
There are a few situations where vitamin E deficiency is possible. One is in premature babies with low birth weight. It is also possible in people with a fat-malabsorption disorder, like Crohn's disease and cystic fibrosis, where the body has a hard time or does not properly absorb dietary fat. Both require supplementation to reduce the risk of complications.
Vitamin E, or alpha-tocopherol, is a fat-soluble vitamin that acts as a powerful antioxidant to protect cells from free radical damage and is involved in immune function. It's an essential vitamin and must be found in your diet . Vitamin E is important for your brain, eyes, immune system , and heart health. The nutrient may prevent heart disease and eye disorders, improve cognitive function , and even protect against some cancers. However, the research supporting these claims is varied. You can read more about the benefits of vitamin E below.
May Prevent Coronary Heart Disease
Whether vitamin E prevents coronary heart disease (CVD) in the general population has yet to be determined. Much of the existing research contradicts findings suggesting vitamin E supplementation in high-risk patients is beneficial. In contrast, other research indicates that vitamin E does not improve cardiovascular risk factors.
According to a review published in the Journal of Lipid Research , administering vitamin E supplementation may be cardioprotective for those with high levels of oxidative stress, including those with type 2 diabetes and those undergoing hemodialysis.
Interestingly, a 2019 study determined quite the opposite: supplementing with vitamin E had adverse effects on coronary artery disease (CAD). Scientists found that higher vitamin E levels may increase the CAD risk.
At this time, more research is needed to determine the effects of vitamin E on cardiovascular risk factors. Talk with your cardiologist before taking vitamin E to improve heart health .
Finally, the American Heart Association does not promote the usage of vitamin E supplementation to prevent cardiovascular disease as it may be associated with an increase in total mortality, heart failure, and hemorrhagic stroke. However, they suggest eating foods rich in vitamin E and other antioxidant nutrients to promote heart health.
Could Reduce Risk of Developing Certain Cancers
Another controversial benefit of vitamin E is its effect on cancer. Vitamin E is a powerful antioxidant that prevents and fights free radical oxidation and damage to cells which may play a role in developing cancer and other health conditions.
Research on whether or not vitamin E prevents or promotes cancer is still emerging and is specific to the form of vitamin E and its bioavailability. Evidence suggests that lower vitamin E intake is associated with increased cancer risk.
Other reviews have examined the type of vitamin E (tocopherols and tocotrienols) on cancer risk. They have found that a gamma-tocopherol-rich mixture of vitamin E tocopherols is a promising anti-cancer agent and should be studied further.
On the other hand, some evidence does not support the supplementation of vitamin E for cancer prevention. One study examined the effect of vitamin E supplementation on the risk of prostate cancer and showed that vitamin E is not a good prevention method for cancer. This study also determined that vitamin E may increase the risk of prostate cancer.
More research is needed to determine whether vitamin E can help prevent cancer.
May Prevent or Treat Eye Disorders
Macular degeneration (AMD) and cataracts are the most common age-related eye diseases associated with oxidative stress and free radical damage. Vitamin E's antioxidant activity makes it an ideal candidate for preventing and treating both AMD and cataracts.
One review investigated the benefits of antioxidant micronutrients on eye health and macular degeneration. It found that vitamin E helps reduce the cellular oxidative stress of the retina or macular region of the eye. Additional studies have found a correlation between increased dietary vitamin E and AMD's slower progression rate.
In addition, vitamin E aids in the self-repair of the retina, cornea, and uvea (the pigmented portion of the eye). A 2015 review of studies published in Public Health Nutrition concluded that vitamin E supplementation was associated with a reduced risk of aging-related cataracts.
Though the evidence is promising for vitamin E and the prevention of age-related eye disorders, more research is needed.
May Prevent or Delay Cognitive Decline
Cognitive health refers to how well you think, learn, and remember things. A balanced, nutritious diet is at the forefront of maintaining good cognitive health and preventing age-related cognitive deterioration, including dementia and Alzheimer's.
It's been postulated that foods rich in antioxidant vitamins would slow the onset of Alzheimer's disease. However, the research is not clear on whether supplementing with antioxidant vitamins, including vitamin E, is only beneficial for those with antioxidant vitamin deficiencies.
However, one study did see a slight decline in the incidence of Alzheimer's disease when supplementing with vitamin E.
Another study hypothesized that supplementation with vitamin E in patients with Alzheimer's disease could protect against oxidative damage, reduce neuronal damage, and slow the progression of Alzheimer's disease. After two years of supplementing with 2000 IUs per day of vitamin E, researchers found that they were able to slow the progression of the disease.
A similar study over three years found that vitamin E had no benefit in patients with mild cognitive impairment. And the rate of progression of Alzheimer's disease did not change.
More research is needed to determine whether supplementing with vitamin E will slow the onset or progression of age-related cognitive decline. However, those with a deficiency would benefit from supplementing with alpha-tocopherol vitamin E.
Protects the Skin
Vitamin E has been used for decades in dermatology as a shield to protect the skin from UV-induced free radical damage, which is why it is often added to some of our favorite sunscreens . When taken orally, vitamin E helps reduce the time it takes for wounds to heal.
Topically vitamin E is known for its anti-inflammatory properties, which is why it can often be found in pain relief creams . It is also used to promote collagen production. Vitamin E oil can also be used to remove waterproof makeup .
Unfortunately, existing research is varied and inconclusive. While it sounds great, expecting vitamin E to clear skin conditions beyond reducing healing time could be a waste of money. A quality skincare routine and a discussion with a dermatologist is the best way to combat skin disorders.
Large Doses of Vitamin E
Vitamin E supplements rarely cause any harm if taken at the recommended daily dose. And research has not found any adverse effects from vitamin E in food.
However, taking vitamin E in doses greater than the RDA of 300 IUs daily puts you at a greater risk of hemorrhagic stroke. One study cautions against the use of vitamin E supplementation as it found vitamin E increased the risk of hemorrhagic stroke by 22%.
Even doses lower than this can trigger side effects like nausea, vomiting, stomach pain, and diarrhea.
Interactions with Medications
Vitamin E prevents platelet aggregation, meaning it slows blood clotting. Talk to a healthcare professional before taking vitamin E if you take blood thinners, including Coumadin (warfarin) or Plavix (clopidogrel), especially if you have low vitamin K intake.
Additionally, avoid taking vitamin E at least two weeks before surgery to prevent excessive bleeding.
Vitamin E may also interact with certain medications, including the immune-suppressive drug Sandimmune (cyclosporine), certain chemotherapy drugs, statin drugs like Lipitor (atorvastatin), and tamoxifen.
Use During Pregnancy or Breastfeeding
Vitamin E is generally found to be safe for pregnant or breastfeeding people. Always speak with a health care provider before taking any new supplements or medications.
The recommended dietary allowance (RDA) for vitamin E is 15 mg. Most vitamin E supplements provide around 67 mg of the nutrient, which is much greater than the RDA. Those requiring a vitamin E supplement likely have a diagnosed vitamin E deficiency, which is much more appropriate for the 60 to 75 mg daily dosage provided in a supplement. Large dosage vitamin E supplements should be approached with caution and discussed with your doctor in advance.
Vitamin E supplements are available in two forms: synthetic and natural. The natural form of vitamin E is alpha-tocopherol, while the synthetic form is DI-alpha-tocopherol. Both work well; however, a larger dose of the synthetic form is required to achieve similar results. You can also find vitamin E supplements containing both forms of alpha-tocopherol, called mixed tocopherols .
It can be confusing to determine if a product contains the dosing you need in a vitamin E supplement. Use these simple formulas to ensure you remain within the RDA of vitamin E:
Vitamin E Dosing Formulas
- To calculate the milligram dose of D-alpha-tocopherol , multiply the IUs by 0.67. Based on this formula, 25 IUs equal 16.75 mg.
- To calculate the milligram dose of Dl-alpha-tocopherol , multiply the IUs by 0.43. Based on this formula, 50 IUs equal 21.5 mg.
Supplement manufacturers are not required to put their products through vigorous testing and research. Because of this, there's no way to be sure the label represents what is actually in the bottle.
To find products you can trust, opt for brands that voluntarily put their products through independent third-party testing by a certifying body like the U.S. Pharmacopeia (USP), ConsumerLab, or NSF International.
Vitamin E is sensitive to heat and can quickly degrade if exposed to extreme heat or direct sunlight. Always store vitamin E in the original container in a cool, dry room. Remember to discard any gel caps that have reached their use-by or expiration date, are discolored, or have evidence of leakage.
Topical vitamin E oil is available in drugstores and health food markets. It's intended for external use only.
Which foods are highest in vitamin E?
Vitamin E is found naturally in a variety of foods. The best food sources of vitamin E include nuts, seeds, vegetable oils, leafy green vegetables, and fortified cereals.
Vitamin E-Rich Foods
- Wheat germ oil : 21.8 mg per tablespoon (or 135% of your daily value)
- Sunflower seeds : 7.4 mg per one-ounce serving (or 49% of your daily value)
- Almonds : 7.4 mg per one-ounce serving (or 49% of your daily value)
- Avocados : 4.2 mg per avocado (or 28% of your daily value)
- Trout: 4 mg per average trout (or 26% of your daily value)
- Spinach : 3.7 mg per one-cup serving (or 25% of your daily value)
- Butternut squash : 2.6 mg per one-cup serving (or 18% of your daily value)
- Kiwi fruit : 2.6 mg per one-cup serving (or 18% of your daily value)
- Broccoli : 2.3 mg per one-cup serving (or 15% of your daily value)
- Olive oil : 1.9 mg per tablespoon (or 13% of your daily value)
- Shrimp : 1.9 mg per 3-ounce serving (or 13% of your daily value)
Can vitamin E cause weight gain?
Various studies investigating the effect of vitamin E intake on weight have produced mixed results. However, a 2021 meta-analysis of 24 studies show that vitamin E does not significantly impact weight in people with normal BMI.
Should I take vitamin E in the morning or at night?
If you choose to take a vitamin E supplement, there is some evidence that taking vitamin E in the evening reduces mortality from cardiovascular disease. Since vitamin E is a fat-soluble vitamin, it is probably more important to take it with some fat so that it is absorbed well by your body.
National Institutes of Health Office of Dietary Supplements. Vitamin E Fact Sheet for Health Professionals .
Heart Outcomes Prevention Evaluation Study Investigators, Yusuf S, Dagenais G, Pogue J, Bosch J, Sleight P. Vitamin E supplementation and cardiovascular events in high-risk patients . N Engl J Med . 2000 Jan 20;342(3):154-60. doi:10.1056/NEJM200001203420302
Vardi M, Levy NS, Levy AP. Vitamin E in the prevention of cardiovascular disease: the importance of proper patient selection . J Lipid Res . 2013;54(9):2307-2314. doi:10.1194/jlr.R026641
Wang T, Xu L. Circulating Vitamin E Levels and Risk of Coronary Artery Disease and Myocardial Infarction: A Mendelian Randomization Study . Nutrients . 2019;11(9):2153. Published 2019 Sep 9. doi:10.3390/nu11092153
Saremi A, Arora R. Vitamin E and cardiovascular disease . Am J Ther . 2010 May-Jun;17(3):e56-65. doi:10.1097/MJT.0b013e31819cdc9a
Dreher D, Junod AF. Role of oxygen free radicals in cancer development . Eur J Cancer . 1996 Jan;32A(1):30-8. doi:10.1016/0959-8049(95)00531-5
Yang CS, Luo P, Zeng Z, Wang H, Malafa M, Suh N. Vitamin E and cancer prevention: Studies with different forms of tocopherols and tocotrienols . Mol Carcinog . 2020 Apr;59(4):365-389. doi:10.1002/mc.23160
Ju J, Picinich SC, Yang Z, Zhao Y, Suh N, Kong AN, Yang CS. Cancer-preventive activities of tocopherols and tocotrienols . Carcinogenesis . 2010 Apr;31(4):533-42. doi:10.1093/carcin/bgp205
Klein EA, Thompson IM Jr, Tangen CM, et al. Vitamin E and the risk of prostate cancer: the Selenium and Vitamin E Cancer Prevention Trial (SELECT) . JAMA . 2011;306(14):1549-1556. doi:10.1001/jama.2011.1437
Khoo HE, Ng HS, Yap WS, Goh HJH, Yim HS. Nutrients for Prevention of Macular Degeneration and Eye-Related Diseases . Antioxidants (Basel) . 2019;8(4):85. Published 2019 Apr 2. doi:10.3390/antiox8040085
Zhang Y, Jiang W, Xie Z, Wu W, Zhang D. Vitamin E and risk of age-related cataract: a meta-analysis . Public Health Nutrition . 2015;18(15):2804-2814. doi:10.1017/s1368980014003115
National Institute on Aging: Cognitive Health and Older Adults
Morley JE, Morris JC, Berg-Weger M, et al. Brain health: the importance of recognizing cognitive impairment: an IAGG consensus conference. J Am Med Dir Assoc . 2015;16(9):731-739. doi:10.1016/j.jamda.2015.06.017
Dysken MW, Sano M, Asthana S, et al. Effect of vitamin E and memantine on functional decline in Alzheimer disease: the TEAM-AD VA cooperative randomized trial [published correction appears in JAMA. 2014 Mar 19;311(11):1161]. JAMA . 2014;311(1):33-44. doi:10.1001/jama.2013.282834
Sano M, Ernesto C, Thomas RG, Klauber MR, Schafer K, Grundman M, Woodbury P, Growdon J, Cotman CW, Pfeiffer E, Schneider LS, Thal LJ. A controlled trial of selegiline, alpha-tocopherol, or both as treatment for Alzheimer's disease. The Alzheimer's Disease Cooperative Study . N Engl J Med . 1997 Apr 24;336(17):1216-22. doi:10.1056/NEJM199704243361704
Petersen RC, Thomas RG, Grundman M, Bennett D, Doody R, Ferris S, Galasko D, Jin S, Kaye J, Levey A, Pfeiffer E, Sano M, van Dyck CH, Thal LJ; Alzheimer's Disease Cooperative Study Group. Vitamin E and donepezil for the treatment of mild cognitive impairment. N Engl J Med . 2005 Jun 9;352(23):2379-88. doi:10.1056/NEJMoa050151
Keen MA, Hassan I. Vitamin E in dermatology. Indian Dermatol Online J . 2016;7(4):311-315. doi:10.4103/2229-5178.185494
Chiu A, Kimball AB. Topical vitamins, minerals and botanical ingredients as modulators of environmental and chronological skin damage . Br J Dermatol . 2003 Oct;149(4):681-91. doi: 10.1046/j.1365-2133.2003.05540.x
Pehr K, Forsey RR. Why don't we use vitamin E in dermatology? CMAJ. 1993 Nov 1;149(9):1247-53. PMID:8221479
Schürks M, Glynn RJ, Rist PM, Tzourio C, Kurth T. Effects of vitamin E on stroke subtypes: meta-analysis of randomised controlled trials . BMJ . 2010 Nov 4;341:c5702. doi:10.1136/bmj.c5702
National Library of Medicine. National Center for Biotechnology Information. Vitamin E Compound Summary .
National Institutes of Health, Office of Dietary Supplements. Vitamin E fact sheet for health professionals .
Podszun M, Frank J. Vitamin E–drug interactions: molecular basis and clinical relevance . Nutrition Research Reviews . 2014;27(2):215-231. doi:10.1017/s0954422414000146
Emami MR, Jamshidi S, Zarezadeh M, et al. Can vitamin E supplementation affect obesity indices? A systematic review and meta-analysis of twenty-four randomized controlled trials . Clin Nutr. 2021;40(5):3201-3209. doi:10.1016/j.clnu.2021.02.002
Gu W, Wu H, Hu C, et al. The association of dietary vitamin intake time across a day with cardiovascular disease and all-cause mortality . Front Cardiovasc Med . 2022;9:822209. doi:10.3389/fcvm.2022.822209
By Shoshana Pritzker RD, CDN, CSSD, CISSN Shoshana Pritzker RD, CDN is a sports and pediatric dietitian, the owner of Nutrition by Shoshana, and is the author of "Carb Cycling for Weight Loss." Shoshana received her B.S in dietetics and nutrition from Florida International University. She's been writing and creating content in the health, nutrition, and fitness space for over 15 years and is regularly featured in Oxygen Magazine, JennyCraig.com, and more.

- ‹ Prev
- Next ›
1.1 Introduction
1.2 homologues: nomenclature and structure, 1.3 physicochemical properties, 1.4 sources, 1.5 chemical synthesis, 1.6 analysis, 1.7 functions and applications, 1.8 stability, chapter 1: vitamin e: structure, properties and functions.
- Published: 04 Feb 2019
- Special Collection: 2019 ebook collection Series: Food Chemistry, Function and Analysis
- Open the Chapter PDF for in another window
- Get permissions
- Cite Icon Cite
E. Niki and K. Abe, in Vitamin E: Chemistry and Nutritional Benefits, ed. E. Niki, The Royal Society of Chemistry, 2019, pp. 1-11.
Download citation file:
- Ris (Zotero)
- Reference Manager
Vitamin E is the collective name for lipophilic, naturally occurring compounds whose molecular structure is comprised of a chromanol ring with a side chain located at the C2 position and includes four tocopherols and four tocotrienols. Vitamin E, discovered as a dietary factor essential for normal reproduction, is now accepted as a major free radical scavenging antioxidant in humans and protects biological molecules from detrimental oxidative modifications. The structures and properties of vitamin E homologues and their sources, functions, and applications are summarized.
In 1922, Evans and Bishop demonstrated the existence of a hitherto unrecognized dietary factor essential for normal reproduction in the rat. 1 It was accepted at that time that the most striking function of vitamin E was to provide a normal gestation in a pregnant rat to prevent the resorption of the embryos which invariably occurred in its absence. 2 This unknown dietary factor X was found to be present in green lettuce, dried alfalfa leaves, wheat, and oats. Evans isolated the factor X from wheat germ oil, provided the chemical formula C 29 H 50 O 2 and proposed the name α-tocopherol in 1936. 3 The structural formula for α-tocopherol was provided by Fernholz in 1938. 4 Tocotrienols were discovered much later than tocopherol and named in the early 1960s. 5,6
Olcott found that the lipid fractions of vegetable oils contained antioxidants against the oxidative deterioration of lard. 7 Since then, it has been unequivocally demonstrated that vitamin E acts as an essential antioxidant in vivo as well as in vitro and plays an important role in the prevention of detrimental oxidative damage of biological molecules. 8–11 More recently, the non-antioxidant functions of vitamin E, including cellular signaling, gene regulation, membrane processes, and nerve functions, have also received much attention. 12–14 However, many issues are still controversial and remain to be elucidated. Sound information based on solid chemical evidence is essential for understanding the role of vitamin E in vivo as well as in vitro .
Vitamin E is a plant-derived, lipid-soluble substance whose molecular structure is comprised of a chromanol ring with a side chain located at the C2 position. Vitamin E refers to a group of eight different compounds: α-, β-, γ-, and δ-tocopherols and the corresponding four tocotrienols. The four tocopherols have a saturated phytyl side chain, while tocotrienols have an unsaturated isoprenyl side chain containing three double bonds at C3′, C7′, and C11′. The double bonds of tocotrienols' side chains at C3′ and C7′ have a trans -configuration. The α-, β-, γ-, and δ-forms differ with respect to the number and position of methyl groups on the chromanol ring. The α-forms of tocopherol and tocotrienol have three methyl groups at the C5, C7, and C8-positions of the chromanol ring, while the β- and γ-forms have two and the δ-forms have one methyl group as illustrated in Figure 1.1 .

Chemical structure of vitamin E homologues.
In addition to tocopherols and tocotrienols, tocomonoenols and tocodienols containing a single and two double bond unsaturation, respectively, have also been found in nature. For example, a tocomonoenol with a single double bond at carbon 11′, 2,5,7,8-tetramethy1-2-(4′,8′,12′-trimethyltrideca-11′-enyl)-6-chromanol, was isolated from palm and rice bran oils. 15 Since then, several groups have detected tocomonoenols in plants and plant foods, such as α-tocomonoenol in palm oil, 16–22 pumpkin seed oil ( Cucurbita pepo L.), 23 and sunflower oil ( Helianthus annuus ), 24 γ-tocomonoenol in pumpkin seed oil, 22,23 δ-tocomonoenol in kiwi ( Actinidia chinensis ), 25 and β-, γ-, and δ-tocomonoenol in the leaves of Kalanchoe daigremontiana and Phaseolus coccineus . 26 A tocomonoenol with an unsaturation at the isoprenoid-chain terminus was also found in the tissues of salmon. 27 Furthermore, tocodienols with two double bonds at carbon 7′ and 11′ were identified in palm oil. 16,21
Tocopherols contain three chiral carbons, one at C2 in the chromanol ring and two in the side chain at C4′ and C8′. Naturally occurring α-tocopherol contains chiral carbons in the R -conformation, 2 R , 4′ R , and 8′ R -α-tocopherol. α-Tocotrienol has one chiral center at C2 in the chromanol ring and natural tocotrienols occur as the R -isoform. On the other hand, the chemical synthesis of α-tocopherol produces an equimolar mixture of eight different stereoisomers: RRR , SRR , RSR , RRS , RSS , SSR , SRS , and SSS . The synthetic α-tocopherol is called all-rac-α-tocopherol. An equimolar mixture of RRR-α-tocopherol and SRR-α-tocopherol is called 2-ambo-α-tocopherol. The IUPAC names of RRR -α-tocopherol and RRR -α-tocotrienol are (2 R )-2,5,7,8-tetramethyl-2-[(4 R ,8 R )-(4,8,12-trimethyltridecyl)]chroman-6-ol and (2 R )-2,5,7,8-tetramethyl-2-[(3 E ,7 E )-4,8,12-trimethyltrideca-3,7,11-trienyl]-3,4-dihydrochromen-6-ol, respectively.
Ester forms of tocopherol and tocotrienols, including acetate, nicotinate, succinate, and phosphate, have been prepared and their action and potential applications have been studied. Vitamin E is easily oxidized when subjected to heat, light, and alkaline conditions, but esters are less susceptible to oxidation and therefore more appropriate for food, cosmetic, and pharmaceutical applications compared to the free form. Polyethylene glycol conjugates of tocopherols and tocotrienols have the ability to form miscible micelles in water due to amphiphilic properties and enhance bioavailability in animals and humans via improving their water solubility and absorption. 28 It was reported that RRR -α-tocopheryl polyethylene glycol 1000 succinate acted as a safe and effective form of vitamin E for reversing or preventing vitamin E deficiency during chronic childhood cholestasis. 29
The tocopherols are viscous oils at room temperature, insoluble in water but soluble in ethanol and aprotic solvents. Vitamin E is a slightly yellow to amber, nearly odorless, clear, viscous oil, which darkens on exposure to air or light by oxidation. The physicochemical properties of α-tocopherol, the most abundant and active form of vitamin E in humans, are summarized in Table 1.1 . 30 The melting point of RRR -α-tocopherol is 3 °C. The optical rotations of tocopherols are very small and depend on the nature of the solvent. The ultraviolet absorption spectra of tocopherols and tocotrienols in ethanol show an absorption maximum at 292–298 nm, while the infrared spectra show OH (2.8 ± 3.0 µm) and CH (3.4 ± 3.5 µm) stretching and a characteristic band at 8.6 µm. α-Tocopherol is fluorescent with an emission maximum about 325 nm in a hydrophobic solution. The bond dissociation energy of α-tocopherol's O–H bond is 77.1 kcal mol −1 . 31 The p K a values for α-, β-, γ-, and δ-tocopherol in a micellar solution were reported as 13.1, 12.8, 12.7, and 12.6 respectively. 32
Physicochemical properties of α-tocopherol
Bond dissociation energy. 31
The partition coefficient of α-tocopherol is 12.2, while that for ascorbic acid is −1.85, 30 showing their lipophilic and hydrophilic characters, respectively.
Numerous foods provide vitamin E. Seeds and fruits are among the best sources of vitamin E. Green leafy vegetables are also important sources. Only plants and photosynthetic organisms are able to synthesize vitamin E. 33,34 The synthesis is facilitated by enzymes to produce stereospecific tocopherols: RRR -tocopherols. 35 Tocopherols and tocotrienols can be extracted and purified or concentrated from vegetable oils and other higher plant materials. Dietary supplements are another source of vitamin E. Most vitamin E supplements contain substantially higher amounts of vitamin E than foods. Vitamin E in dietary supplements and fortified foods is often esterified to prolong its shelf life while protecting its antioxidant properties.
The contents and composition of tocopherols and tocotrienols in natural oils vary markedly between the plant species and even within the same species. Tocopherols are widely distributed in higher plants, whereas tocotrienols occur only in some non-photosynthetic tissues. Some examples of the contents in natural edible oils adopted from several reports 36–41 are shown in Table 1.2 . α-Tocopherol is the major tocopherol in palm, olive, and sunflower oils, whereas the contents of γ-tocopherol in some edible oils such as corn, rapeseed, and soybean oils are higher than α-tocopherol.
The contents of tocopherols (T) and tocotrienols (T3) in representative edible oils. Adapted from ref. 36–41 a
In mg per 100 g oil. Major components are shown in bold.
The major sources of tocotrienols are palm, rice, and annatto, the ratio of tocopherol–tocotrienol in each being 25 : 75, 50 : 50, and 0.1 : 99.9, respectively. 42 Palm oil contains considerable amounts of α-, γ-, and δ-tocotrienols. γ-Tocotrienol is the major vitamin E isoform in the oil extracted from rice bran 39,43 while β-tocopherol is one of the major isoforms found in wheat germ oil. 36,37 Interestingly, the lipid fraction of annatto ( Bixa orellana L.) seeds contained only tocotrienols, mainly δ-tocotrienol, but no tocopherols. 44
Due to wide applications in the pharmaceutical, food, and cosmetic industries, about 35 000 tons of vitamin E is manufactured per year worldwide. 45 All-racemic-α-tocopherol, all-rac-α-tocopherol, an equimolar mixture of all eight stereoisomers, is industrially the most important product and is prepared either by total synthesis or originates from natural sources. It is mainly applied as an acetate ester. The industrial synthesis consists of three major parts: the preparation of 2,3,5-trimethylhydroquinone, the production of the side chain component, and the condensation reaction. 45
Pure RRR -α-tocopherol is chemically prepared by semi-synthesis. Vegetable oils refined on a large scale and isolated by a combination of several separation methods contain mixtures of RRR -tocopherols, which are converted to RRR -α-tocopherol by permethylation reactions. The efforts and strategies to synthesize tocopherols and tocotrienols have been described in detail. 45
Natural products contain mixtures of isomeric tocopherols and tocotrienols together with minor amounts of tocomonoenols and tocodienols. They are metabolized and oxidized to produce many kinds of compounds. The biological samples contain complicated mixtures of vitamin E isoforms and their metabolites and oxidation products. The identification and quantitation of vitamin E isoforms and their products are important for elucidating their role and functions. Sample preparation is the most time-consuming and important step in analysis, because it is the main source of errors. Many analytical methods including colorimetric, fluorometric, gas chromatographic (GC), high performance liquid chromatographic (HPLC), 46 GC-MS, 47 and HPLC-MS 47,48 have been reported (see also Chapter 2). Concerning public documents for the quantitative determination method of vitamin E in active pharmaceutical ingredients, United States and European Pharmacopeia adopt the GC method, while Japanese Pharmacopeia adopts the HPLC method. Each of these methods has its merits and demerits. At the present time, HPLC methods are the most widely applied.
HPLC conditions for vitamin E analysis have been summarized in several reviews. 46,47,49,50 Vitamin E and products are obtained from natural products, food matrices, and biological samples by direct extraction, solid-phase extraction, and saponification. Care should be taken to avoid artifactual oxidation and decomposition during preparation of samples and analysis. The use of electrochemical (amperometric), fluorometric (Ex. 290–295 nm, Em. 320–330 nm), or MS detection is much more sensitive and specific than the conventional UV detection. Tocol, 2-methyl-2-(4,8,12-trimethyltridecyl)-6-chromanol, may be the best compound to use as an internal standard because its characteristics are similar to vitamin E. Deuterium-labelled α-tocopherol acetate is commonly used as a standard in MS analysis. In most vitamin E analyses, atmospheric pressure chemical ionization (APCI) is used in the positive ionization mode. It may be noted that supercritical-fluid chromatography using CO 2 and ethanol as a mobile phase, NH 2 as a stationary phase, and mass spectrometry for the detection and quantification of vitamin E homologues has been proposed as a “greener” analytical strategy. 51,52
Vitamin E is a physiologically essential micronutrient and has been applied in various fields including medicine, pharmaceutics, cosmetics, and foods. Vitamin E is assumed to play an important role in the promotion of health and prevention and/or treatment of some diseases and disorders. The daily recommended intake is 15 mg (22.4 IU, International Unit) for adults [ https://ods.od.nih.gov/factsheets/VitaminE-HealthProfessional/ ].
Multiple functions of vitamin E have been demonstrated or proposed, including (1) antioxidant by scavenging free radicals, especially peroxyl radicals, and singlet oxygen, (2) membrane stabilization by forming complexes with destabilizing molecules so as to prevent disturbance of the amphipathic balance within the structure, (3) physiological regulator of enzyme activity, cellular signaling, cell proliferation, and gene expression, which is not directly related to antioxidant action, (4) inhibition of platelet coagulation, (5) prevention of diseases including neurological disorders, cardiovascular diseases, age-related eye and skin damage, and infertility, and (6) biocompatible modifier of biomaterials and medical devices, for example in high molecular weight polyethylene used in hip and knee implants. It has been argued that tocotrienols possess additional positive health effects beyond those of tocopherols including, for example, induction of immune responses and lowering of serum cholesterol levels. 53–55
Among these functions, the role of vitamin E as an antioxidant against free radical-mediated lipid peroxidation has been unequivocally demonstrated and it appears that this is the most important physiological function of this vitamin. Vitamin E also inhibits air oxidation of foods, oils, and industrial materials to extend their lifetime. The physiological significance of other functions that are not related to antioxidant function must be established in a future study.
Vitamin E is widely used as a dietary supplement, by itself or together with other micronutrients such as vitamin C, to promote health and to reduce the risk of or prevent diseases that are assumed to arise from detrimental oxidative modification of biological molecules. Vitamin E is used to fortify some foods and beverages.
Deficiency of vitamin E is uncommon as typical diets appear to provide sufficient amounts, although malnutrition and genetic disorders may result in vitamin E deficiency. Premature babies of very low birth weight might be deficient in vitamin E. Further, people with fat-malabsorption disorders 56 and inherited disorders in which the liver's α-tocopherol transfer protein (α-TTP) is defective or absent 57 or there are decreased levels of selenoproteins 58 are more likely to become vitamin E deficient and require high doses of supplemental vitamin E.
The potential role of vitamin E against periodontal disease, 59 nonalcoholic steatohepatitis, 60 and sarcopenia 61 has received attention. Insufficient micronutrient intake (vitamins and phosphorus) was significantly associated with severity of periodontal disease. 62 A systematic review showed significant improvement of periodontal parameters by vitamin E and lycopene. 63 Vitamin E may mitigate age-associated skeletal dysfunction and enhance muscle regeneration, thus attenuating sarcopenia. 64
Vitamin E is also used for biomedical materials. α-Tocopherol is blended to a dialysis membrane for clinical management of chronic hemodialysis patients to improve stability and functions. 65 Vitamin E-blended ultra-high molecular weight polyethylene (UHMWPE) has been developed as a material for use in total knee and hip replacements. 66 α-Tocopherol is accepted to improve oxidation resistance while maintaining wear resistance and fatigue strength.
The poor water solubility of vitamin E has greatly limited its application. Investigations to improve both oral and topical encapsulation and formulations of vitamin E have been widely carried out and various delivery systems for vitamin E have been developed to overcome this problem and to enhance solubility, permeation, and bioavailability. Liposomes, 67 nano-emulsions, and lipid nanoparticles 68 are some examples. 69 The tocopheryl ester of polyethylene glycol and tocopheryl phosphate are water soluble. Polyethylene conjugates of tocotrienols have also been studied. 28
Dietary polyphenols such as quercetin are converted to glucoside and/or sulfate derivatives, or their O -methyl derivatives, during absorption into the body, and presents as these conjugated metabolites in circulating blood. Formation of the metabolites of tocopherol such as glucoside, sulfate, and O -methyl derivatives in vivo has not been reported but α-tocopherol glucoside was synthesized from 2-hydroxymethyl-2,5,7,8-tetramethylchroman-6-ol and maltose by transglycosylation with α-glucosidase from Saccharomyces species. 70 The glycosylated product, 2-(α- d -glucopyranosyl)methyl-2,5,7,8-tetramethylchroman-6-ol, is water soluble and acts as a radical scavenging antioxidant. 70,71 δ-Tocopherol glucoside was prepared and its effects during its topical application on skin were studied. 72
One important question is whether or not each vitamin E isoform exerts its own specific function which is not shared with other isoforms. It has been argued that tocotrienol exerts some functions that tocopherol does not, and that tocopherol interferes with such tocotrienol functions. 42 These important issues must be clarified in future studies.
Vitamin E is stable at ambient temperature, but it is readily oxidized at high temperature, under light or in an alkaline medium. Frying is one of the most common methods of food preparation and during the frying process, usually between 160–190 °C, vitamin E is oxidized to give complicated mixtures of products including tocored (5,6-tocopheryldione) and dimers that are assumed to be formed by a recombination of tocopheroxyl radicals. α-Tocopherol is oxidized to α-tocopheroxyl radical by transition metal ions such as ferric ions (Fe 3+ ) and cupric ions (Cu 2+ ).
- Campaigning and outreach
- News and events
- Awards and funding
- Privacy policy
- Journals and databases
- Locations and contacts
- Membership and professional community
- Teaching and learning
- Help and legal
- Cookie policy
- Terms and conditions
- Get Adobe Acrobat Reader
- Registered charity number: 207890
- © Royal Society of Chemistry 2023
This Feature Is Available To Subscribers Only
Sign In or Create an Account

- school Campus Bookshelves
- menu_book Bookshelves
- perm_media Learning Objects
- login Login
- how_to_reg Request Instructor Account
- hub Instructor Commons
Margin Size
- Download Page (PDF)
- Download Full Book (PDF)
- Periodic Table
- Physics Constants
- Scientific Calculator
- Reference & Cite
- Tools expand_more
- Readability
selected template will load here
This action is not available.
9.2: Vitamin E
- Last updated
- Save as PDF
- Page ID 40976

- Brian Lindshield
- Kansas State University
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
There are 8 different forms of vitamin E: 4 tocopherols and 4 tocotrienols. The difference between tocopherols and tocotrienols is that the former have a saturated tail, while the latter have an unsaturated tail. Within tocopherols and tocotrienols, the difference between the different forms is the position of the methyl groups on the ring. The 4 different forms within the tocopherol and tocotrienols are designated by the Greek letters: alpha, beta, gamma, and delta. The difference in these structures is shown in the figures below.

Query \(\PageIndex{1}\)
Query \(\PageIndex{2}\)
For reasons that will be covered in a later subsection, the primary form of vitamin E found in the body is alpha-tocopherol. The major, and possibly only, function of vitamin E is as an antioxidant. When it serves as an antioxidant it forms an alpha-tocopherol radical, as shown below.

Alpha-tocopherol is believed to be the first part of an antioxidant network (shown below) where it is oxidized to donate an electron to stabilize reactive oxygen species. Alpha-tocopherol radical can then be reduced by the donation of an electron from ascorbate.

To help protect the antioxidant function of alpha-tocopherol (by preventing the formation of alpha-tocopherol radical) in foods and during digestion, some manufacturers have added compounds to this site of alpha-tocopherol through ester bonds. These are referred to as alpha-tocopherol derivatives or alpha-tocopherol esters. The most common forms are alpha-tocopherol acetate, alpha-tocopherol succinate, and alpha-tocopherol phosphate (Ester-E®). The figures below show the structure of alpha-tocopherol acetate, and the structure of succinic acid.

Alpha-tocopherol derivatives, such as acetate in alpha-tocopherol acetate, are cleaved prior to absorption in the small intestine by esterases, meaning that alpha-tocopherol is absorbed, not the alpha-tocopherol derivative.
Query \(\PageIndex{3}\)
Alpha-Tocopherol: Natural vs. Synthetic
In addition to being found naturally in foods, alpha-tocopherol can also be synthesized. It is important to know whether alpha-tocopherol is natural or synthetic because the stereochemistry (spatial arrangement) differs between these forms. In some cases stereochemistry is used to three dimensionally depict whether a molecule is coming out towards you or alternatively away from you. Alpha-tocopherol contains 3 chiral centers (non-superimposable mirror images) designated as R or S.
The 3 chiral centers in alpha-tocopherol are located at the 2, 4’, and 8’ positions. You can see the full numbering of tocopherols in the link below. In short, the rings are normal numbers and the tail are prime numbers.
Tocopherol Numbering
The figure below shows the 3 chiral centers without the other numbers.

In natural alpha-tocopherol, all 3 chiral centers are in the R configuration. Thus, it is designated RRR-alpha-tocopherol. The R’s represent the 2, 4’, and 8’ positions of alpha-tocopherol, respectively, as shown below 4 .

Query \(\PageIndex{4}\)
Synthetic alpha-tocopherol is a racemic (equal) mixture of all the different possibilities at the three chiral centers. These are:
The two forms of alpha-tocopherol are designated (these are placed before alpha-tocopherol to indicate whether it is natural or synthetic) as listed below:
New designation: RRR-alpha-tocopherol (because all 3 positions are RRR)
Old designation: d-alpha-tocopherol
New designation: all-rac-alpha-tocopherol (because it is a racemic mixture)
Old designation: dl-alpha-tocopherol
The old d and dl designations were describing the chemical structure that are sometimes still used. Keep in mind the natural and synthetic are describing the stereochemistry of alpha-tocopherol and not whether it is naturally derived. For example, there are natural alpha-tocopherol derivatives where the derivatives are added through synthetic procedures.
Query \(\PageIndex{5}\)
Query \(\PageIndex{6}\)
Vitamin E Absorption, Metabolism, & Excretion
You might be saying to yourself, “who cares about natural versus synthetic alpha-tocopherol.” But the small change in stereochemistry makes a big difference in how alpha-tocopherol is maintained in the body.
All forms of vitamin E (tocopherols, tocotrienols) are absorbed equally. Fat-soluble vitamins are handled like lipids and thus are incorporated into chylomicrons that have triglycerides removed by lipoprotein lipase. The chylomicron remnants containing the different forms of vitamin E are then taken up by the liver. The figure below shows the absorption, metabolism, and excretion of vitamin E.

Query \(\PageIndex{7}\)
The liver contains a protein called alpha-tocopherol transfer protein (alpha-TTP), which is responsible for maintaining higher levels of alpha-tocopherol in the body. Alpha-TTP preferentially binds to 2R alpha-tocopherol and helps facilitate its incorporation into VLDL. 2R means any form of alpha-tocopherol in which the 2 position is in the R conformation. The following table summarizes the forms of alpha-tocopherol that bind well to alpha-TTP, and those that don't bind well to alpha-TTP.
Query \(\PageIndex{8}\)
Other forms of vitamin E (gamma-tocopherol, tocotrienols) also don't bind well to alpha-TTP and thus, are found in lower levels than alpha-tocopherol in the body. The following graph shows plasma (liquid component of blood) vitamin E levels from a study in which subjects were given 150 mg each of RRR-alpha-tocopherol, all-rac-alpha-tocopherol, or gamma-tocopherol 5 .

As you can see in the figure, there was a greater rise in the plasma alpha-tocopherol levels after receiving RRR-alpha-tocopherol vs. all-rac-alpha-tocopherol. This is not a surprise because approximately 50% of all-rac-alpha-tocopherol is 2R alpha-tocopherol that binds well with alpha-TTP. You can also see that the plasma gamma-tocopherol concentration is much lower than either natural or synthetic alpha-tocopherol.
From VLDL and subsequent lipoproteins, vitamin E reaches tissues, with most vitamin E in the body being found in the adipose tissue. There are 2 main routes of vitamin E excretion. The major route of excretion is through bile that is then excreted in feces. The second route is in the urine after vitamin E is chain-shortened in a process similar to beta-oxidation to make them more water-soluble.
Query \(\PageIndex{9}\)
Dietary Vitamin E & Amounts Found in Body
The best food sources of vitamin E are primarily oils and nuts. As you can see below, the forms of vitamin E that nuts and oils contain varies, with the two major forms being alpha and gamma-tocopherol. Soybean, corn, and flaxseed oils are good sources of gamma-tocopherol. Palm and canola oils contain almost equal amounts of alpha-tocopherol and gamma-tocopherol. Safflower oil, almonds, sunflower oil, and wheat germ oil are good sources of alpha-tocopherol. Beta-tocopherol and delta-tocopherol are found in lower levels in foods. Tocotrienols, for the most part, are not found in high levels in the diet. The amount of tocopherols in different nuts and oils are shown in the figure below.

Three-fourths of the oil Americans consume is soybean oil. As a result, it is estimated that we consume 2-4 times more gamma-tocopherol than alpha-tocopherol. Europeans consume more olive, sunflower, and canola oil and thus are believed to consume at least 2 times more alpha-tocopherol than gamma-tocopherol 6 .
Despite Americans’ higher intake of gamma tocopherol compared to other countries, our serum (liquid portion of blood without coagulation proteins) concentrations do not differ much as illustrated in the table below.
There are 3 different studies that have reported serum levels in the United States.
Tissue concentrations, for the most part, also indicate a greater accumulation of alpha-tocopherol than gamma-tocopherol as shown in the table below.
Query \(\PageIndex{10}\)
Vitamin E Deficiency & Toxicity
Vitamin E deficiency is extremely rare. Depletion studies require years on a vitamin E-deficient diet to cause deficiency 7 . Deficiency primarily occurs in people with lipid malabsorption problems or Ataxia with Isolated Vitamin E Deficiency (AVED). Individuals with AVED have a mutation in their alpha-TTP that prevents it from functioning correctly. The primary symptoms of vitamin E deficiency are neurological problems.
Query \(\PageIndex{11}\)
High levels of vitamin E intake do not result in a noted toxicity. However, higher levels of intake of alpha-tocopherol (like achieved by taking supplements) are associated with decreased blood coagulation. In particular, hemorrhagic stroke has been linked to high alpha-tocopherol intake levels. The link below shows that in this condition a blood vessel ruptures or leaks in the brain.
Hemorrhagic Stroke
It is believed that this increased bleeding risk is due to a alpha-tocopherol metabolite that has anti-vitamin K activity. This potential antagonism will be described more in the vitamin K section.
Query \(\PageIndex{12}\)
Vitamin E DRI & IUs
Before 2001, all forms of vitamin E contributed to the RDA, using a measure called alpha-tocopherol equivalents. This indicator essentially provided a value for all forms relative to alpha-tocopherol. In 2001, the Dietary Reference Intake (DRI) committee decided only 2R forms of alpha-tocopherol should be used to estimate the requirement, because these forms bind to alpha-TTP. Thus, other forms of vitamin E (gamma-tocopherol, tocotrienols etc.) do not count toward the requirement and the unit is now mg of alpha-tocopherol. As a result, soybean, corn, and flaxseed oils, which are good sources of gamma-tocopherol, are no longer considered to be good sources of vitamin E. The figure below is a reminder of the tocopherol content of different nuts and oils.

Query \(\PageIndex{13}\)
Another level of complexity is added by international units (IU). IUs are a unit that are used to describe the bioactivity of different compounds, including 4 vitamins: A, D, E, and C. You might be wondering why these 4 vitamins, it is because these are the ones that were chosen by those who set IUs. Most likely because these vitamins are commonly included in supplements. It would be less confusing if these units were not used. However, most supplements use IUs, IUs are not as common on food items.
For vitamin E, IUs are specific for alpha-tocopherol and adjusted for the molecular weight of the different forms (alpha-tocopherol acetate etc.). The conversion factors for converting IU to mg of alpha-tocopherol are:
0.67 for RRR-alpha-tocopherol (and its esters)
0.45 for all-rac-alpha-tocopherol (and its esters)
Here are some example calculations showing how to use these conversion factors:
For a supplement containing 100 IU of RRR-alpha tocopherol:
100 IU X 0.67 = 67 mg alpha-tocopherol
For a supplement containing 100 IU of all-rac-alpha tocopherol:
100 IU X 0.45 = 45 mg alpha-tocopherol 7 ,8
Query \(\PageIndex{14}\)
- en.Wikipedia.org/wiki/Radica.../File:VitE.gif
- Packer L, Weber SU, Rimbach G. (2001) Molecular aspects of alpha-tocotrienol antioxidant action and cell signalling. J Nutr 131(2): 369S-373S
- en.Wikipedia.org/wiki/File:Be...%C3%A4ure2.svg
- http://lpi.oregonstate.edu/mic/vitamins/vitamin-E
- Traber MG, Elsner A, Brigelius-Floh R. (1998) Synthetic as compared with natural vitamin E is preferentially excreted as alpha-CEHC in human urine: Studies using deuterated alpha-tocopheryl acetates. FEBS Lett 437(1-2): 145-148.
- Wagner KH, Kamal-Eldin A, Elmadfa I. (2004) Gamma-tocopherol--an underestimated vitamin? Ann Nutr Metab 48(3): 169-188.
- DRI (2000) Dietary reference intakes for vitamin C, vitamin E, selenium, and carotenoids.
- https://ods.od.nih.gov/factsheets/Vi...hProfessional/

Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
Chapter 10: Micronutrients Overview and Role as Antioxidants
10.4 Vitamin E
University of Hawai‘i at Mānoa Food Science and Human Nutrition Program
Vitamin E Functions and Health Benefits
Vitamin E occurs in eight chemical forms, of which alpha-tocopherol appears to be the only form that is recognized to meet human requirements. Alpha-tocopherol and vitamin E’s other constituents are fat-soluble and primarily responsible for protecting cell membranes against lipid destruction caused by free radicals, therefore making it an antioxidant. When alpha-tocopherol interacts with a free radical it is no longer capable of acting as an antioxidant unless it is enzymatically regenerated. Vitamin C helps to regenerate some of the alpha-tocopherol, but the remainder is eliminated from the body. Therefore, to maintain vitamin E levels, you ingest it as part of your diet.
Insufficient levels are rare ( signs and symptoms of such conditions are not always evident) but are primarily the result of nerve degeneration. People with malabsorption disorders, such as Crohn’s disease or cystic fibrosis, and babies born prematurely, are at higher risk for vitamin E deficiency.
Vitamin E has many other important roles and functions in the body such as boosting the immune system by helping to fight off bacteria and viruses. It also enhances the dilation of blood vessels and inhibiting the formation of blood clotting. Despite vitamin E’s numerous beneficial functions when taken in recommended amounts, large studies do not support the idea that taking higher doses of this vitamin will increase its power to prevent or reduce disease risk. [1] [2]
Fat in the diet is required for vitamin E absorption as it is packaged into lipid-rich chylomicrons in intestinal cells and transported to the liver. The liver stores some of the vitamin E or packages it into lipoproteins, which deliver it to cells.
Cardiovascular Disease
Vitamin E reduces the oxidation of LDLs, and it was therefore hypothesized that vitamin E supplements would protect against atherosclerosis . However, large clinical trials have not consistently found evidence to support this hypothesis. In fact, in the “Women’s Angiographic Vitamin and Estrogen Study,” postmenopausal women who took 400 international units (264 milligrams) of vitamin E and 500 milligrams of vitamin C twice per day had higher death rates from all causes. [3]
Other studies have not confirmed the association between increased vitamin E intake from supplements and increased mortality. There is more consistent evidence from observational studies that a higher intake of vitamin E from foods is linked to a decreased risk of dying from a heart attack.
The large clinical trials that evaluated whether there was a link between vitamin E and cardiovascular disease risk also looked at cancer risk. These trials, called the HOPE-TOO Trial and Women’s Health Study, did not find that vitamin E at doses of 400 international units (264 milligrams) per day or 600 international units (396 milligrams) every other day reduced the risk of developing any form of cancer. [4] [5]
Eye Conditions
Oxidative stress plays a role in age-related loss of vision, called macular degeneration. Age-related macular degeneration (AMD) primarily occurs in people over age fifty and is the progressive loss of central vision resulting from damage to the center of the retina, referred to as the macula. There are two forms of AMD, dry and wet, with wet being the more severe form.
In the dry form, deposits form in the macula; the deposits may or may not directly impair vision, at least in the early stages of the disease. In the wet form, abnormal blood vessel growth in the macula causes vision loss. Clinical trials evaluating the effects of vitamin E supplements on AMD and cataracts (clouding of the lens of an eye) did not consistently observe a decreased risk for either. However, scientists do believe vitamin E in combination with other antioxidants such as zinc and copper may slow the progression of macular degeneration in people with early-stage disease.
The brain’s high glucose consumption makes it more vulnerable than other organs to oxidative stress. Oxidative stress has been implicated as a major contributing factor to dementia and Alzheimer’s disease. Some studies suggest vitamin E supplements delay the progression of Alzheimer’s disease and cognitive decline, but again, not all of the studies confirm the relationship. A recent study with over five thousand participants published in the July 2010 issue of the Archives of Neurology demonstrated that people with the highest intakes of dietary vitamin E were 25 percent less likely to develop dementia than those with the lowest intakes of vitamin E. [6]
More studies are needed to better assess the dose and dietary requirements of vitamin E and, for that matter, whether other antioxidants lower the risk of dementia, a disease that not only devastates the mind, but also puts a substantial burden on loved ones, caretakers, and society in general.
Vitamin E Toxicity
Currently, researchers have not found any adverse effects from consuming vitamin E in food. Although that may be the case, supplementation of alpha-tocopherol in animals has shown to cause hemorrhage and disrupt blood coagulation. Extremely high levels of vitamin E can interact with vitamin K-dependent clotting factors causing an inhibition of blood clotting. [7]
Dietary Reference Intakes for Vitamin E
The Recommended Dietary Allowances (RDAs) and Tolerable Upper Intake Levels (ULs) for different age groups for vitamin E are given in Table 10.41 “Dietary Reference Intakes for Vitamin E”.
Table 10.41 Dietary Reference Intakes for Vitamin E [8]
Vitamin E supplements often contain more than 400 international units, which is almost twenty times the RDA. The UL for vitamin E is set at 1,500 international units for adults. There is some evidence that taking vitamin E supplements at high doses has negative effects on health. As mentioned, vitamin E inhibits blood clotting and a few clinical trials have found that people taking vitamin E supplements have an increased risk of stroke. In contrast to vitamin E from supplements, there is no evidence that consuming foods containing vitamin E compromises health.
Dietary Sources of Vitamin E
Add some nuts to your salad and make your own dressing to get a healthy dietary dose of vitamin E.

Vitamin E is found in many foods, especially those higher in fat, such as nuts and oils. Some spices, such as paprika and red chili pepper, and herbs, such as oregano, basil, cumin, and thyme, also contain vitamin E. (Keep in mind spices and herbs are commonly used in small amounts in cooking and therefore are a lesser source of dietary vitamin E.) See Table 10.42 “Vitamin E Content of Various Foods” for a list of foods and their vitamin E contents.
Everyday Connection
To increase your dietary intake of vitamin E from plant-based foods try a spinach salad with tomatoes and sunflower seeds, and add a dressing made with sunflower oil, oregano, and basil.
Table 10.42 Vitamin E Content of Various Foods [9]
- Goodman M, Bostlick RM, Kucuk O, Jones DP. Clinical trials of antioxidants as cancer prevention agents: past, present, and future. Free Radic Biol Med. 2011; 51(5), 1068–84. https://www.ncbi.nlm.nih.gov/pubmed/21683786. Accessed October 5, 2017. ↵
- McGinley C, Shafat A. Donnelly AE. Does antioxidant vitamin supplementation protect against muscle damage. Sports Med. 2009; 39(12), 1011–32. https://www.ncbi.nlm.nih.gov/pubmed/19902983 . Accessed October 5, 2017. ↵
- Waters DD, et al. Effects of Hormone Replacement Therapy and Antioxidant Vitamin Supplements on Coronary Atherosclerosis in Postmenopausal Women: A Randomized Controlled Trial. JAMA. 2002; 288(19), 2432–40. https://jamanetwork.com/journals/jama/fullarticle/195531 . Accessed October 5, 2017. ↵
- HOPE and HOPE-TOO Trial Investigators. Effects of Long-Term Vitamin E Supplementation on Cardiovascular Events and Cancer. JAMA. 2005; 293, 1338–47. http://jama.ama-assn.org/content/293/11/1338.long ., Accessed October 5, 2017. ↵
- Lee IM, et al. Vitamin E in the Primary Prevention of Cardiovascular Disease and Cancer: The Women’s Health Study. JAMA.2005; 294, 56–65. http://jama.ama-assn.org/content/294/1/56.long . Accessed October 5, 2017. ↵
- Devore EE, et al. Dietary Antioxidants and Long-Term Risk of Dementia. Arch Neurol. 2010; 67(7), 819–25. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2923546/?tool=pubmed . Accessed October 5, 2017. ↵
- Dietary Supplement Fact Sheet: Vitamin E.National Institutes of Health, Office of Dietary Supplements. http://ods.od.nih.gov/factsheets/VitaminE-QuickFacts/ . Updated October 11, 2011. Accessed October 5, 2017. ↵
- Source: Dietary Fact Sheet for Health Professionals: Vitamin E. National Institutes of Health, Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminE-HealthProfessional/ . Updated March 26, 2021. Accessed July 31, 2023. ↵
- Source: Dietary Supplement Fact Sheet: Vitamin E.National Institutes of Health, Office of Dietary Supplements. http://ods.od.nih.gov/factsheets/VitaminE-QuickFacts/ . Updated October 11, 2011. Accessed October 5, 2017. ↵
Signs refer to readily observed identifying characteristics of a disease such as swelling, weight loss, or fever. Symptoms are the subjective features of a disease recognized by a patient and/or their doctor.
Absorption is the process of getting nutrients from the digestive tract into the blood or lymph.
Chylomicrons are lipoproteins formed by the merging of a protein carrier, triglycerides, cholesterol, and phospholipids.
Atherosclerosis is a condition that occurs when too much plaque builds up in your arteries, causing them to narrow.
Oxidative stress refers to an imbalance between the production of reactive oxygen species (ROS) orfree radicals and the body’s ability to quench them. In other words, oxidative stress is what your cells experience when you’re making more free radicals than your cells can handle.
Organs are a group of tissues arranged in a specific manner to support a common physiological function.
Principles of Human Nutrition Copyright © by University of Hawai‘i at Mānoa Food Science and Human Nutrition Program is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License , except where otherwise noted.
Review article vitamin E: a multi-functional ingredient for health enhancement and food preservation
- Review Paper
- Published: 23 August 2023
- Volume 17 , pages 6144–6156, ( 2023 )
Cite this article

- Chee Chin Chu 1 ,
- Sook Chin Chew 2 ,
- Wen Ching Liew 3 &
- Kar Lin Nyam ORCID: orcid.org/0000-0002-2410-9823 4
Explore all metrics
Vitamin E (tocopherols and tocotrienols) has demonstrated significant biological effects on enhancing human health and play a promising role in food systems. Studies have shown the relative antioxidant activity of vitamin E contributes to food preservation. It can reduce the negative impact of chemical reactions on food systems by improving their safety, nutritional value, and shelf-life. This review aims to discuss the functionality of vitamin E, mainly focusing on its sources, physico-chemical characteristics, biological functions, and application as a food stabilizer. Relevant studies were identified through searches in online databases such as Scopus, PubMed, ISI Web of Science, and Google Scholar using appropriate keywords. Vitamin E has been found to act on cellular signaling pathways, effectively combating oxidative stress which benefits for anti-inflammation, anti-cancer, cardioprotection, neuroprotection, skin health, and other degenerative conditions. The functions of γ- and δ- tocotrienol and tocopherol have been found to exhibit anti-inflammation and anti-cancer properties. Vitamin E also contributes to cardio health via cardiomyocyte anti-apoptosis. Additionally, vitamin E offers good protection against lipid peroxidation under food processing and storage conditions. Vitamin E works in oils, fats, and active packaging by stabilizing their lipid components to prevent off-flavours and changes in the colour of the food constituents. Supplementation of α-tocopherol up to 0.2% in oils is able provide higher oxidative stability. Therefore, it can be inferred that vitamin E could be utilized as a functional ingredient in food preservation and for enhancing nutritional quality.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
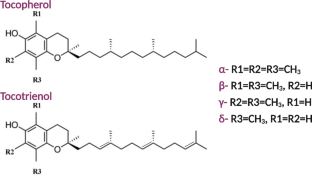
Similar content being viewed by others

Food Antioxidants: Functional Aspects and Preservation During Food Processing

Functional Foods as Source of Bioactive Principles: Some Marked Examples

Functional components and medicinal properties of food: a review
V. Boccardi, M. Baroni, F. Mangialasche, P. Mecocci, Vitamin E family: role in the pathogenesis and treatment of Alzheimer’s disease. TRCI. 2 , 182–191 (2016). https://doi.org/10.1016/j.trci.2016.08.002
Article PubMed PubMed Central Google Scholar
Z. Zou, L. Dai, D. Liu, W. Du, Research progress in enzymatic synthesis of vitamin E ester derivatives. Catalysts. 11 , 739 (2021). https://doi.org/10.3390/catal11060739
Article CAS Google Scholar
A. Durazzo, A. Nazhand, M. Lucarini, A.M. Delgado, M.D. Wit, K.L. Nyam, A. Santini, M.F. Ramadan, Occurrence of tocols in foods: An updated shot of current databases. J. Food Qual. 2021, 1–7 (2021). https://doi.org/10.1155/2021/8857571
S.N. Selamat, I.I. Muhamad, Z. Idham, N. Pae, Retention of alpha tocopherol and antioxidant activity of encapsulated palm mixed vitamin E in formulated blends. MOJFPT. 6 , 272–278 (2018). https://doi.org/10.15406/mojfpt.2018.06.00175
Article Google Scholar
A. Delgado, S. Al-Hamimi, M.F. Ramadan, M.D. Wit, A. Durazzo, K.L. Nyam, M. Issaoui, Contribution of tocols to food sensorial properties, stability, and overall quality. J. Food Qual. 2020, 1–8 (2020). https://doi.org/10.1155/2020/8885865
B. Yi, M.J. Kim, J. Lee, Oxidative stability of oil-in-water emulsions with α-tocopherol, charged emulsifier, and different oxidative stress. Food Sci. Biotechnol. 27 , 1571–1578 (2018). https://doi.org/10.1007/s10068-018-0407-0
Article CAS PubMed PubMed Central Google Scholar
G.K. Samdani, D.J. McClements, E.A. Decker, Impact of phospholipids and tocopherols on the oxidative stability of soybean oil-in-water emulsions. J. Agric. Food Chem. 66 , 3939–3948 (2018). https://doi.org/10.1021/acs.jafc.8b00677
Article CAS PubMed Google Scholar
L. Wang, X. Yu, F. Geng, C. Cheng, J. Yang, Q. Deng, Effects of tocopherols on the stability of flaxseed oil-in-water emulsions stabilized by different emulsifiers: interfacial partitioning and interaction. Food Chem. 374 , 131691 (2022). https://doi.org/10.1016/j.foodchem.2021.131691
Z.Y. Niu, Y.N. Min, F.Z. Liu, Dietary vitamin E improves meat quality and antioxidant capacity in broilers by upregulating the expression of antioxidant enzyme genes. J. Appl. Anim. Res. 46 , 397–401 (2018). https://doi.org/10.1080/09712119.2017.1309321
F. Pop, L. Mihalescu, Effects of α-tocopherol and citric acid on the oxidative stability of alimentary poultry fats during storage at low temperatures. Int. J. Food Prop. 20 , 1085–1096 (2017). https://doi.org/10.1080/10942912.2016.1199037
A.I.O. Jideani, H. Silungwe, T. Takalani, A.O. Omolola, H.O. Udeh, T.A. Anyasi, Antioxidant-rich natural fruit and vegetable products and human health. Int. J. Food Prop. 24 , 41–67 (2021). https://doi.org/10.1080/10942912.2020.1866597
Q. Jiang, S. Im, J.G. Wagner, M.L. Hernandez, D.B. Peden, Gamma-tocopherol, a major form of vitamin E in diets: insights into antioxidant and anti-inflammatory effects, mechanisms, and roles in disease management. Free Radic. Biol. Med. 178 , 347–359 (2022). https://doi.org/10.1016/j.freeradbiomed.2021.12.012
E. Reboul, E. Vitamin, bioavailability: Mechanisms of intestinal absorption in the spotlight. Antioxidants 6, 1–11 (2017). https://doi.org/10.3390/antiox6040095
M. Sharifi-Rad, N.V. Anil Kumar, P. Zucca, E.M. Varoni, L. Dini, E. Panzarini, J. Rajkovic, P.V.T. Fokou, E. Azzini, I. Peluso, A.P. Mishra, M. Nigam, Y.E. Rayess, M.E. Beyrouthy, L. Polito, M. Iriti, N. Martins, M. Martorell, A.O. Docea, W.N. Setzer, D. Calina, W.C. Cho, J. Sharifi-Rad, Lifestyle, oxidative stress, and antioxidants: back and forth in the pathophysiology of chronic diseases. Front. Physiol. 11 , 694 (2020). https://doi.org/10.3389/fphys.2020.00694
C.S. Yang, P. Luo, Z. Zeng, H. Wang, M. Malafa, N. Suh, Vitamin E and cancer prevention: studies with different forms of tocopherols and tocotrienols. Mol. Carcinog. 59 , 365–389 (2020). https://doi.org/10.1002/mc.23160
B.L. Tan, M.E. Norhaizan, W.P. Liew, H. Sulaiman Rahman, Antioxidant and oxidative stress: a mutual interplay in age-related diseases. Front. Pharmacol. 9 , 1162 (2018). https://doi.org/10.3389/fphar.2018.01162
Q. Jiang, Natural forms of vitamin E as effective agents for cancer prevention and therapy. Adv. Nutr. 8 , 850–867 (2017). https://doi.org/10.3945/an.117.016329
M. Wallert, M. Ziegler, X. Wang, A. Maluenda, X. Xu, M.L. Yap, R. Witt, C. Giles, S. Kluge, M. Hortmann, J. Zhang, P. Meikle, S. Lorkowski, Peter, α-Tocopherol preserves cardiac function by reducing oxidative stress and inflammation in ischemia/reperfusion injury. Redox Biol. 26 , 101292 (2019). https://doi.org/10.1016/j.redox.2019.101292
M. Ziegler, M. Wallert, S. Lorkowski, K. Peter, Cardiovascular and metabolic protection by vitamin E: A matter of treatment strategy? Antioxidants 29, 935. (2020). https://doi.org/10.3390/antiox9100935
M. Nandave, I. Mohanty, T.C. Nag, S.K. Ojha, R. Mittal, S. Kumari, D.S. Arya, Cardioprotective response to chronic administration of vitamin E in isoproterenol induced myocardial necrosis: hemodynamic, biochemical and ultrastructural studies. Indian J. Clin. Biochem. 22 , 22–28 (2017). https://doi.org/10.1007/BF02912876
A.T. Abdelhalim, N.M. Nur, S. Mansour, A. Ibrahim, Cardioprotective effect of vitamin E against myocardial infarction induced by isoprenaline in albino rats. Asian J. Pharm. Clin. Res. 11 , 273–276 (2018). https://doi.org/10.22159/ajpcr.2018.v11i6.24999
T. Schirinzi, G. Martella, P. Imbriani, G. Di Lazzaro, D. Franco, V.L. Colona, M. Alwardat, P. Sinibaldi Salimei, N.B. Mercuri, M. Pierantozzi, A. Pisani, Dietary vitamin E as a protective factor for Parkinson’s disease: clinical and experimental evidence. Front. Neurol. 10 , 148 (2019). https://doi.org/10.3389/fneur.2019.00148
M.C. Chang, S.G. Kwak, S.Y. Kwak, Effect of dietary vitamins C and E on the risk of Parkinson’s disease: a meta-analysis. Clin. Nutr. 40 , 3922–3930 (2021). https://doi.org/10.1016/j.clnu.2021.05.011
V. Buranasudja, D. Rani, A. Malla, K. Kobtrakul, S. Vimolmangkang, Insights into antioxidant activities and anti-skin-aging potential of callus extract from Centella asiatica (L). Sci. Rep. 11 , 13459 (2021). https://doi.org/10.1038/s41598-021-92958-7
C.C. Chu, Z.A. Azizul Hasan, C.P. Tan, K.L. Nyam, In vitro antiaging evaluation of sunscreen formulated from nanostructured lipid carrier and tocotrienol-rich fraction. J. Pharm. Sci. 110 , 3929–3936 (2021). https://doi.org/10.1016/j.xphs.2021.08.020
C.C. Chu, Z.A. Azizul Hasan, C.P. Tan, Nyam in vitro safety evaluation of sunscreen formulation from nanostructured lipid carriers using human cells and skin model. Toxicol. In Vitro. 84 , 105431 (2022). https://doi.org/10.1016/j.tiv.2022.105431
T.J. Stephens, M.L. Sigler, P.D. Hino, A.L. Moigne, L. Dispensa, A randomized, double-blind, placebo-controlled clinical trial evaluating an oral anti-aging skin care supplement for treating photodamaged skin. J. Clin. Aesthet. Dermatol. 9 , 25–32 (2016)
PubMed PubMed Central Google Scholar
E. Said, S. Mousa, M. Fawzi, N.A. Sabry, S. Farid, Combined effect of high-dose vitamin A, vitamin E supplementation, and zinc on adult patients with diabetes: a randomized trial. J. Adv. Res. 28 , 27–33 (2021). https://doi.org/10.1016/j.jare.2020.06.013
O. Asbaghi, B. Nazarian, M. Yousefi, J. Anjom-Shoae, H. Rasekhi, O. Sadeghi, Effect of vitamin E intake on glycemic control and insulin resistance in diabetic patients: an updated systematic review and meta-analysis of randomized controlled trials. Nutr. J. 22 , 1–22 (2023). https://doi.org/10.1186/s12937-023-00840-1
Y. Zhang, W. Jiang, Z. Xie, W. Wu, D. Zhang, Vitamin E and risk of age-related cataract: a meta-analysis. Public. Health Nutr. 18 , 2804–2814 (2015). https://doi.org/10.1017/S1368980014003115
E.D. Lewis, S.N. Meydani, D. Wu, Regulatory role of vitamin E in the immune system and inflammation. IUBMB Life. 71 , 487–494 (2019). https://doi.org/10.1002/iub.1976
G. Lee, S. Han, The role of vitamin E in immunity. Nutr. 10 , 1614 (2018). https://doi.org/10.3390/nu10111614
S. Sabetian, B.N. Jahromi, S. Vakili, S. Forouhari, S. Alipour, The effect of oral vitamin E on semen parameters and IVF outcome: A double-blinded randomized placebo-controlled clinical trial. Biomed Res. Int. 2021, 1 5588275 (2021)
N.A. Md Amin, S.H. Sheikh Abdul Kadir, A.H. Arshad, N. Abdul Aziz, N.A. Abdul Nasir, Ab latip, are vitamin E supplementation beneficial for female gynaecology health and diseases? Molecules. 27 , 1896 (2022). https://doi.org/10.3390/molecules27061896
M. Abbas Ali, S.C. Chew, Efficacy of exogenous natural antioxidants in stability of polyunsaturated oils under frying temperature. J. Food Meas. 17 , 408–429 (2023). https://doi.org/10.1007/s11694-022-01601-0
N. Xu, A.G. Shanbhag, B. Li, T. Angkuratipakorn, E.A. Decker, Impact of phospholipid-tocopherol combinations and enzyme-modified lecithin on the oxidative stability of bulk oil. J. Agric. Food Chem. 67 , 7954–7960 (2019). https://doi.org/10.1021/acs.jafc.9b02520
E. Tabee, S. Azadmard-Damirchi, M. Jägerstad, P.C. Dutta, Effects of α-tocopherol on oxidative stability and phytosterol oxidation during heating in some regular and high-oleic vegetable oils. J. Am. Oil Chem. Soc. 85 , 857–867 (2008). https://doi.org/10.1007/s11746-008-1274-2
K.H. Wagner, I. Elmadfa, Effects of tocopherols and their mixtures on the oxidative stability of olive oil and linseed oil under heating. Eur. J. Lipid Sci. Technol. 102 , 624–629 (2000). https://doi.org/10.1002/1438-9312(200010)102:10<624::AID-EJLT624>3.0.CO;2-I
L.M. Mazzaro, E.A. Koutsos, J.J. Williams, Current practices in aquatic animal supplementation. J. Zoo Aquar Res. 4 , 202–208 (2016). https://doi.org/10.19227/jzar.v4i4.202
A.F. Horn, N.S. Nielsen, C. Jacobsen, Additions of caffeic acid, ascorbyl palmitate or -tocopherol to fish oil-enriched energy bars affect lipid oxidation differently. Food Chem. 112 , 412–420 (2009)
A.B. Amaral, M.V. da Silva, S.C.S. Lannes, Lipid oxidation in meat: mechanisms and protective factors-a review. J. Food Sci. Technol. 38 , 1–15 (2018)
C. Tullberg, G. Vegarud, I. Undeland, Oxidation of marine oils during in vitro gastrointestinal digestion with human digestive fluids-role of oil origin, added tocopherols and lipolytic activity. Food Chem. 270 , 527–537 (2019). https://doi.org/10.1016/j.foodchem.2018.07.049
C.M. Seppanen, Q. Song, A. Saari, Csallany, The antioxidant functions of tocopherol and tocotrienol homologues in oils, fats, and food systems. J. Am. Oil Chem. Soc. 87 , 469–481 (2010). https://doi.org/10.1007/s11746-009-1526-9
L. Barbosa-Pereira, J.M. Cruz, R.A. Sendón, Rodríguez Bernaldo de Quirós, A. Ares, M. Castro-López, M.J. Abad, J. Maroto, P. Paseiro-Losada, Development of antioxidant active films containing tocopherols to extend the shelf life of fish. Food Control 31, 236–243 (2013)
D. Djenane, A. Sánchez-Escalante, J.A. Beltrán, P. Roncalés, Ability of α-tocopherol, taurine and rosemary, in combination with vitamin C, to increase the oxidative stability of beef steaks packaged in modified atmosphere. Food Chem. 76 , 407–415 (2002)
P.S. Melo, L.D.O.R. Arrivetti, S.M. de Alencar, L.H. Skibsted, Antioxidative and prooxidative effects in food lipids and synergism with α-tocopherol of açaí seed extracts and grape rachis extracts. Food Chem. 213 , 440–449 (2016). https://doi.org/10.1016/j.foodchem.2016.06.101
M. Cornelia, A. Aprilina, I. Triyanti, Effect of retort processing on low sodium instant noodle seasoning based on oil-in-water emulsions. Int. J. Food Stud. 10 , 150–160 (2021). https://doi.org/10.7455/ijfs/10.1.2021.a2
J.Y. Kim, S. Oh, B.R. Yi, M.J. Kim, J.H. Lee, Synergism of phosphatidylcholine on the antioxidant properties of α-tocopherol in corn oils under different relative humidity. Int. J. Food Sci. Technol. 50 , 1421–1428 (2015)
A. Maldonado, N. Riquelme, O. Muñoz-Fariña, O. García, C. Arancibia, Stability and bioaccessibility of α-tocopherol-enriched nanoemulsions containing different edible oils as carriers. LWT-Food Sci. Technol. 174 , 114419 (2023)
M.B. Let, C. Jacobsen, A.S. Meyer, Ascorbyl palmitate, gamma-tocopherol, and edta affect lipid oxidation in fish oil enriched salad dressing differently. J. Agric. Food Chem. 55 , 2369–2375 (2007). https://doi.org/10.1021/jf062675c
X. Zhang, Y. Shen, W. Prinyawiwatkul, J.M. King, Z. Xu, Comparison of the activities of hydrophilic anthocyanins and lipophilic tocols in black rice bran against lipid oxidation. Food Chem. 141 , 111–116 (2013). https://doi.org/10.1016/j.foodchem.2013.03.034
C. Agudelo-Cuartas, D. Granda-Restrepo, P.J.A. Sobral, H. Hernandez, W. Castro, Characterization of whey protein-based films incorporated with natamycin and nanoemulsion of α-tocopherol. Heliyon. 6 , e03809 (2020). https://doi.org/10.1016/j.heliyon.2020.e03809
X. Chen, D.S. Lee, X. Zhu, K.L. Yam, Release kinetics of tocopherol and quercetin from binary antioxidant controlled-release packaging films J. Agric. Food Chem. 60 , 3492–3497 (2012). https://doi.org/10.1021/jf2045813
B. Marcos, C. Sárraga, M. Castellari, F. Kappen, G. Schennink, J. Arnau, Development of biodegradable films with antioxidant properties based on polyesters containing α-tocopherol and olive leaf extract for food packaging applications. Food Packag. Shelf Life. 1 , 140–150 (2014). https://doi.org/10.1016/j.fpsl.2014.04.002
A. Gull, F.A. Masoodi, L. Masoodi, A. Gani, S. Muzaffar, Effect of sodium alginate coatings enriched with α-tocopherol on quality of fresh walnut kernels. Food Chem. Adv. 2 , 100169 (2023). https://doi.org/10.1016/j.focha.2022.100169
M.A. Khalili, A.A. Kenari, M. Rezaei, M.K. Mirzakhani, Antioxidant and antibacterial effects of vitamins C and E alone or a combination on microalgae ( Nannochloropsis oculata ) paste quality during cold storage. J. Aquat. Food Prod. Technol. 28 , 1051–1062 (2019). https://doi.org/10.1080/10498850.2019.1683108
S. Hosseini, Y. Ramezan, S.A. Arab, Comparative study on physicochemical characteristics and antioxidant activity of sumac ( Rhus coriaria L.), cumin ( Cuminum cyminum ), and caraway ( Carum carvil ) oils. J. Food Meas. 14 , 3175–3183 (2020). https://doi.org/10.1007/s11694-020-00561-7
M.A. Aboudzadeh, E. Mehravar, M. Fernandez, L. Lezama, R. Tomovska, Low-energy encapsulation of α–tocopherol using fully food grade oil-in-water microemulsions. ACS Omega. 3 , 10999–11008 (2018). https://doi.org/10.1021/acsomega.8b01272
D. Wang, M. Zhong, Y. Sun, L. Fang, Y. Sun, B. Qi, Y. Li, Effects of pH on ultrasonic-modified soybean lipophilic protein nanoemulsions with encapsulated vitamin E. LWT-Food Sci. Technol. 144 , 111240 (2021). https://doi.org/10.1016/j.lwt.2021.111240
Z. Zhang, L. Zhang, Q. Xie, L. Che, Effect of accelerated storage on fatty acids, thermal properties and bioactive compounds of kenaf seed oil. J. Food Sci. 0 , 1–7 (2019). https://doi.org/10.1111/1750-3841.14653
P.G. Ergönül, O. Köseoğlu, Changes in α-, β-, γ- and δ-tocopherol contents of mostly consumed vegetable oils during refining process. CyTA-J. Food. 12 , 199–202 (2013). https://doi.org/10.1080/19476337.2013.821672
L. Cerretani, M.J. Lerma-García, J.M. Herrero-Martínez, T. Gallina-Toschi, E.F. Simó-Alfonso, Determination of tocopherols and tocotrienols in vegetable oils by nanoliquid chromatography with ultraviolet-visible detection using a silica monolithic column. J. Agric. Food Chem. 58 , 757–761 (2010). https://doi.org/10.1021/jf9031537
K. Nurkhuzaiah, A.S. Babji, W.I. Wan Rosli, S.P. Foo, Tocopherol and tocotrienol contents of chicken nuggets blended with red palm oils before and after frying. J. Oil Palm. Res. 27 , 83–90 (2015)
Google Scholar
T. Tuersuntuoheti, Z. Wang, Y. Zheng, S. Wang, Z. Wang, Y. Wu, S. Liang, X. Li, M. Zhang, Study on the shelf life and quality characteristics of highland barley fresh noodles as affected by microwave treatment and food preservatives. Food Sci. Nutri. 7 , 2958–2967 (2019). https://doi.org/10.1002/fsn3.1151
Download references
Acknowledgements
No funding was received to assist with the preparation of this manuscript.
Author information
Authors and affiliations.
School of Pharmacy, Faculty of Health and Medical Sciences, Taylor’s University, Subang Jaya, 47500, Malaysia
Chee Chin Chu
School of Foundation Studies, Xiamen University Malaysia Campus, Bandar Serenia, Sepang, 43900, Selangor, Malaysia
Sook Chin Chew
School of Chemical and Biomedical Engineering, Nanyang Technological University, 62 Nanyang Drive, Singapore, 637459, Singapore
Wen Ching Liew
Department of Food Science and Nutrition, Faculty of Applied Sciences, UCSI University, Kuala Lumpur, 56000, Malaysia
Kar Lin Nyam
You can also search for this author in PubMed Google Scholar
Contributions
Conceptualization and design: Chee Chin Chu, Sook Chin Chew, and Kar Lin Nyam. Writing-original draft and editing: Chee Chin Chu. Writing-review and editing: Sook Chin Chew, Wen Ching Liew, and Kar Lin Nyam. All authors read and approved the final manuscript.
Corresponding author
Correspondence to Kar Lin Nyam .
Ethics declarations
Conflict of interest.
The authors declare no conflict of interest.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Chu, C.C., Chew, S.C., Liew, W.C. et al. Review article vitamin E: a multi-functional ingredient for health enhancement and food preservation. Food Measure 17 , 6144–6156 (2023). https://doi.org/10.1007/s11694-023-02042-z
Download citation
Received : 21 April 2023
Accepted : 28 June 2023
Published : 23 August 2023
Issue Date : December 2023
DOI : https://doi.org/10.1007/s11694-023-02042-z
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Anti-inflammation
- Cardioprotection
- Neuroprotection
- Lipid oxidation
- Food stabiliser
- Find a journal
- Publish with us
- Track your research

Apr 01, 2019
2.89k likes | 7.15k Views
http://www.thedailygreen.com/healthy-eating/eat-safe/top-sources-vitamin-E-44111408. http://science.kqed.org/quest/2011/10/14/vitamin-e-supplements-increase-prostate-cancer-risk/. Vitamin E. Corey Crowe, Brittany Shannon, Amanda Sperry, and Jocelyn Tomsic. Overview:. Composition
Share Presentation
- severe selenium
- which vitamin e
- com picview
- high levels
- digestive system images photo

Presentation Transcript
http://www.thedailygreen.com/healthy-eating/eat-safe/top-sources-vitamin-E-44111408 http://www.thedailygreen.com/healthy-eating/eat-safe/top-sources-vitamin-E-44111408 http://science.kqed.org/quest/2011/10/14/vitamin-e-supplements-increase-prostate-cancer-risk/ Vitamin E Corey Crowe, Brittany Shannon, Amanda Sperry, and Jocelyn Tomsic
Overview: • Composition • Food Sources (plant/animal) • Digestion & Absorption • Transport & Metabolism • Storage & Excretion • Functions • Interactions with other nutrients/medications • Deficiencies • Toxicity • Vitamin E and Diseases
Vitamin E Composition • Composed of 8 compounds (vitamers) divided into two classes: • Tocopherols: • which have saturated side chains with 16 carbons • Tocotrienols: • which have unsaturated side chains with 16 carbons • Each class is composed of 4 vitamers that differ in the # and location of methyl groups on the chromanol ring.
Vitamin E Composition http://lipidlibrary.aocs.org/topics/tocopherols/index.htm • Only the alpha-tocopherol has biological activity and can meet the body’s requirement for the vitamin.
Vitamin E Classification • Is part of the fat-soluble vitamin family (A,D,E,K) • Is also an important antioxidant (A,C,E) • Like the other fat-soluble vitamins, vitamin E, is very susceptible to destruction during food preparation and storage. • Tocopherols can become oxidized with long-term exposure to air. • Exposure to light and heat can also lead to its increased destruction.
DietaryVitamin http://www.fitnessrxwomen.com/nutrition/healthy-eating-tips/improve-health-performance-with-vitamin-e/
Plant Sources Food Sources • Vegetable Oil • Nuts • Seeds • Avocados • Spinach • Kale Animal Sources • Concentrated fats of meats • Found in various forms however, is predominantly found in plant sources, especially the oils from plants. • It is recommended getting proper amounts of vitamin E from mostly food sources rather than supplements. http://ljayhealth.wordpress.com/2012/02/23/health-benefits-of-spinach-2/
Supplementation Sources • Vitamin E is present in almost every multivitamin pill. • Alpha-tocopherol in dietary supplements and fortified foods is often esterified to prolong its shelf life while protecting its antioxidant properties. • People need approximately 50% more IU of synthetic alpha tocopherol from dietary supplements and fortified foods to obtain the same amount of the nutrient when compared to the natural form. http://www.ehow.com/how_4542_absorb-vitamin-e.html http://ods.od.nih.gov/factsheets/VITAMINE-HealthProfessional/
Digestion & Absorption http://cnx.org/content/m44742/latest/
Digestion • Tocopherols are found free in foods, whereas the tocotrienols are found esterified and must be hydrolyzed before absorption. • Pancreatic esterase and duodenal mucosal esterase function in the lumen and/or at the brush border membranes of enterocytes to hydrolyze tocotrienols and synthetic ester alpha-tocopherols for absorption.
Absorption • Vitamin E is primarily absorbed in the jejunum by passive diffusion. • Diffused like lipids using bile salts for emulsification, solubilization, and micelle formation • Uptake of vitamin E into cells occurs as lipoproteins are taken up by body tissues and can occur in several ways: • Through receptor-mediated uptake of LDLs • Through lipoprotein lipase-mediated hydrolysis of chylomicrons and VLDLs • Through HDL-mediated nutrient delivery http://www.smscs.com/picview.php?title=digestive+system+images&photo=http%3A%2F%2Fwww.macroevolution.net%2Fimages%2Fhuman-digestive-system-225-401-12.jpg
Transport &Metabolism
Transport • In the enterocyte, absorbed tocopherols are incorporated into chylomicrons for transportation through the lymph and then into circulation. • During transport in the chylomicrons, tocopherol is transferred among the other lipoproteins, including HDLs and LDLs. • LDLs posses the highest concentrations of vitamin E. http://www.sigmaaldrich.com/life-science/metabolomics/enzyme-explorer/learning-center/plasma-blood-protein/lipoprotein-function.html
Metabolism • Chylomicron remnants deliver vitamin E to the liver to be metabolized. • However only RRR alpha-tocopherol is incorporated into VLDL for recirculation back into the blood to be transported to other tissues. http://www.theheart.org/fr/documents/infoSite/infocus/infocus.html
Storage &Excretion
Storage • There is no single storage organ for vitamin E. • The liver, lungs, heart, muscles, adrenal glands, spleen, and the brain are the major tissues that take up small amounts of vitamin E. • The largest amount (over 90%) occurs in concentrated unesterified form in fat droplets in adipose tissue. • The vitamin E in adipose tissue increases linearly with the intake of it, however the release of it from adipose tissue is much slower even during times of low intake.
Excretion • After the liver has absorbed the alpha-tocopherol form of vitamin E and absorption in the small intestine has occurred, the liver secretes only alpha-tocopherol via the hepatic alpha-tocopherol transfer protein. • The liver will metabolize and excrete other forms of vitamin E. • Begins with a hydroxylation reaction that requires Cytochrome P-450. • Then a series of reactions within Beta -oxidation occurs to shorten vitamin E’s side chains. • The end product results in a group of carboxyethyl hydroxychroman • For urinary excretion this carboxyethyl hydroxychroman combines with sulfate to be eliminated.
http://novenamaternity.com/ingredients/ Antioxidant Function http://www.wesleyvirgin.com/give-your-body-the-gift-of-kale/
Antioxidant Role • The main function of vitamin E: • As an antioxidant, it helps to maintain membrane integrity within cells. • The mechanism by which vitamin E protects the membranes from destruction is through its ability to prevent oxidation of unsaturated FA contained in the phospholipids of the membrane. • The lungs, brain, and RBCs are the most vulnerable AND are the most susceptible to oxidation. http://face-and-emotion.com/dataface/anatomy/brain-cranium.jsp http://www.odiadoctors.com/respiratory-functions-lungs/
Antioxidant Role • As an antioxidant, vitamin E can destroy singlet molecular oxygen and stop reactions involving free radicals. • Its ability to diminish free radicals is related to the hydroxyl group on the chromane ring portion of the vitamin. • The hydroxyl group gives up hydrogen and therefore inactivates the free radical. • Not all tocopherols are equal in their ability to diminish free radicals. • Alpha-tocopherol was found to be more effective than beta-tocopherol, gamma-tocopherol, or sigma-tocopherol.
http://trialx.com/curebyte/2011/07/06/immune-function-photos-and-related-clinical-trials/ http://trialx.com/curebyte/2011/07/06/immune-function-photos-and-related-clinical-trials/ Immune Function
Immune Response • Needed to boost the body’s immune system so that it can fight off invading bacteria and viruses. • Vitamin E can partially overcome immunosuppression of substances like: • High levels of PUFA • Severe selenium deficiency • High levels of vitamin C can protect tissue levels of vitamin E and may indirectly contribute to the immunoenhancement by vitamin E. http://healthy-proteins.blogspot.com/2012/11/optimize-your-immune-system-naturally.html
Interactions with Other Nutrients
How Does Vitamin E Get Along With…? • Selenium • Vitamin C • Dietary polyunsaturated FA • Other fat-soluble vitamins (especially Vitamin K)
Vitamin E and Selenium • Selenium has roles in reproduction, thyroid hormone metabolism, DNA synthesis, and protection from oxidative damage and infection. • The actions of both nutrients complement each other • Higher concentrations of one can reduce the effects of lower concentration of the other, creating a counterbalancing body system. http://healthfreedoms.org/2009/05/27/selenium-in-diet-overview/
Vitamin E and Vitamin C • Similar to vitamin E’s relationship with Selenium, Vitamin C also complements vitamin E. • Though vitamin E is an antioxidant, it can become oxidized when it interacts with a free radical, therefore creating more oxidative damage. • But vitamin C can interact with oxidized vitamin E, reducing free radicals and regenerating the benefits of vitamin E. https://az.naturesgardendelivered.com/blog/increase-your-vitamin-c-intake-and-ward-off-seasonal-allergies/ http://reebokcrossfit5thave.com/tag/vitamin-c/
Vitamin E and Polyunsaturated Fatty Acids • Vitamin E requirements increase or decrease as the degree of unsaturated fatty acids in body tissues rise or fall, respectfully. • Body tissue lipids are in turn influenced by dietary lipid intake. • Foods high in polyunsaturated FA also tend to be relatively good sources of vitamin E. http://www.beefitzxt.com/main/products
Vitamin E and Fat-soluble Vitamins • High intake of vitamin E can interfere with other fat-soluble vitamins. • Vitamin E inhibits beta-carotene absorption and its metabolism in the intestine. • Impairs vitamin K absorption and its metabolism. • The effects of vitamin E may increase the risk for bleeding secondary to the interference of vitamin K’s ability to clot blood • Vitamin E is also important in helping your body make red blood cells, and it helps the body to use vitamin K. http://www.hollandandbarrett.com/pages/categories.asp?cid=70
Possible Interactions with Medications: -Antidepressant medications (ex: Norpramin) -Antipsychotic medications (ex: chlorpromazine) -AZT (A medication used to treat HIV and AIDS) -Bile acid sequestrants (ex: Cholestyramine, cholestipol) -Statins (ex: Niacin and Zocor) • -Chemotherapy drugs (ex: chlorambucil) • -Anticoagulant and antiplatelet medications • -Chemotherapy and radiotherapy • -Aspirin • -Orlistat • -Beta-blockers (ex: Propranolol)
Deficiencies and Symptoms
Deficiencies • Deficiencies of vitamin E are rare in humans, but many people have slightly low levels. • Since the digestive tract requires fat to absorb vitamin E, people with fat-malabsorption disorders (for example steatorrhea or cystic fibrosis) are more likely to become deficient rather than people without such disorders. • Deficiencies that last a long time could cause liver and kidney problems. http://www.123rf.com/photo_7732679_feet-on-a-bathroom-scale-with-the-word-help-on-the-screen-isolated--includes-clipping-path.html http://immunetreeblog.com/extreme-fatigue-what-causes-extreme-tiredness/
Symptoms • Myopathy (skeletal muscle pain) and Weakness • Ceroid Pigment Accumulation (fat accumulation) • Hemolytic Anemia • Degenerative Neuropathy • Ataxia • Loss of Vibratory Sense • Loss of Coordination of Limbs http://myweb.tiscali.co.uk/ataxia.pages/
Toxicity http://www.newautism.com/heavy-metal-toxicity/158/
Problems Associated with Toxicity • Vitamin E appears to be one of the least toxic vitamins. • It is not mutagenic, carcinogenic, or teratogenic • Oral supplementations of vitamin E do not result in serious side effects • Mild gastrointestinal problems may occur with intake between 200 and 800 mg. • Due to the increased tendency for bleeding, because of antiplatelet effects and/or abnormal blood clotting, a Tolerable Upper Intake of 1,000 mg/day of alpha-tocopherol has been suggested.
Toxicity Symptoms • Gastrointestinal Distress • Nausea • Diarrhea • Flatulence • Impaired Blood Coagulation • Increased Severity of Respiratory Infections • Muscle Weakness • Fatigue • Double Vision http://news.softpedia.com/news/Common-Antibiotic-Effective-Against-Bloating-and-Flatulence-18165.shtml http://medicalmarijuanalabprojectthursdayam.wikispaces.com/file/detail/nausea.gif/386256408
Vitamin E and Disease
Vitamin E & Heart Disease • Results have not shown that vitamin E helps lower the risk of Heart Disease • One of the largest studies, the Heart Outcomes Prevention Evaluation (HOPE) trial, found that taking 400 IU of vitamin E (d-alpha-tocopherol) daily did not lower the number of heart attacks, strokes, or deaths from heart disease among men and women who already had heart disease or were at high risk for it. • What about in healthy people who were at low risk for heart disease? • Two large trials also found no protection from vitamin E. In one -- the Physicians' Health Study II -- vitamin E was associated with a higher risk of stroke http://health.allrefer.com/pictures-images/vitamin-e-and-heart-disease.html
Vitamin E and Cancer • There is no concrete evidence to support the fact that Vitamin E can cure/prevent cancer • There is a small amount of evidence suggesting that taking vitamin E along with vitamin A and vitamin C, or as part of a multivitamin would help protect people who had colorectal adenomas, a precursor for colon cancer. • There are several studies showing that intake of multiple vitamin supplements, including vitamin E can lower prostate cancer. • Vitamin E has some positive effects on cancer treatment • A study of 108 people taking chemotherapy drug cisplatin found that taking a vitamin E supplement during and as long as three months after treatment reduced nerve damage from the drug. • Some doctors worry though that large doses of antioxidants could interfere with chemotherapy medications.
Vitamin E and Eye Health • Vitamin E (400 IU) combined with other antioxidants including zinc, beta-carotene and vitamin C protect against developing macular degeneration (AMD). • AMD is the leading cause of legal blindness in people over 55 in the United States. • People with advanced AMD seem to benefit the most from this treatment. • Vitamins E and C can also help to treat uveitis, or inflammation of the uvea. This is the middle layer of the eye. • These vitamins can help people with inflammation and help them to have clearer vision. http://www.lookupinfo.org/easy_read_information/easy_read_eye_health_information.aspx
Vitamin E and Photodermatitis • Photodermatitis is a condition where an individual has an allergic reaction to UV sun rays. • An 8 day study which compared treatment with vitamins C and E to a placebo found that people who took the vitamins became significantly less sensitive to the sun. • Another study lasting for 50 days showed a protective effect from the vitamin C and E treatment. http://www.abc.net.au/news/2011-10-07/uv-rays-more-damaging-than-thought/3335828
Vitamin E and Dementia • Studies have documented low levels of vitamin E in patients with Alzheimer's disease. • A placebo-controlled trial found that supplementation with 2,000 IU of synthetic alpha-tocopherol daily for two years significantly slowed progression of Alzheimer's dementia. • Vascular dementia (dementia resulting from strokes) • A study examining risk factors for vascular dementia in elderly Japanese-American men found that supplemental vitamin E and vitamin C intake was associated with a significantly decreased risk of vascular and other types of dementia but not Alzheimer's dementia. • Among those without dementia, vitamin E supplement use was associated with better scores on cognitive tests.
Take Home Points… To be able to discuss the importance of Vitamin E in our diet. To understand the digestion, absorption, transportation and excretion of Vitamin E. To be able to identify the major food sources of Vitamin E. To understand the effects of Vitamin E on certain diseases.
Questions? http://www.inc.com/tom-searcy/5-great-questions-ceos-ask-customers.html
References • National Institute of Health: Office of Dietary Supplements. Vitamin E. Reviewed: June 05, 2013. Available at http://ods.od.nih.gov/factsheets/VitaminE-HealthProfessional/#h2. Accessed November 06, 2013. • Ehrlich S. Vitamin E. University of Maryland Medical Center Complimentary and Alternative Medicine Guide. http://umm.edu/health/medical/altmed/supplement/vitamin-e Published Jan 15, 2012. Last Updated May 7, 2013. Assessed Nov 10, 2013. • Micronutrient Information Center: Vitamin E. Linus Pauling Institute, Oregon State University, Corvallis, OR. Available at: http://lpi.oregonstate.edu/infocenter/vitamins/vitaminE/. Accessed November 13, 2013. • Bendich A. Vitamin E and immune functions. Basic Life Sci. 1988;49:615-20. • Anderson KE. Comparison of fatty acid, cholesterol, vitamin A and E composition, and trans fats in eggs from brown and white egg strains that were molted or nonmolted. Poult Sci. 2013;92(12):3259-65. • Dietary Facts Sheet: Selenium. National Institutes of Health: Office of Dietary Supplements. Available at: http://ods.od.nih.gov/factsheets/Selenium-HealthProfessional/. Accessed October 9, 2013. • Gropper, SS, Smith. Advanced Nutrition and Human Metabolism, 6th Edition, Wadsworth/Cengage Learning, 2012.
- More by User

Zenith Nutrition Vitamin E
Zenith Nutrition, a division of Medizen Labs, is a leading manufacturer of wellness products in India. The company is focusing primarily on growing Nutritional supplements and dietary supplements space globally. The Company utilizes its industry leading R&D and technical capabilities to produce superior research based formulations that optimize the nutritional value and performance for its customers’. The Company also leverages its knowledge and expertise to complement its products with value-added technical services and continuous customer support. The Company’s specialised product and service offerings combined with its manufacturing flexibility enables it to create customized value added solutions that address specific customer needs. Zenith Nutrition’s broad knowledge across a wide variety of competencies allows the Company to provide condition specific wellness products to meet customer’s needs./nZenith Nutrition’s products are unique in their use of synergistic ingredient formulations which deliver outstanding potency and therefore greater efficacy and a better value to the customers Zenith Nutrition runs on passion, innovation and highest quality for healthier world. For more than five years, Zenith Nutrition’s has been proactively contributed to growth and continues success of health care industry by passion, innovation, and most important, customers satisfaction.
332 views • 7 slides

Vista Nutrition Vitamin E
Vitamin E is found naturally in some foods, added to others, and available as a dietary supplement. "Vitamin E" is the collective name for a group of fat-soluble compounds with distinctive antioxidant activities Naturally occurring vitamin E exists in eight chemical forms (alpha-, beta-, gamma-, and delta-tocopherol and alpha-, beta-, gamma-, and delta-tocotrienol) that have varying levels of biological activity [1]. Alpha- (or α-) tocopherol is the only form that is recognized to meet human requirements. The term "Vitamin E" refers to a family of eight related, lipid-soluble, antioxidant compounds widely distributed in plants. The tocopherol and tocotrienol subfamilies are each composed of alpha, beta, gamma and delta, and all possess unique biological effects. Different ratios of these compounds are found in anatomically different parts of a plant. For example, the green parts of a plant contain mostly alpha tocopherol and the seed germ and bran contain mostly tocotrienols.
335 views • 7 slides

VITAMIN E. The term vitamin E describes a family of 8 antioxidants, 4 tocopherols ( a , b , g , & d ) and 4 tocotrienols. a -tocopherol is the active form of vitamin E in the human body. FUNCTIONS.
1.9k views • 29 slides

Vitamin E. By Lauren Gervase. Vitamin E. Vitamin E is also known as: Alpha-tocopherol, tocopherol, tocotrienol. Tocopherol Chemical Composition. The term tocol is the trivial designation for 2-methyl-2-(4,8,12-trimethyltridecyl)chroman-6-ol (I, R 1 = R 2 = R 3 = H)
1.42k views • 15 slides

Vitamin E - Tocopherol
Vitamin E - Tocopherol. Functions Antioxidant- reduces risk of heart disease, stroke, cancer Improves absorption of vitamin A Destroys free radicals, reduces effects of ageing Protects blood cells. Effects of deficiency Deficiency is rare Linked to lung cancer in smokers
930 views • 3 slides

Fat Soluble Vitamins Vitamin A Vitamin E Vitamin D Vitamin K
Fat Soluble Vitamins Vitamin A Vitamin E Vitamin D Vitamin K. Vitamin A. RETINOIDS. The retinoids : a family of molecules that are related to retinol (vitamin A) ------------------------------------- The term retinoids includes
1.51k views • 58 slides

LIPID SOLUBLE VITAMINS : s tructure, properties, biological role, nature sources and day necessities of vitamins E, K, F. Vitamin E. Tocopherols and tocotrienols. Antisterile. Group of tocopherols and tocotrienols Most active – alpha-tocopherol. Biological role
733 views • 43 slides

Importance of Vitamin E Supplements
Vitamin E is just as important as any other nutrient, like Vitamin A, B, C and D. It is crucial for us, owing to the many health benefits it provides. The many uses of Vitamin E, makes it important that this nutrient should be ingested every day for smooth functioning of the body. Having powerful antioxidant properties is one of the most unique characteristics of Vitamin E.
569 views • 11 slides

Treat Vitamin E Deficiency with Vitamin E Supplement
Vitamin E is required by the body to keep the immune system strong to fight against viruses and bacteria.
392 views • 8 slides

tasmanhealth.co.nz | Solgar Vitamin E 400IU
Vitamin E is the body’s primary vitamin antioxidant. This fat soluble vitamin nourishes the skin, cardiovascular health, and immune defences with its potent antioxidant mechanisms. Vitamin E works by scavenging destructive free radicals that causes oxidative stress in the cells, leading to premature cell ageing and death. Solgar Vitamin E-400 provides natural, plant-based Vitamin E. visit us: http://www.tasmanhealth.co.nz/solgar-vitamin-e-400iu/ for more details!!
139 views • 4 slides

NATURAL VITAMIN E SQUALANE SERUM
If you want to keep your skin well hydrated and protected for a younger and healthier appearance, then use Savarnas Mantra Natural Vitamin E Squalane Serum. It has vitamins and minerals that will act as the first line of defense against all the external damaging factors. It is best suited to keep the moisture levels of your skin high and reinforce its protective and regenerative properties. With a combination of Squalane and Vitamin E, the serum provides moisture and essential nutrients to protect, revive and reinvigorate the skin. Squalane acts as a pure and natural moisturizer, while Vitamin E is a powerful antioxidant. It is a skin-protecting nutrient and ensures anti-aging.
28 views • 2 slides

If you want to keep your skin well hydrated and protected for a younger and healthier appearance, then use Savarnas Mantra Natural Vitamin E Squalane Serum. It has vitamins and minerals that will act as the first line of defense against all the external damaging factors. It is best suited to keep the moisture levels of your skin high and reinforce its protective and regenerative properties. With a combination of Squalane and Vitamin E, the serum provides moisture and essential nutrients to protect, revive and reinvigorate the skin. Squalane acts as a pure and natural moisturizer, while Vitamin E is a powerful antioxidant. It is a skin-protecting nutrient and ensures anti-aging. Benefits The serum will smooth your skin and soften the wrinkles on your face. It will further moisturize the dry and irritated skin. It ensures to revitalize the damaged skin and stimulates healing of the skin. The serum is an effective anti-antioxidant. It gives healthy protection to the skin Check out the Product: https://savarnasmantra.com/collections/serums/products/natural-vitamin-e-squalane-serum-30-ml
26 views • 2 slides

Vitamin E Tablets
We all know that vitamin E has the high sales over the entire world as it is considered as master antioxidant. EAnnatto tocotrienols has great antioxidant properties. USA army is also giving these supplements to their soldiers when they are in high radiation areas. If you are also looking for best vitamin E tablets online then you can take EAnnatto tocotrienols. For more information visit their website:https://www.eannatto.ca/product/eannatto-deltagold-vitamin-e-buy-online/
47 views • 2 slides

Buy Online Vitamin E capsules
Vitamin E Tocotrienols are part of vitamin E family. Vitamin E is a family of eight separate but related molecules including four Tocopherol (delta, gamma, alpha and beta) and four tocotrienols (also delta, gamma, alpha and beta). Tocotrienols have amazing antioxidant properties of the annatto. EAnnatto Tocotrienols DeltaGold tablets has anti cancer properties. It kills cancer cells along with cancer making cells. For more information visit our website:-https://www.astervedahealthcare.com/product/eannatto-deltagold/
106 views • 10 slides

Vitamin D, E & K
Fat soluble vitamins. Vitamin D, E & K. Vitamin D. Vitamin D. The term “Vitamin D” refers to a family of related compounds biosynthesized from cholesterol and ergosterol .
609 views • 43 slides

Vitamin E Tocotrienols
Vitamin E Tocotrienols extensively increase immunity or to reduce disease in our body. Vitamin E is the fat-soluble, widely distributed in the foods and can even be stored in our bodies.
46 views • 1 slides

Vitamin E Market
Vitamin E is fat soluble antioxidants that will protect the cell membrane from reactive oxygen species. It is found in many food ingredients such as vegetable oil, cereal, meat, poultry eggs, fruits, vegetables and wheat germ oil. Vitamin E deficiency is found in people with genetic disorder or in premature infants.
73 views • 6 slides

Vitamin e market
Vitamin E is fat soluble antioxidants that will protect the cell membrane from reactive oxygen species. It is found in many food ingredients such as vegetable oil, cereal, meat, poultry eggs, fruits, vegetables and wheat germ oil.
78 views • 6 slides

Vitamin E is a group of 8 fat soluble compounds that include four tocopherols and four tocotrienols. It is chemically k/a tocopherol. (Greek: tocos=childbirth , piro=to bear and ol=alcohol) Vitamin E is the name given to group of tocopherols and tocotrienols
630 views • 19 slides

Vitamin E Oil for Hair?
The modern developed world offers great options and opportunities to thrive in life. However, the hustle and bustle of today's world come up with a lot of side-effects. Some of those are Source: https://pureethics.mystrikingly.com/blog/vitamin-e-oil-for-hair
75 views • 6 slides

Vitamin C & E Serum
A glass of orange juice rounds out a perfect breakfast. Similarly, a Vitamin C & E serum rounds out a great skincare regimen. If you're not using a Vitamin C & E serum every morning, here are five reasons why you should start: Please visit :https://soonskincare.com/products/phoenix-15-vitamin-c-e-serum
58 views • 2 slides

Looking for info on the benefits of vitamin E? What to know before taking the supplement
A merica's obsession with low-fat diets has contributed to otherwise healthy people being deficient in some healthy fats . These fats are necessary for strong immunity , healthy brain function, hormone balance and antioxidant power.
Research shows that vitamin E is one such nutrient that a whopping 88.5% of Americans aren't getting enough of naturally. That's especially worrisome considering some controversy exists in the medical community regarding the safety of supplementing vitamin E.
Though concerning levels of vitamin E deficiencies are rare in people who eat a healthy diet , they are more common among people who avoid healthy fats, those with digestive disorders and in people who can't absorb fat properly such as individuals suffering from pancreatitis , celiac disease or cystic fibrosis.
Start the day smarter. Get all the news you need in your inbox each morning.
What is vitamin E good for?
Vitamin E is a fat-soluble nutrient that exists in several forms and has many health benefits including improved immune, skin and eye health. It's also a powerful antioxidant "and may protect your cells from the effects of free radicals , which may play a role in contributing to heart disease and cancer," says Lisa Young, PhD, an adjunct professor of nutrition at New York University and author of "Finally Full, Finally Slim."
Vitamin E also plays an important role in the body's immune system "in keeping blood vessels working at their best," says Kate Zeratsky, a registered dietitian nutritionist at Mayo Clinic in Rochester, MN.
Josh Redd, NMD, the founder of RedRiver Health and Wellness and author of "The Truth About Low Thyroid," says that vitamin E plays a part "in helping patients with autoimmune disorders by dampening autoimmune expression and regulating inflammation."
And while there is still much that remains unknown about other vitamin-E related health benefits, some research suggests the nutrient may also help preserve brain health against cognitive decline and dementia, and may reduce symptoms of anxiety and depression.
"There also seems to be some improvement in the pain associated with menstruation in some women," adds Zeratsky.
What are the symptoms of vitamin E deficiency?
Signs of vitamin E deficiency include:
- impaired vision
- ataxia (loss of bodily control)
- diminished immune function
- and nerve pain or damage.
Are you supposed to take vitamin E every day?
Though you should be able to get all the vitamin E you need naturally from a healthy diet, some people choose to supplement the nutrient through a pill or multivitamin. The National Institutes of Health Office of Dietary Supplements recommends for anyone 14 years and older, including pregnant women, to get only 15 milligrams of the nutrient daily. Nursing mothers should get 19 milligrams.
Unlike most nutrients, however, vitamin E supplementation "should be discussed with your health care provider as some studies suggest certain conditions and doses may have worse outcomes," cautions Zeratsky.
Indeed, Sarah Booth, PhD, center director of the Jean Mayer USDA Human Nutrition Research Center on Aging at Tufts University, says there is "considerable controversy regarding supplement vitamin E use," due to some studies that have connected very high rates of vitamin E supplementation with prostate cancer or increased risk of early death. "The data are very inconsistent, however," Booth explains. "In general, there is little evidence for increased mortality risk when vitamin E supplements are taken by healthy individuals."
When supplementing, check the label for the safest form of the nutrient. "Find a vitamin E supplement that contains d-alpha tocopherol and one that is not synthesized but instead derived from plants," recommends Redd.
Booth also recommends the alpha tocopherol form of vitamin E and says one can get plenty of that type naturally from a well-rounded diet. The most abundant natural source of the nutrient is wheatgerm oil (found in some cereals), followed by sunflower seeds, vegetable oils , peanut butter , almonds , hazelnuts, peanuts, and fruits and vegetables such as asparagus, spinach, broccoli, kiwi, mangoes and tomatoes. Booth adds: "Vitamin E consumed in the diet is considered safe."
This article originally appeared on USA TODAY: Looking for info on the benefits of vitamin E? What to know before taking the supplement

Disclaimer » Advertising
- HealthyChildren.org
Study Design
Participants, rickets screening procedures, laboratory methods and radiographic interpretations, case definition, statistical analysis, maternal and infant characteristics, effect of maternal vitamin d supplementation on biochemical rickets, subgroup analyses, infant bone biomarkers, radiographically confirmed rickets, conclusions, acknowledgments, maternal vitamin d supplementation and infantile rickets: secondary analysis of a randomized trial.
FUNDING: This work was supported in part by the Bill & Melinda Gates Foundation (OPP1066764). Under the grant conditions of the Foundation, a Creative Commons Attribution 4.0 Generic License has already been assigned to the Author Accepted Manuscript version that might arise from this submission. Dr Lautatzis received salary support from the Canadian Pediatric Endocrine Group Fellowship Program and CIHR Canada Graduate Scholarship. The funding agencies were not involved in the design, implementation, analysis, or interpretation of the data.
CONFLICT OF INTEREST DISCLOSURES: There are no conflicts of interest to disclose.
- Split-Screen
- Article contents
- Figures & tables
- Supplementary Data
- Peer Review
- CME Quiz Close Quiz
- Open the PDF for in another window
- Get Permissions
- Cite Icon Cite
- Search Site
Maria-Elena Lautatzis , Farhana K. Keya , Abdullah Al Mahmud , Ulaina Tariq , Carol Lam , Shaun K. Morris , Jennifer Stimec , Stanley Zlotkin , Tahmeed Ahmed , Jennifer Harrington , Daniel E. Roth; Maternal Vitamin D Supplementation and Infantile Rickets: Secondary Analysis of a Randomized Trial. Pediatrics 2024; e2023063263. 10.1542/peds.2023-063263
Download citation file:
- Ris (Zotero)
- Reference Manager
The role of maternal vitamin D supplementation in the prevention of infantile rickets is unknown, particularly in low- and middle-income countries without routine infant vitamin D supplementation. Through secondary analysis of a randomized, placebo-controlled trial in Bangladesh, we examined the dose-ranging effects of maternal vitamin D supplementation on the risk of biochemical rickets at 6 to 12 months of age.
Pregnant women ( n = 1300) were randomized into 5 groups: placebo, or vitamin D 4200 IU/week, 16 800 IU/week, or 28 000 IU/week from second trimester to delivery and placebo until 6 months postpartum; or 28 000 IU/week prenatally and until 6 months postpartum. Infants underwent biochemical rickets screening from 6 to 12 months of age ( n = 790). Relative risks (RR) and 95% confidence intervals (95% CI) of biochemical rickets were estimated for each group versus placebo.
Overall, 39/790 (4.9%) infants had biochemical rickets. Prevalence was highest in the placebo group (7.8%), and the risk was significantly lower among infants whose mothers received combined prenatal and postpartum vitamin D at 28 000 IU/week (1.3%; RR, 0.16; 95% CI, 0.03–0.72). Risks among infants whose mothers received only prenatal supplementation (4200 IU, 16 800 IU, 28 000 IU weekly) were not significantly different from placebo: 3.8% (RR, 0.48; 95% CI, 0.19–1.22), 5.8% (RR, 0.74; 95% CI, 0.33–1.69), and 5.7% (RR, 0.73; 95% CI, 0.32–1.65), respectively.
Maternal vitamin D supplementation (28 000 IU/week) during the third trimester of pregnancy until 6 months postpartum reduced the risk of infantile biochemical rickets. Further research is needed to define optimal postpartum supplementation dosing during lactation.
Maternal vitamin D supplementation during pregnancy and lactation modifies infant vitamin D status, but its effects on the risk of infantile rickets have not previously been established.
High-dose maternal vitamin D supplementation during the third trimester of pregnancy and up to 6-months postpartum reduced the risk of infantile rickets in Bangladesh. Maternal postpartum vitamin D supplementation may be an alternative to direct infant supplementation for rickets prevention.
Nutritional rickets is one of the most common causes of pediatric bone disease globally. 1 Biochemical abnormalities are detectable at an early stage of rickets across all age groups and have an important role in screening and diagnosis. 2 , – 6 Young infants with rickets often have a more subtle bony phenotype compared with older children given their lack of substantial weight bearing and may remain undiagnosed until later stages of the disease. However, the high metabolic demand for calcium resulting from rapid growth in infancy can lead to acute presentations of rickets with hypocalcemia before the emergence of other clinical or radiologic signs. 7 , – 9 Compared with older children, there may be substantial morbidity associated with infantile rickets given sequelae such as hypocalcemic seizures and, in rare cases, cardiomyopathy. 10 , – 12
Vitamin D deficiency is the predominant cause of nutritional rickets worldwide, particularly in infants. Maternal prenatal vitamin D status is the primary determinant of newborn vitamin D status. 13 , – 17 The major circulating metabolite of vitamin D, 25-hydroxyvitamin D (25(OH)D), crosses the placenta such that cord blood concentrations are highly correlated with maternal values at term. 18 However, the influence of maternal prenatal vitamin D status on infant vitamin D stores diminishes by 2 months of age and infants become dependent on other vitamin D sources. 19 In the Maternal Vitamin D for Infant Growth (MDIG) trial, 20 there was a dose-response effect of prenatal vitamin D supplementation on cord blood and infant vitamin D blood concentrations up to 3 months of age, as has been observed in other prenatal vitamin D supplementation trials. 21 , 22 Therefore, although deficiency in the early postnatal period may be caused primarily by maternal prenatal vitamin D deficiency, 23 vitamin D deficiency later in infancy is attributable to other risk factors. Because breast milk is a poor source of vitamin D if a lactating mother has inadequate vitamin D intake/status, prolonged breast feeding without vitamin D supplementation is an important cause of vitamin D deficiency in infants. However, adequate maternal intake of vitamin D during lactation can support vitamin D sufficiency in the breastfed infant. 24 For example, the MDIG trial demonstrated that continued maternal postpartum supplementation (28 000 IU/week) maintained infant 25(OH)D concentrations at or above 30 nmol/L up to 6 months of age. 20
The role of vitamin D in fetal calcium homeostasis is uncertain; whereas animal studies suggest transplacental transfer may be independent of prenatal maternal vitamin D status, some human studies have provided evidence that maternal prenatal vitamin D status affects fetal calcium accrual. 25 Immediately after delivery, vitamin D is required as an essential regulator of infant intestinal calcium absorption and bone mineral metabolism, similar to older children. 26 Therefore, it is plausible that maternal vitamin D supplementation in the prenatal and postpartum period would reduce the risk of infantile rickets by supporting fetal calcium accrual, neonatal vitamin D endowment, and infant vitamin D intake via breastmilk.
Although there is limited evidence establishing the effect of postpartum vitamin D supplementation in breastfeeding women on the risk of infantile rickets, 27 , 28 there have not been published trials examining prenatal supplementation alone or in combination with postpartum supplementation. Such evidence would be particularly relevant to many low- and middle-income countries such as Bangladesh, where there is a high burden of vitamin D deficiency among both women of child-bearing age and newborns and vitamin D supplementation in infants is not a routine practice. 17 , 29 , – 31 In this substudy of a randomized controlled trial, we aimed to estimate the effect of a range of doses of maternal vitamin D supplementation during pregnancy and continued supplementation during lactation, compared with placebo, on the risk of infantile biochemical rickets at 6 to 12 months of age in Dhaka, Bangladesh.
This study was based on secondary analyses of data from the MDIG trial, conducted in Dhaka, Bangladesh, from 2014 to 2018. This was a randomized double-blinded, placebo-controlled, dose-ranging trial of maternal vitamin D supplementation (from mid-gestation up to 6 months postpartum) for which the primary outcome was infant growth. 20 , 32 Briefly, 1300 generally healthy females 18 years of age or older were enrolled in the second trimester of pregnancy and randomized into 1 of 5 intervention groups: (1) placebo in prenatal and postpartum; (2) prenatal vitamin D3 (4200 IU/week) and placebo postpartum; (3) prenatal vitamin D3 (16 800 IU/week) and placebo postpartum; (4) prenatal vitamin D3 (28 000 IU/week) and placebo postpartum; or (5) vitamin D3 (28 000 IU/week) prenatal and to 6 months postpartum. Supplementation was administered weekly under direct supervision by trained study personnel either in the participant’s home or in the clinic. Participants in all groups were provided daily calcium (500 mg) and iron–folic acid supplements. Ethics approval for secondary use of the trial data for this sub-study was provided by the Research Ethics Board at the Hospital for Sick Children in Canada (REB #1000061259).
Individuals were excluded from the MDIG if there was history of medical conditions with altered vitamin D metabolism and/or hypercalcemia, were having a high-risk pregnancy, were unwilling to stop taking nonstudy vitamin D or calcium supplements or multivitamins containing calcium and/or vitamin D, or were currently being prescribed vitamin D supplements as part of a physician’s treatment plan for vitamin D deficiency. Infants in the MDIG cohort were eligible for biochemical screening at or after 6 months of age; those included in this substudy had at least 1 measurement of serum alkaline phosphatase (ALP) between 6 and 12 months of age ( Supplemental Fig 2 ). Infants with known disorders that affect calcium homeostasis or known skeletal dysplasia would have been excluded from the study, yet no such cases were identified.
Infants in the MDIG were born between June 2014 and February 2016. Systematic screening for rickets at 6-month follow-up visits was launched in May 2016. The biochemical screening panel included serum concentrations of ALP, calcium, and phosphate. Any of the initial parameters found to be outside of established reference ranges prompted a physician referral for assessment and treatment, facilitation of radiographs of wrists and/or knees and an extended laboratory panel (including parathyroid hormone [PTH] and 25(OH)D) that were managed according to the treating physician.
Infant serum calcium, phosphate, and ALP concentrations were measured using quantitative colorimetric assays (Beckman Coulter OSR60117, OSR6122, and OSR6104) at the Clinical Biochemistry Laboratory in Dhaka (icddr,b). Serum 25(OH)D concentrations were measured at the Analytical Facility for Bioactive Molecules (AFBM) in Toronto using high-performance liquid chromatography-tandem mass spectrometry, as previously described. 33 Infant intact PTH concentrations were quantified using a sandwich enzyme-linked immunosorbent assay kit (Immunotopic 60-3100) at AFBM. Clinical management by physicians in Dhaka was informed by local radiologist interpretations of wrist and/or knee radiographs, where available. However, if possible, wrist and/or knee radiographs obtained from children who screened positive for biochemical rickets were further reviewed using a standardized approach by a pediatric radiologist who was blinded to the clinical and laboratory data, as previously described. 20
Biochemical rickets is marked by an elevated ALP level, which is indicative of increased bone turnover; this is a nearly universal feature of rickets and usually the earliest biochemical abnormality. 34 A common compensatory response to hypocalcemia is an elevation in PTH, which promotes the mobilization of calcium from bones. The development of hypocalcemia and hypophosphatemia may occur as the disease progresses or in the presence of an inadequate PTH response. 35 , 36 However, there are no standardized cutoff points for these biochemical markers that define onset or stages of progression of rickets. Age-specific reference ranges must be used for these biochemical markers; ALP in particular is highly dependent on age and rate of bone growth. Here, we defined “biochemical rickets” as (1) ALP ≥ 450 U/L or (2) ALP ≥ 350 U/L plus at least 1 of the following: calcium ≤ 2.2 mmol/L or phosphate ≤ 1.6 mmol/L or PTH ≥ 6.9 pmol/L. The cutoffs for this definition were consensus-based among investigators. This definition used for analytical purposes differed slightly from the definition used to prompt clinical referral during the MDIG study because PTH was not available in real time as part of the initial screening panel.
Left skewing of ALP was noted with a higher-than-expected proportion of low values; of 790 infants in this substudy, 132 (17%) had ALP <90 U/L. These low values were distributed throughout the study period. Following an extensive review, no preanalytical factors were identified that might have artifactually lowered ALP. The distribution of other biochemical markers analyzed in the same samples were similarly distributed in the low ALP and non–low ALP groups (data not shown), ruling out overdilution as an explanation. Hypercalcemia was not observed in the infants with low ALP, making hereditary hypophosphatasia less likely. Malnutrition is known to decrease ALP production, 37 although we did not find differences in anthropometric parameters (weight for age z -score and height for age z -score at 6 months of age) between the low ALP and non–low ALP groups (data not shown). A set of serum samples ( n = 244) from infants in the MDIG across a wider age range than included in this study was tested at the AFBM laboratory at The Hospital for Sick Children using a different colorimetric assay (Alkaline Phosphatase Colorimetric Assay Kit; ab83369); 8.2% (20/244) were found to have ALP <90 IU/L compared with a frequency of 12% among all samples tested at the Clinical Biochemistry Laboratory (135/1085), suggesting that the high proportion of low values in this cohort was a reproducible finding.
Participant characteristics and biomarker concentrations were expressed as mean ± SD, median (25th and 75th percentiles), or frequencies and percentages. PTH was log-transformed because of right-skewing. Participant demographics across the 5 maternal vitamin D treatment arms were compared using analysis of variance for normally distributed continuous variables, Kruskal-Wallis for nonnormally distributed continuous variables, and χ-squared tests for categorical variables. To estimate the relative risk (RR) of infantile rickets in each prenatal and postnatal maternal vitamin D supplementation group, versus placebo, we used a modified Poisson regression with robust error variance. 38 Planned subgroup analyses included unadjusted regression models stratified by child sex, maternal vitamin D status at randomization (25(OH)D ≥30 nmol/L vs <30 nmol/L), and gestational age (term ≥ 37 weeks), respectively. All point estimates were presented with 95% confidence intervals (95% CI) and P values (α < 0.05 considered statistically significant). Data were analyzed using Stata version 16.1 (StataCorp 2019).
Characteristics of participants included in this substudy were similar across the 5 intervention groups ( Table 1 ), as previously reported for the MDIG trial. 20
Demographics and Characteristics of Participants, Stratified by Vitamin D Treatment Group
LAZ, length for age z-score; WAZ, weight for age z-score
Maternal prenatal vitamin D supplementation (second trimester to delivery); postnatal maternal supplementation (0–6 mo).
p value for Kruskal Wallis, Pearson χ 2 , or analysis of variance test.
Based on Intergrowth-21 growth standards, by gestational age, within first 48 h of life, n = 566.
Based on Intergrowth-21st growth standards, by gestational age, within first 48 h of life, n = 550.
Ever consumed a vitamin/supplement containing or possibly containing vitamin D from birth to 1 y.
Number of weeks a supplement containing or possibly containing vitamin D was consumed among infants with at least 1 wk of reported consumption from birth to 6 mo of age, median (interquartile range).
A total of 39 cases of biochemical rickets were identified among 790 infants who underwent biochemical screening. Of these 39 cases, 10 met the criteria based on ALP ≥450 U/L alone, 12 had ALP ≥350 U/L and phosphate ≤1.6 mmol/L as the only abnormalities, 14 had ALP ≥350 U/L and intact PTH ≥6.9 pmol/L as the only abnormalities, and 3 had more than 2 abnormalities.
The highest prevalence of rickets (7.9%) was found in the placebo group ( Table 2 ). The lowest prevalence (1.3%) was in the high-dose supplementation group in which mothers received 28 000 IU prenatally and up to 6 months postpartum; this corresponded to a significantly reduced risk of infantile biochemical rickets compared with placebo ( Table 2 ). High-dose vitamin D during the prenatal period alone (4200 IU/week, 16 800 IU/week, and 28 000 IU/week) did not have a significant effect on the risk of rickets, although there were fewer rickets cases identified in each of these groups compared with placebo ( Table 2 ).
RR of Rickets in Each Treatment Arm Compared With Placebo
RR, relative risk.
Poisson regression model with robust error variance used to obtain RR.
In an analysis restricted to infants born to women with baseline 25(OH)D <30 nmol/L during the second trimester of pregnancy ( n = 507), inferences were unchanged ( Fig 1 ). Inferences also remained the same in stratified analysis by sex (males or females), albeit more male than female infants were affected by rickets overall. Inferences remained the same when analysis was restricted to infants born at term ( ≥ 37 weeks’ gestation) ( Supplemental Tables 3 – 5 ).

The relative risk of biochemical rickets among varying doses of maternal prenatal and postpartum vitamin D supplementation compared with placebo using modified Poisson regression (blue bars). Subgroup analysis assessing the effect of maternal vitamin D supplementation on infantile rickets among women with vitamin D deficiency (25(OH)D <30 nmol) at baseline ( n = 507). The circles represent the effect estimates, with 95% confidence interval (CI) bars.
Serum calcium concentrations were highest in the combined supplementation group and lowest in the placebo group; however, these differences were not statistically significant ( Supplemental Fig 4 ). Phosphate concentrations were significantly higher and ALP concentrations were significantly lower in the combined supplementation group compared with placebo ( Supplemental Fig 4 ).
Of the 39 infants with biochemical rickets, 16 had radiographs of the wrist and/or knee available for review by the SickKids radiologist, of whom 4 were found to have radiographic findings of rickets, as previously reported. 20 Three of the 4 infants were in the placebo group, and the fourth was in the group administered 4200 IU/week prenatally. Mean ALP was higher at presentation for these infants, at 705 U/L, compared with mean 439 U/L for the other infants with biochemical rickets. All 4 infants were hypophosphatemic (serum phosphate <1.56 mmol/), and 1 was hypocalcemic (serum calcium <2.1 mmol/L). Radiographs were not available for all infants with biochemical rickets. In large part, this was because infants who met criteria of ALP ≥ 350 U/L and PTH ≥ 6.9 pmol/L were not flagged for imaging because PTH was not available in real time as part of the initial screening panels.
Combined prenatal and postpartum maternal supplementation (28 000; 28 000 IU/week) decreased the risk of biochemical rickets compared with placebo among infants 6 to 12 months of age. However, maternal prenatal supplementation alone at any dose, without postpartum continuation, did not significantly decrease the risk of biochemical rickets. Prenatal maternal vitamin D supplementation influences early postnatal infant 25(OH)D, but postpartum continuation was required to maintain 25(OH)D ≥30 nmol/L up to 6 months of age, as previously reported in the MDIG trial ( Supplemental Fig 3 ). 20 Therefore, the present findings strongly support the hypothesis that vitamin D deficiency (marked by inadequate circulating 25(OH)D), is an important cause of biochemical rickets in this infant population. As previously reported, all the cases of radiographically confirmed rickets were in the placebo and lowest-dose prenatal supplementation (4200 IU weekly prenatally) groups, further supporting the potential role of vitamin D in rickets prevention. However, we cannot rule out other causes of rickets in this setting; moreover, most infants with 25(OH)D <30 nmol/L did not have biochemical rickets, indicating that other contributing factors act in concert with vitamin D deficiency.
There were relatively more male infants affected by biochemical rickets in our study. It has been speculated that rickets may occur more frequently in boys because of greater linear bone growth and increased skeletal demands during times of rapid growth. Although not seen consistently, this phenomenon has been noted in several studies evaluating rickets in infancy. 39 , – 41 The present findings are consistent with evidence from 2 smaller randomized trials in India that previously found that there were fewer cases of biochemical rickets among infants of mothers who received postpartum supplementation. 27 , 28 Although it has been well established that infant 25(OH)D status can be influenced by maternal supplementation during lactation, the dose-response relationship remains uncertain. 24 , 42 Human milk is considered a poor source of vitamin D3 unless the lactating woman has high amount of vitamin D intake. 43 The transfer of the vitamin D parent compound (vitamin D3) is favored over 25(OH)D in the mammary gland, suggesting that the vitamin D concentration of breast milk is primarily affected by maternal vitamin D intake or cutaneous synthesis rather than maternal vitamin D status (ie, circulating 25(OH)D). 44 , 45 This distinction is important because the short half-life of vitamin D3 (12–24 hours) implies that an analogous dose of vitamin D is consumed by the infant soon after the corresponding maternal ingestion. 46 However, low daily doses of maternal vitamin D supplementation may not achieve sufficiently high circulating levels of vitamin D in breast milk to impact infant 25(OH)D, even if they prevent maternal vitamin D deficiency. 47 High-dose maternal supplementation, often greater than the Institute of Medicine–recommended upper limit of 4000 IU/day, 48 has been previously shown to have similar effects on breastfeeding infant 25(OH)D as daily infant vitamin D supplementation. 42 , 49 , 50 Further research involving direct comparison of various doses, including daily maternal dosing compared with intermittent weekly or bolus dosing regimens, is required to determine the minimum effective maternal postpartum dose to maintain 25(OH)D sufficiency in infants and in turn minimize the risk of rickets.
A strength of this study is that the randomized, dose-ranging, placebo-controlled design of the MDIG trial and the lack of routine infant supplementation permitted causal inferences regarding the effects of maternal vitamin D supplementation on the risk of biochemical rickets. However, several limitations of the study should be acknowledged. This is a substudy of a previous trial; the mother and infant pairs included were selected from the existing MDIG cohort based on data availability, which may have compromised the generalizability of the findings. Although the participants in this substudy were similar to the remainder of the MDIG cohort, it is possible that this cohort was not fully representative of the mothers and infants in the MDIG trial or of the general population in Dhaka. The biochemical case definition was useful for identifying early disease because infants with rickets may present without skeletal abnormalities; however, we lacked complete radiographic information for all the infants who met biochemical rickets criteria, and the longer term clinical significance of infantile biochemical rickets is uncertain. Because the diagnosis of biochemical rickets was based on cross-sectional biochemical evaluation starting at 6 months of age, we were unable to determine the precise age of onset of the abnormalities. Furthermore, a greater number of infants screened late in infancy or at older ages might have enabled us to describe the natural history of this process in the absence of routine supplementation or vitamin D treatment of those who screened positive in early infancy.
High-dose maternal postpartum vitamin D supplementation may serve as a viable public health strategy for rickets prevention by effectively increasing infant 25(OH)D status in conjunction with efforts to promote breastfeeding. Other low- and middle-income countries in South Asia that have similar burdens of maternal and infant vitamin D deficiency and do not have vitamin D supplementation programs could benefit from this strategy. Future studies should include comparisons of different doses of maternal postpartum supplementation and longer term follow-up including radiologic assessments and clinical outcomes.
We thank Huma Qamar of The Global Centre for Child Health, The Hospital for Sick Children, for her assistance with data organization and Talia Wolfe, former summer student at The Global Centre for Child Health, The Hospital for Sick Children, for her work on the initial data analysis.
Dr Roth is the principal investigator, conceptualized, designed, and supervised the study, drafted the initial manuscript, and critically reviewed and revised the manuscript; Dr Lautatzis designed the study, performed statistical analysis, drafted the initial manuscript, and critically reviewed and revised the manuscript; Dr Al Mahmud supervised data collection and field study activities in Dhaka and critically reviewed and revised the manuscript; Drs Ahmed and Keya contributed to local implementation of the study and data collection in Dhaka, and critically reviewed and revised the manuscript; Ms Tariq contributed to study design, performed statistical analysis, drafted the initial manuscript, and critically reviewed and revised the manuscript; Dr Harrington, Dr Zlotkin, Dr Lam, and Dr Morris contributed to study design, and critically reviewed and revised the manuscript; Dr Stimec provided expert review of radiographic data and critically reviewed and revised the manuscript; and all authors read and approved the final manuscript and agree to be accountable for all aspects of the work. The authors report no conflicts of interest or financial relationships relevant to this article to disclose.
Clinical Trial Registration: This trial has been registered at www.clinicaltrials.gov (identifier NCT01924013).
25-hydroxyvitamin D
95% confidence interval
Analytical Facility for Bioactive Molecules
alkaline phosphatase
Maternal Vitamin D for Infant Growth
parathyroid hormone
relative risk
Competing Interests

Supplementary data
Advertising Disclaimer »
Citing articles via
Email alerts.

Affiliations
- Editorial Board
- Editorial Policies
- Journal Blogs
- Pediatrics On Call
- Online ISSN 1098-4275
- Print ISSN 0031-4005
- Pediatrics Open Science
- Hospital Pediatrics
- Pediatrics in Review
- AAP Grand Rounds
- Latest News
- Pediatric Care Online
- Red Book Online
- Pediatric Patient Education
- AAP Toolkits
- AAP Pediatric Coding Newsletter
First 1,000 Days Knowledge Center
Institutions/librarians, group practices, licensing/permissions, integrations, advertising.
- Privacy Statement | Accessibility Statement | Terms of Use | Support Center | Contact Us
- © Copyright American Academy of Pediatrics
This Feature Is Available To Subscribers Only
Sign In or Create an Account

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
Vitamin E Intake and Risk of Prostate Cancer: A Meta-Analysis
1 Saw Swee Hock School of Public Health, National University of Singapore and National University Health System, 12 Science Drive 2, #10-01, Singapore 117549, Singapore
Jiyoung Youn
2 Department of Food and Nutrition, College of Human Ecology, Seoul National University, Seoul 08826, Republic of Korea
Wei Jie Seow
Associated data.
Data described in the manuscript, code book, and analytic code will be made available upon request from the corresponding author, pending application and approval.
Vitamin E is a group of antioxidative tocopherols and tocotrienols that play a potential role in chemoprevention. Studies investigating the association between vitamin E and prostate cancer risk have been conflicting. We identified observational and interventional studies examining the association between vitamin E intake and prostate cancer risk from PubMed, EMBASE and the Cochrane Library. A random-effects model was used to perform a meta-analysis and estimate relative risks (RRs) and the corresponding 95% confidence intervals (CIs) of prostate cancer risk according to vitamin E intake. Subgroup analyses were conducted by study design, sample size, study population characteristics, geographical region, and dose of vitamin E intake. The association between dietary (RR = 0.97; 95% CI = 0.92–1.02) and supplemental (RR = 0.99; 95% CI = 0.94–1.04) vitamin E intake on prostate cancer risk was non-significant. In subgroup analyses, supplemental vitamin E was significantly associated with reduced prostate cancer risk in studies in Europe (RR = 0.81, 95% CI = 0.69–0.97). Overall, this meta-analysis demonstrates little evidence for a beneficial effect of vitamin E intake on prostate cancer risk but suggests that there may be some conditions in which supplements could confer a protective effect on prostate cancer risk.
1. Introduction
Prostate cancer is characterised by uncontrolled cell growth within the prostate, which is a small muscular gland located below the bladder in men. In more than half of the countries in the world, prostate cancer is the most frequently diagnosed cancer among men [ 1 ]. Globally, there were an estimated 1,414,259 newly diagnosed cases in 2020 [ 1 ]. However, the etiology of prostate cancer has remained poorly understood compared to other common cancers [ 2 , 3 ].
Vitamin E is a group of antioxidant fat-soluble micronutrients (α-, γ-, δ-, β-tocotrienol and α-, γ-, δ-, β-tocopherol) that is found in high amounts (>10 mg per 100 mL or 100 mg) in nuts, seeds and vegetable oil [ 4 ]. It has been reported that consuming 1.5 ounces of almonds or hazelnuts may provide up to approximately 75% of the recommended intake of 15 mg/day. Vitamin E has been identified as a potential chemopreventive agent due to its radical-scavenging antioxidative effects [ 5 , 6 ]. Both tocopherols and tocotrienols have demonstrated effectiveness in the growth inhibition of prostate cancer cells in in vitro studies [ 7 , 8 ]. Many studies, including large-scale randomized controlled trials (RCTs), have attempted to investigate the potential chemopreventive effects of supplemental vitamin E in prostate cancer, but findings have been inconsistent [ 9 , 10 , 11 , 12 , 13 , 14 ].
Previously, a meta-analysis of RCTs using vitamin E-containing interventions estimated a significant protective effect for vitamin E on prostate cancer risk [ 15 ]. However, this meta-analysis only included five studies and its findings were largely driven by a single study, the Alpha-Tocopherol Beta-Carotene (ATBC) trial. In another meta-analysis of both observational and interventional studies, no associations were found between the use of vitamin E supplements and prostate cancer risk [ 16 ]. Meanwhile, no meta-analysis has been conducted to date on the association between dietary vitamin E and prostate cancer risk. The effectiveness of dietary and supplemental vitamin E intake may differ, given the differences in stereoisomerism between natural and synthetic forms [ 17 ]. Additionally, vitamin E is a frequently consumed supplement, particularly in Western populations [ 18 , 19 ]. Therefore, our study aimed to provide updated evidence on the respective associations between dietary, supplemental, or total vitamin E intake with prostate cancer risk.
2. Materials and Methods
The protocol was developed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-P) statement [ 20 ].
2.1. Search Strategy
A search of the electronic databases PUBMED, EMBASE, and the Cochrane Library for references published before 30 November 2021 was undertaken. We used a combination of standard controlled vocabulary (MeSH and Emtree) and keywords for (1) vitamin E and (2) prostate cancer to identify relevant references that studied the association between vitamin E and prostate cancer risk. The search strings used for all three databases are presented in Supplementary Table S1 . For each database, all references identified with the final search terms were downloaded into Endnote X9 software (Version 3.3, Clarivate Analytics, London, UK). We also searched through the reference lists of studies that fulfilled the eligibility criteria in screening to identify additional references.
2.2. Eligibility Criteria
We included RCTs and observational studies (case-control studies, cohort studies, case-cohort studies, nested case-control studies) that studied the association between vitamin intake (including any of its eight isoforms: α-, β-, γ-, and δ-tocopherol as well as α-, β-, γ-, and δ-tocotrienol) and prostate cancer risk in our meta-analysis. RCTs evaluating the use of a multi-vitamin supplement were eligible if vitamin E was described as a component. Studies had to have enrolled adult male participants over 40 years of age and presented risk estimates of prostate cancer (risk ratio, hazard ratio, odds ratio) as well as the respective 95% CI according to categories of dietary and/or supplemental vitamin E intake.
If multiple studies used data from the same population, the study with the longest follow-up time was included in this meta-analysis. Included studies had to be written in English and published in peer-reviewed journals.
2.3. Study Selection and Data Extraction
Two reviewers, LWQ and YJY, independently screened all references downloaded from the three databases. The following data items were extracted from the included studies: publication information (article title, author details, journal, year of study, location of study), study population (sample size, study design, demographics such as age and ethnicity), exposure or intervention of vitamin E intake (type of vitamin E intake [i.e., dietary, supplemental or total]), prostate cancer risk estimates of highest versus lowest category of vitamin E intake (risk ratios, rate ratios, odds ratios or hazards ratios, and their respective 95% CI), as well as any covariates that were adjusted for in the models. When results from multiple statistical models were presented, risk estimates and the respective 95% CI were extracted from the model that adjusted for more covariates. Data extraction was completed through an electronic form developed in Microsoft Excel. Any inconsistencies between the two reviewers were resolved through discussion and consensus.
2.4. Quality Assessment
Two reviewers, LWQ and YJY, evaluated the risk of bias of individual studies independently. RCTs were assessed using the Revised Cochrane Risk-of-Bias (RoB 2) tool, which consists of five domains: (1) bias arising from the randomization process, (2) bias due to deviations from intended interventions, (3) bias due to missing outcome data, (4) bias in the measurement of the outcomes, and (5) bias in the selection of the reported result [ 21 ]. The risk levels were classified as ‘low risk of bias’, ‘some concerns’ and ‘high risk of bias’ according to the signalling questions provided.
Observational studies were assessed using the Cochrane tool Risk of Bias In Non-randomised Studies of Interventions (ROBINS-I) [ 22 ]. This tool evaluated the internal validity of individual studies across seven domains, comprising: (1) bias due to confounding, (2) selection bias, (3) bias in classification of interventions, (4) bias due to departure from intended interventions, (5) bias due to missing data, (6) bias in measurement of outcomes, and (7) bias in selection of reporting of results. Each domain was categorized to be at “low risk”, “moderate risk”, “serious risk” or “critical risk” of bias according to the signalling questions provided. Any disagreements were resolved through discussion among the two reviewers.
2.5. Statistical Analysis
Using data extracted from the included studies, pooled risk estimates and respective 95% CIs for prostate cancer risk according to vitamin E intake (highest category versus lowest category) were computed. We chose to implement the random effects model in this meta-analysis as the studies were clinically heterogeneous (e.g., different study designs, doses of vitamin E intake), and were likely to estimate different underlying true effects. The restricted maximum likelihood method was used to estimate the heterogeneity variance. We examined and quantified the statistical heterogeneity of the study results using a Cochrane Q test and I 2 values. Synthesis of the overall estimate was done with careful consideration of the heterogeneity, making sure that studies were only combined under appropriate heterogeneity levels (<70%). Subgroup analyses according to study design, sample size, study population characteristics, geographical region and dose of vitamin E intake were conducted to determine if pooled risk estimates differed across these characteristics. To assess the robustness of our findings, we performed sensitivity analyses by excluding one study at a time to examine the magnitude of influence each study had on the pooled risk estimates. We also carried out further sensitivity analyses by excluding studies with a high or serious risk of bias, as determined by the RoB2 and ROBINS-I tools, as well as limiting studies to those that had adjusted for important confounders (i.e., energy intake and family history of prostate cancer). We also attempted to estimate the trend of relative risk estimates across increasing categories of vitamin E intake through a dose-response meta-analysis using the ‘dosres’ package in R [ 23 , 24 , 25 ].
We examined small study effects, including potential publication bias, by carrying out a funnel plot analysis and assessing asymmetry using an Egger’s regression test. The trim-and-fill method was applied to calculate an adjusted effect size. All analyses were done using the ‘metafor’ package in R (R Version 4.0, R Core Team, Vienna, Austria) [ 26 ]. All p values were two-sided, with a value of <0.05 being considered as statistically significant.
3.1. Characteristics of Studies Selected
Details of the study selection process are presented in a PRISMA flowchart ( Figure 1 ). A total of 12,753 potentially relevant articles were identified from the databases of PubMed, EMBASE and the Cochrane Library. A total of 32 studies were included in the meta-analysis after screening.

PRISMA flowchart outlining the study selection and data extraction process.
Table 1 presents the characteristics of 32 studies included in this meta-analysis evaluating the association between vitamin E intake and overall prostate cancer risk. The age of the participants ranged from 35 to 89 years. The majority of the studies were conducted in the United States (12 studies), Europe (11 studies) and Canada (five studies). The remaining studies took place across several countries (two studies), or were conducted in Australia (one study) and Uruguay (one study).
Characteristics of the studies included in the meta-analysis.
ATBC: Alpha-tocopherol, Beta-Carotene Cancer Prevention Study; BMI: Body mass index; CAPLIFE: Prostate cancer lifestyles study; CPS-II: Cancer Prevention Study II; CSDLH: Canadian Study of Diet, Lifestyle, and Health; FFQ: Food frequency questionnaire; FinsRPC: Finnish Prostate Cancer Screening Trial; HPFS: Health Professionals Follow-up Study; HOPE: Heart Outcomes Prevention Evaluation; HOPE-TOO: Heart Outcomes Prevention Evaluation–The Ongoing Outcomes; MEC: Multiethnic Cohort; NIH-AARP: National Institutes of Health-American Association of Retired Persons; NLCS: Netherlands Cohort Study; PHS II: Physicians’ Health Study II; PLCO: Prostate, Lung, Colorectal, and Ovarian Cancer; PSA: Prostate-specific antigen; RCT: Randomised controlled trial; SELECT: Selenium and Vitamin E Cancer Prevention Trial; SU.VI.MAX: Supplementation en Vitamines et Mineraux Antioxydants;VITAL: VITamin D and OmegA-3 TriaL; WNYDS: Western New York Diet Study.
We identified 19 studies that investigated associations between dietary intake of vitamin E and prostate cancer risk. This included 11 case-control studies, six prospective cohort studies, one case-cohort study and one nested case-control study. In total, the analysis comprised 516,753 participants, in which 27,141 cases of prostate cancer were identified.
Meanwhile, we identified a total of 18 studies that evaluated the supplemental intake of vitamin E and prostate cancer risk, comprising six RCTs, nine prospective cohort studies, two case-control studies and one case-cohort study. Here, the analysis consisted of 686,348 non-overlapping participants, among which 31,274 cases of prostate cancer had been identified.
There were five studies evaluating the association between total (both diet and supplemental) intake of vitamin E and prostate cancer risk. This comprised one case-control study, three prospective cohort studies and one case-cohort study. In total, the analysis included 94,421 non-overlapping participants, in which 5122 cases of prostate cancer had been identified.
3.2. Overall Analysis of Vitamin E Intake and Prostate Cancer
The pooled relative risk estimates of prostate cancer risk were 0.97 (95% CI = 0.92–1.02, I 2 = 7.47%; Figure 2 A) for dietary vitamin E intake and 0.99 (95% CI = 0.94–1.04, I2 = 34.64%; Figure 2 B) for supplemental vitamin E intake. There was no evidence of an association between total (dietary and supplemental) vitamin E intake and prostate cancer risk (RR = 0.96, 95% CI = 0.85–1.08, I 2 = 0.00%; Figure 2 C). Overall, the statistical heterogeneity for the three pooled relative risk estimates were either low (I 2 < 25%) or moderate (25% ≤ I 2 < 50%).

Forest plot for associations between ( A ) dietary, ( B ) supplemental and ( C ) total vitamin E intake and prostate cancer risk. CI: Confidence interval; RR: Relative risk.
3.3. Small-Study Effects and Quality Analysis
To assess the presence of small-study effects, we carried out funnel-plot analyses of the included studies on dietary ( Figure 3 A) and supplemental vitamin E intake ( Figure 3 B). Using Egger’s regression test for funnel plot asymmetry, we found borderline significant evidence for small study effects, including publication bias, for the studies on dietary intake ( p value = 0.060) and supplemental intake ( p value = 0.048) and prostate cancer risk. Applying the trim-and-fill method did not drastically alter the risk estimates (RR = 0.98, 95% CI = 0.93–1.03 for dietary intake; RR = 1.01, 95% CI = 0.95–1.08 for supplemental intake). We did not carry out an assessment of small-study effects for studies on total vitamin E intake as the number of studies with this variable were limited.

Funnel-plot analyses of studies included in meta-analysis for ( A ) dietary vitamin E intake and ( B ) supplemental vitamin E intake.
The overall risk of bias for RCTs and observational studies are presented in Figure 4 A,B. Out of the six RCTs, three were rated as ‘low risk’ of bias, while the remaining three were assessed to have ‘some concerns’ of bias. All observational studies included in our analysis were assessed to be at either ‘moderate’ risk of bias (13 out of 26 studies), or at ‘serious’ risk of bias (13 out of 26 studies). Potential confounding and/or selection bias were the most concerning issues that led to ‘serious’ risk of bias.

Summary bar plots assessing the risk of bias in ( A ) randomized controlled trials and ( B ) observational studies using the RoB2 and ROBINS-I tools, respectively.
3.4. Sensitivity Analyses
During the leave-one-out sensitivity analysis, pooled relative risk estimates remained largely similar to original estimates for dietary/supplemental intake of vitamin E and prostate cancer risk. However, when excluding the prospective cohort study by Stram et al., the inverse association between dietary vitamin E intake and prostate cancer risk attained borderline significance (RR = 0.95; 95% CI = 0.90–1.00; I 2 = 0.04%). Further sensitivity analyses by excluding observational studies at ‘serious’ risk of bias or RCTs with ‘some concerns’ of bias did not alter our findings for dietary vitamin E (RR: 0.97; 95% CI = 0.91–1.04; I 2 = 18.98%) or supplemental vitamin E (RR = 0.99; 95% CI = 0.95–1.03; I 2 = 0.00%). In addition, restricting studies to those that had adjusted for energy intake (dietary vitamin E: RR = 0.98; 95% CI = 0.92–1.04; I 2 = 10.13%; supplemental vitamin E: RR = 0.95; 95% CI = 0.83–1.09; I 2 = 0.00%) or family history of prostate cancer (dietary vitamin E: RR = 0.95, 95% CI = 0.88–1.03; I 2 = 27.77%); supplemental vitamin E: RR = 1.00; 95% CI = 0.95–1.04; I 2 = 0.00%) did not alter our findings. There was limited evidence of a dose-response relationship for dietary or supplemental vitamin E intake and prostate cancer risk. Sensitivity analysis for studies on total vitamin E intake were not conducted, as the number of studies on this variable were limited.
3.5. Subgroup Analyses
Results of the subgroup analyses are summarised in Table 2 . For dietary vitamin E, there remained no significant associations between intake and prostate cancer risk in the subgroup analyses according to study design, sample size, geographical region, and amount of vitamin E intake. There was a significant subgroup difference for studies conducted in Europe as compared to North America ( p value for subgroup differences = 0.036).
Subgroup analyses of studies on vitamin E intake and prostate cancer.
Abbreviations: IU, International units; RCT: Randomized controlled trial. a Recommended daily intake by the Institute of Medicine Panel on Dietary Antioxidants and Related Compounds in the United States. The guidelines for intake may differ from country to country and can vary from 3 mg/day to 15 mg/day [ 53 ]. Bolded values represent a statistically significant result at p value < 0.05.
For supplemental vitamin E intake, the pooled risk estimates in studies of European populations (RR = 0.81; 95% CI = 0.69–0.97; I 2 = 33.56%) and North American populations (RR = 1.01; 95% CI = 0.97–1.06; I 2 = 18.76%) were significantly different ( p value for subgroup differences = 0.020). However, study design, study type, sample size, dose of supplements used, as well as the presence of underlying conditions in participants of RCTs, did not appear to influence estimates of prostate cancer risk with supplemental vitamin E intake.
4. Discussion
In this meta-analysis, we quantitatively estimated the associations between dietary and supplemental vitamin E and prostate cancer risk by pooling estimates in observational and interventional studies published to date.
Although the risk estimates (RR = 0.97; 95% CI = 0.92–1.02; I 2 = 7.47%) were suggestive of a slight reduction in prostate cancer risk for high dietary intake of vitamin E, there was no statistical evidence for a benefit. This implies that a high dietary intake of vitamin E may not account for the inverse associations between serum/plasma vitamin E (in particular, α-tocopherol) and prostate cancer risk that have been reported in the literature [ 54 , 55 ]. Apart from dietary intake, serum/plasma concentrations of α-tocopherol can be influenced by other factors including genetics, use of supplements, seasonality, ethnicity, and location of residence [ 56 , 57 , 58 , 59 , 60 ]. In a nested case-control study of the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial, minor alleles on an single nucleotide polymorphism rs964184 located near the apolipoprotein 5 gene, known to be involved in vitamin E transport and metabolism, were significantly inversely associated with prostate cancer risk [ 61 ].
Supplemental intake of vitamin E was not associated with prostate cancer risk in this study. This null association is consistent with findings from previous reviews [ 15 , 16 , 62 ]. However, we found statistically significant subgroup differences between studies conducted in Europe and North America regarding the effect of vitamin E. Further, a significant inverse association was observed between supplemental vitamin E and prostate cancer risk when combining studies in Europe. One possible explanation for this observation is the difference in predominant forms of dietary vitamin E in these regions. Vitamin E forms can be found in varying proportions in vegetable oils: α-tocopherol is found in higher amounts in sunflower and olive oil while γ-tocopherol is more common in corn and soybean oil [ 63 , 64 ]. Although α-tocopherol is the predominant dietary form in Europe as well as commercial vitamin E supplements, γ-tocopherol is the predominant form of dietary vitamin E in countries in the North America region, including the United States [ 65 , 66 ]. Importantly, γ-tocopherol acts as a weak competitive substrate to α-tocopherol for binding to hepatic α-tocopherol transfer protein, and the intake of α -tocopherol has been inversely associated with circulating γ -tocopherol levels [ 59 , 67 , 68 , 69 , 70 , 71 ]. The beneficial effect of supplements (typically α-tocopherol) in North America could have been counterbalanced by the relatively high dietary intake of γ-tocopherol and low dietary intake of α-tocopherol as compared to European counterparts. Future research pertaining to the effects of dietary γ-tocopherol, alongside α-tocopherol metabolism, and prostate cancer risk may be useful in better understanding the association observed.
Additionally, differences in fortification and enrichment practices in North America and Europe may have influenced nutritional adequacy in the populations and result in differential benefits of supplementation [ 72 ]. However, we acknowledge that due to the relatively few studies from Europe (four studies), it is possible that the significant inverse association between vitamin E supplements and prostate cancer risk is a spurious finding by chance.
When evaluating total vitamin E intake with prostate cancer risk, we found that there were no significant associations. However, we were also limited by the number of eligible studies (five studies) in evaluating this exposure variable.
One strength of our meta-analysis is that a low level of heterogeneity was observed within the overall analysis. Results obtained by combining studies of different designs may lead to bias resulting from heterogeneity. the I 2 values for the overall analysis were not substantial (<40%), indicating that the studies included could be reasonably combined. Furthermore, our subgroup analysis by study design suggested that there were no differences in effect detected between studies of various designs.
Secondly, our study took into account both the dietary and supplemental intake of vitamin E, as the effect of these intakes are likely to be interrelated. Past meta-analyses have focused on the use of vitamin E supplements alone and prostate cancer risk, or combined a mixture of studies on either dietary and supplemental intake, without considering that the exposure variables were distinct but also additive [ 15 , 16 , 62 ].
However, there were also several limitations with our meta-analysis. Firstly, the studies used various assessment methods to measure intake, as well as different cut-off values to categorize intake. These variations introduce heterogeneity and make the pooled risk estimates difficult to interpret. Although a dose-response meta-analysis could have addressed this by enabling one to extract multiple risk estimates across varying doses from the same study, we were limited by the number of studies providing sufficient information (i.e., dose levels) for such analysis. We also acknowledge that the lack of association observed in the meta-analysis could be due to a lack of statistical power or a lack of precision due to the inherent information biases of measuring dietary intake through methods such as food-frequency questionnaires and food diaries. Here, non-differential misclassification may bias the results towards the null.
Secondly, we were unable to factor in the bioavailability of vitamin E in our meta-analysis. The absorption rate of vitamin E, which can range from 20% to 80%, is heavily influenced by other factors such as the food matrix present [ 17 ]. We were limited in data in this respect, as most of the included studies do not take bioavailability into account in the estimation of vitamin E intake as a variable.
Furthermore, most studies in the meta-analysis do not differentiate between the subtypes of vitamin E. This may be limited by the challenges faced in separation and quantification of tocopherols and tocotrienols in various food types [ 17 ]. As a result, we were unable to evaluate or compare the effect of different vitamin E isoforms on prostate cancer risk. To date, studies have mostly focused on α-tocopherol, and some have quantified other vitamin E isoforms based on α-tocopherol equivalents. This may be driven by the fact that α-tocopherol was thought to possess the highest biological activities compared to other isoforms of vitamin E. [ 66 ] Future studies should look to investigating the effects of different vitamin E forms on prostate cancer risk, as there is a difference in prevalent forms between geographical regions, and promising experimental and clinical data have emerged on the bioactivities of tocotrienols [ 73 , 74 , 75 , 76 ]. Only one study in our meta-analysis had analysed the intake of tocotrienols as distinct variables [ 36 ].
Additionally, the studies included in our meta-analysis tended to overlook fortified sources and cooking oils, which could be major sources of vitamin E when computing intake. This could have led to an underestimate of vitamin E intake and/or non-differential misclassification, which may have biased the results towards the null.
Lastly, as the majority of the studies had been conducted in Western populations in Europe or North America, the findings may face limited generalisability to populations from other regions, such as Africa or Asia.
Overall, our meta-analysis implies that neither vitamin E supplements, nor a high dietary intake of vitamin E, are likely to be significantly useful in a chemopreventive capacity for prostate cancer. However, future studies may benefit from investigating the intake of specific vitamin E forms and prostate cancer risk in various geographical regions.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nu15010014/s1 , Table S1: Search terms used to identify relevant references.
Funding Statement
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI21C0915).
Author Contributions
The authors’ responsibilities were as follows—W.Q.L.: performed the statistical analyses and drafted the initial manuscript; J.Y.: performed screening and data extraction of studies as an additional independent reviewer; W.J.S.: supervised statistical analysis and interpretation of results, critically revised manuscript, and took primary responsibility for the final content; All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Ethical review and approval were waived for this study as this is a meta-analysis of previously published studies.
Informed Consent Statement
Not applicable as this is a meta-analysis of previously published studies.
Data Availability Statement
Conflicts of interest.
The authors declare that they have no conflict of interest.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
- Healthy living
- Speaker Series
- Find Faculty
Welcome to the Friedman School
- About the Friedman School
- Friedman School Leadership Team
Divisions and Centers
- Named Professorships and Directorships
- Board of Advisors
- Strategic Plan
- New! Annual Report
- Contacting Us
- Visiting Us
- About The Friedmans
The Latest @ Friedman
- Follow Us on Twitter
- Like Us on Facebook
- Watch Us on Vimeo
- Join the Network on LinkedIn
More School Information
- School Administration
- Diversity, Equity, & Inclusion
- Jobs and Careers at the Friedman School
- Policies and Procedures
- Office of Equal Opportunity
- Tufts Threat Assessment and Management
- Family Educational Rights and Privacy Act
Tufts University Friedman School of Nutrition Science and Policy 150 Harrison Avenue Boston, MA 02111

Course Catalog
- Browse the Friedman Course Catalog
- Academic Calendar
- View the Academic Calendar
- Graduate Degree Programs
- MS, PhD Agriculture, Food and Environment
- MS, PhD Biochemical and Molecular Nutrition
- MS, PhD Food and Nutrition Policy and Programs
- MS, PhD Nutrition Epidemiology and Data Science
- MS, PhD Nutrition Interventions, Communication, and Behavior Change
- MAHA Master of Arts in Humanitarian Assistance
- MNSP Master of Nutrition Science and Policy
- MS/DI Master of Science/Dietetic Internship
- MS Master of Science in Sustainable Water Management
Online and Continuing Education
- Online Graduate Courses and Certificate Programs
- Take a Single Course Online or On-Campus
- NEW 6-week Mini-Course, “Serving a Healthy Diet”
- NEW Free Nutrition Micro-Courses
Special Initiatives
- Entrepreneurial Education Initiative
- Service Scholars Program
- Biggest Impact
- Nutrition Summer Session
- Combined Graduate Degree Programs
- MALD Master of Arts International Nutrition + Law and Diplomacy
- MS/DPD Master of Science in Nutrition + Didactic Program in Dietetics
- MS/MA Urban & Environmental Policy & Planning + Nutrition Science and Policy
- MS/MPH Master of Science in Nutrition + Master of Public Health

Applying to Friedman
- Schedule a Visit
- Dates & Deadlines
- New Student Orientation
- Info for International Students
- Graduate Student Fairs & Events
- Online Information Sessions
- Tuition & Financial Aid
- Current Tuition & Fees
- Scholarships
Our Programs
- Internship Information
Student Life
- Student Council
- Friedman Student Organizations
- Student Events
- Living in Boston

Friedman Research
- Research Activities
- Research Themes
- Nourished Children, Families, and Communities
- Healthy Food for All
- Longevity and Vitality
- Sustainable Food Environments
- Discovery and Entrepreneurship
- Creating and Enabling Leaders
- Public Impact Initiative
- Foundational Initiatives
Research Partners & Resources
- Jean Mayer USDA Human Nutrition Research Center on Aging-HNRCA
- Research Information at Tufts
- Hirsh Health Sciences Library
- Tufts Clinical and Translational Science Institute
- Research Communication and Promotion
- Hiring a Student Research Assistant/Hourly Student
Research Centers & Initiatives
- ChildObesity 180
- Feed the Future: Nutrition Innovation Lab
- Feinstein International Center
- New Entry Sustainable Farming Project
- Browse More Research Activities

Friedman Faculty
- Faculty Directory
- Office of Faculty Affairs
- Getting Started at Friedman
- Faculty Openings at the Friedman School
- Postdoctoral Scholars
- Division of Agriculture, Food and Environment
- Division of Biochemical and Molecular Nutrition
- Division of Food and Nutrition Policy and Programs
- Division of Nutrition Epidemiology and Data Science
- Division of Nutrition Interventions, Communication, and Behavior Change
- Feinstein International Center (FIC)
- Food and Nutrition Innovation Institute (FNII)
Teaching Resources
- Center for the Enhancement of Learning & Teaching
- TA Request Form
School and Campus Resources
- Tufts Human Resources
- Health & Wellness
- Technology Resources
- Documents and Forms

Office of Student Affairs
- Friedman Registrar Office
- Registration
- Cross-Registration, Graduation, Degree Requirements, and Transcripts
- Policies and Procedures Handbook
- Privacy Statement and Terms of Use
- Explore Chinatown in Boston
Ellie Block and Family Career Services Center
The Ellie Block and Family Career Services Center at the Friedman School is committed to helping our students and graduates leverage their outstanding experiential education to find impactful and fulfilling careers. Our career coaches leverage their many years of experience, career development training and practice, and industry and employer insights, to assist students and alumni. Learn More
School & Campus Resources
- Student Resources
- Bursar's Office
- Student Payment Request
- Information for International Students
- Information for PhD Students
- Program Discretionary Funds Request Form
- Student Advisory and Health Administration (SAHA)

Making an Impact
- Food is Medicine
- Public Impact & Our Strategic Plan
- Nutrition Advisory Committee
- Healthy Food Guide
- Entrepreneurship
- Tufts Nutrition Council
- Read About Research Activities
- Alumni & Friends at Friedman
- Make a Gift
- Virginia and Dr. Elie J. Baghdady Fund
News & Media
- News & Press Releases
- Video Gallery
- Media Inquiries
- Broadcast Studio Facilities
- Web, Social Media, and Communications
How Are We Making an Impact?
The Friedman School pursues cutting-edge research and education from cell to society, including in molecular nutrition, human metabolism, population studies, clinical trials, nutrition interventions and behavior change, communication, food systems and sustainability, global food insecurity, humanitarian crises, and food economics and policy.
- Food and Nutrition Innovation Institute
Nutrition Publications - Friedman School & HNRCA
- Tufts Nutrition Magazine
- Tufts Health & Nutrition Newsletter
- MyPlate for Older Adults

- Speakers Series
Friedman School Community at ASN 2024

NUTRITION 2024 will bring together thousands of experts from around the globe to share and discuss emerging scientific and policy developments in food, nutrition and public health June 29–July 2 in Chicago. You can view the full meeting schedule here .
Here are the Friedman School's faculty, staff, and students* who will be presenting at this year's conference (list subject to change):
*This schedule only notes Friedman-affiliated presenters, authors, and co-authors. Much of this research has occurred in collaboration with folks outside of our immediate community. For the full schedule and complete listing of everyone affiliated with each paper or presentation, please click on the "Full Schedule" button at the bottom of this page, or explore the corresponding link for each schedule item. All times are noted in CT.
Saturday, June 29
Sunday, june 30, monday, july 1, tuesday, july 2.
View the Full Schedule
IMAGES
VIDEO
COMMENTS
3. Boosts your immune system. You need a healthy immune system to fight off illnesses, from colds and flu to cancer. And vitamin E plays a vital role in your immune health. " Studies have shown ...
Vitamin E or tocopherol is a fat-soluble vitamin that functions as an antioxidant, protecting the cell membrane. As with all vitamins, the body does not form vitamin E. It solely forms from the photosynthetic processes of plants and therefore must be consumed from outside sources in small quantities. Vitamin E is a medication used to manage and treat vitamin E deficiency states and disease ...
Vitamin E is the collective name for a group of fat-soluble compounds with distinctive antioxidant activities . Naturally occurring vitamin E exists in eight chemical forms (alpha-, beta-, gamma-, and delta-tocopherol and alpha-, beta-, gamma-, and delta-tocotrienol) that have varying levels of biological activity . Alpha- (or α-) tocopherol ...
Vitamin E. Vitamin E is a fat-soluble vitamin with several forms, but alpha-tocopherol is the only one used by the human body. Its main role is to act as an antioxidant, scavenging loose electrons—so-called "free radicals"—that can damage cells. [1] It also enhances immune function and prevents clots from forming in heart arteries.
Vitamin E is a group of eight fat soluble compounds that include four tocopherols and four tocotrienols. Vitamin E deficiency, which is rare and usually due to an underlying problem with digesting dietary fat rather than from a diet low in vitamin E, can cause nerve problems. Vitamin E is a fat-soluble antioxidant which may help protect cell membranes from reactive oxygen species.
Vitamin E is a fat-soluble compound and protects cell membranes from oxidation and destruction. In 1922, Evans and Bishop discovered that rats fed a lard-based diet developed infertility, suggesting a dietary deficiency [ 1 ]. The fertility was corrected when a lipid extract of cereals was added to the diet; this was termed the "anti-sterility ...
Vitamin E is a nutrient that's important to vision, reproduction, and the health of your blood, brain and skin. Vitamin E also has antioxidant properties. Antioxidants are substances that might protect your cells against the effects of free radicals — molecules produced when your body breaks down food or is exposed to tobacco smoke and ...
Vitamin E AT A GLANCE Introduction The term vitamin E describes a family of eight related, fat-soluble molecules. Among these, 'alpha-tocopherol' has the highest biological activity and is the most abundant in the human body (1). The name tocopherol derives from the Greek words tocos, meaning childbirth, and pherein, meaning to bring forth.
The form of vitamin E: Although vitamin E sounds like a single substance, it is actually the name of eight related compounds in food, including alpha-tocopherol. Each form has a different potency, or level of activity in the body. Vitamin E from natural sources is commonly listed as d-alpha-tocopherol on food packaging and supplement labels.
Vitamin E, or alpha-tocopherol, is a fat-soluble vitamin that acts as a powerful antioxidant to protect cells from free radical damage and is involved in immune function. It's an essential vitamin and must be found in your diet. Vitamin E is important for your brain, eyes, immune system, and heart health. The nutrient may prevent heart disease ...
HPLC conditions for vitamin E analysis have been summarized in several reviews. 46,47,49,50 Vitamin E and products are obtained from natural products, food matrices, and biological samples by direct extraction, solid-phase extraction, and saponification. Care should be taken to avoid artifactual oxidation and decomposition during preparation of ...
Vitamin E is all the following eight compounds alpha, beta, gamma, and delta-tocopherol and alpha, beta, gamma, and delta-tocotrienol. Alpha-tocopherol is the only compound of the eight that are known to meet human dietary needs. All of the vitamin E forms are absorbed in the small intestine, and then the liver metabolizes only alpha-tocopherol. The liver then removes and excretes the ...
Query 9.2.11 9.2. 11. High levels of vitamin E intake do not result in a noted toxicity. However, higher levels of intake of alpha-tocopherol (like achieved by taking supplements) are associated with decreased blood coagulation. In particular, hemorrhagic stroke has been linked to high alpha-tocopherol intake levels.
V itamin E is the collective term given to a group of fat-soluble compounds first discovered in 1922 by Evans and Bishop; these compounds have distinct antioxidant activities essential for health.1 Vitamin E is present in fat-containing foods2 and, as the fat-soluble property of the vitamin allows it to be stored within the fatty tissues of animals and humans, it does not have to be consumed ...
The UL for vitamin E is set at 1,500 international units for adults. There is some evidence that taking vitamin E supplements at high doses has negative effects on health. As mentioned, vitamin E inhibits blood clotting and a few clinical trials have found that people taking vitamin E supplements have an increased risk of stroke.
Chemical nature: Vitamin E is chemically known as tocopherol (Greek: tocos=childbirth, piro=to bear and ol=alcohol) • An alcohol was capable to prevent reproductive failure in animals • Hence it is known as anti-sterility vitamin • Chemistry: • Vitamin E is the name given to group of tocopherols and tocotrienols
Vitamin E refers to the plant-derived, lipid-soluble antioxidants: tocopherols and tocotrienols. They terminate the chain reaction of lipid peroxidation. Vitamin E biological activity is different from its antioxidant activity, and there is a preference for α-tocopherol. This preference is achieved through the selective degradation and excretion of other vitamin E forms and the selective ...
All structures of vitamin E molecules feature a chromanol ring with a side chain located at the C 2‐position (Niki & Abe, 2019). There are eight different natural isoforms exhibiting vitamin E activity; however, external stress such as light may cause oxidation of the reactive groups leading to a potential loss of vitamin E activity. While
Vitamin E (tocopherols and tocotrienols) has demonstrated significant biological effects on enhancing human health and play a promising role in food systems. Studies have shown the relative antioxidant activity of vitamin E contributes to food preservation. It can reduce the negative impact of chemical reactions on food systems by improving their safety, nutritional value, and shelf-life. This ...
Vitamin E - Download as a PDF or view online for free. 12. • Stabilize reactions or situations that typically produce free radicals • Required for Proper Hair Growth (Beauty Vitamin along with BIOTIN) • Preserves & maintains germinal epithelium of gonads. • Required for cellular respiration. • Optimal absorption amino acids.
Presentation Transcript. Vitamin E Composition • Composed of 8 compounds (vitamers) divided into two classes: • Tocopherols: • which have saturated side chains with 16 carbons • Tocotrienols: • which have unsaturated side chains with 16 carbons • Each class is composed of 4 vitamers that differ in the # and location of methyl groups ...
Absorption. 10-33% of deuterium labelled vitamin E is absorbed in the small intestine 5,15.Absorption of Vitamin E is dependant upon absorption of the fat in which it is dissolved 15,1.For patients with poor fat absorption, a water soluble form of vitamin E may need to be substituted such as tocopheryl polyethylene glycol-1000 succinate 15.. In other studies the oral bioavailability of alpha ...
Research shows that vitamin E is one such nutrient that a whopping 88.5% of Americans aren't getting enough of naturally. That's especially worrisome considering some controversy exists in the ...
Pregnant women (n = 1300) were randomized into 5 groups: placebo, or vitamin D 4200 IU/week, 16 800 IU/week, or 28 000 IU/week from second trimester to delivery and placebo until 6 months postpartum; or 28 000 IU/week prenatally and until 6 months postpartum.Infants underwent biochemical rickets screening from 6 to 12 months of age (n = 790).Relative risks (RR) and 95% confidence intervals (95 ...
Vitamin E is a group of antioxidant fat-soluble micronutrients (α-, γ-, δ-, β-tocotrienol and α-, γ-, δ-, β-tocopherol) that is found in high amounts (>10 mg per 100 mL or 100 mg) in nuts, seeds and vegetable oil . It has been reported that consuming 1.5 ounces of almonds or hazelnuts may provide up to approximately 75% of the ...
Date Time Name Co-Authors Presentation Title and Type; 7/1: 11:45AM-1:45PM. Kelly C. Cara, PhD. Tammy M. Scott, Paul F. Jacques, Mei Chung. Long-Term Adherence to a Healthy Diet and Plant-Based Dietary Patterns in Relation to Cognitive Reserve in the 1946 British Birth Cohort: A Cross-Sectional Analysis (Poster Session Group: Dietary Patterns)